Department of Biochemistry, Faculty of Science, King Abdulaziz
University Jeddah 21589, Saudi Arabia.
Corresponding author email: maaalghamdi3@kau.edu.sa
Article Publishing History
Received: 06/07/2021
Accepted After Revision: 23/09/2021
Vitamin D is synthesized by human skin cells exposed to sunlight and also obtained from nutritional sources. It has dual nature and serves as a vitamin and an immunomodulatory hormone. Metabolically, vitamin D is responsible for calcium and phosphate homeostasis, bone resorption, and maintenance of a healthy and mineralized skeleton. As a hormone, its activated form (1,25-dihydroxyvitamin D), binds with the vitamin D receptor (VDR), triggers the regulation of more than 100 genes, many of those associated with the immune system, Hence, it plays a critical role in the regulation of the key components of both, the innate and adaptive immune systems. Deficiency of 25-hydroxyvitamin D has been linked with an increased risk of autoimmune and respiratory diseases such as rheumatoid arthritis, type 1 diabetes, multiple sclerosis, tuberculosis, and influenza.
Recent pharmacogenomic studies have shown that variation in vitamin D receptor gene expression alters the response of different individuals to treatment with vitamin D. Introduction of vitamin D promotes the synthesis of antimicrobial and antiviral proteins in the cell and improves the cellular levels of calcium and phosphorus, eventually promotes autophagy to remove viruses and bacteria from the cells. This review specifically aims at establishing a concrete relationship between vitamin D deficiency and increased susceptibility to various respiratory diseases. We also aimed to explore the possibility of using vitamin D supplementation programs to improve immunoprotection in individuals prone to respiratory illnesses.
Vitamin D, Respiratory Illness, Immunoprotection, Pharmacogenomics, Supplementation
Al-Ghamdi M. A. Vitamin D Supplementation Can Prevent and Treat Multiple Types of Respiratory Illness – An Updated Review. Biosc.Biotech.Res.Comm. 2021;14(3).
Al-Ghamdi M. A. Vitamin D Supplementation Can Prevent and Treat Multiple Types of Respiratory Illness – An Updated Review. Biosc.Biotech.Res.Comm. 2021;14(3). Available from: <a href=”https://bit.ly/3lU7rZw“>https://bit.ly/3lU7rZw</a>
Copyright ©Al-Ghamdi This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-BY) https://creativecommns.org/licenses/by/4.0/, which permits unrestricted use distribution and reproduction in any medium, provide the original author and source are credited.
INTRODUCTION
Vitamin D is one of the four fat-soluble vitamins which are required for the general physiology of human body. Vitamin D is found naturally in some food materials, added as nutritional supplements with calcium and phosphorous (Lamberg-Allardt, 2006; Bruins and Létinois, 2021). However, the major contribution of vitamin D is by photosynthesis in the human skin exposed to ultraviolet B radiations (UVB) (Oonincx et al., 2018). Physiologically, vitamin D, functions as a vitamin and a hormone, it is responsible for the homeostasis of calcium and phosphorous in the human body, bone formation, health and functions (Ono-Ohmachi et al., 2021).
Vitamin D is obtained or synthesized in 2 natural forms including vitamin D2 and vitamin D3, both types are inactive. After synthesis in the skin from dietary cholesterol in the skin cells exposed to UVB, the cholecalciferol enters blood stream, it is subsequently activated in the liver and kidneys to active form of vitamin D known as calcitriol or 1,25-(OH) 2 D (Panfili et al., 2021).
Calcium and phosphorous homeostasis is considered as one of the main functions of vitamin. It promotes the bone resorption by increasing the calcium absorption resulting the better bone structure and physiology (Hanel and Carlberg, 2020). Supplementary intake of vitamin D has been reported to decrease the chances of many diseases including hypertension, osteoporosis, cancer, and many autoimmune diseases. Vitamin D serves to strengthen the innate and adoptive immune systems by increasing the number and activity of cells and proteins associated with the immune response (Gilani et al., 2021).
The vitamin D receptor (VDR) that interacts with vitamin D is present in most of the body cells and tissues. The interaction of vitamin D with its corresponding receptor as a hormone triggers the regulation of 100s of genes. Most of the regulated genes are involved in the promotion of innate and adoptive immune systems.
These findings suggest the hypothesis that vitamin D can play a crucial role in strengthen the immune response against bacterial and viral infections such as influenza, pneumonia and respiratory diseases. Vitamin D supplements are especially recommended to boost the components of immune system against such disease. It also leads to the hypothesis about the vital role of vitamin D against the severity and mortality of diseases (Giménez et al., 2021).
Looking at the important role of vitamin D as a protective agent and in the treatment of many virus and bacteria, based respiratory infections; we have aimed to conduct a review article representing the association of vitamin D deficiency with the onset and mortality rates of a few respiratory diseases including influenza, COVID-19, tuberculosis and pneumonia.
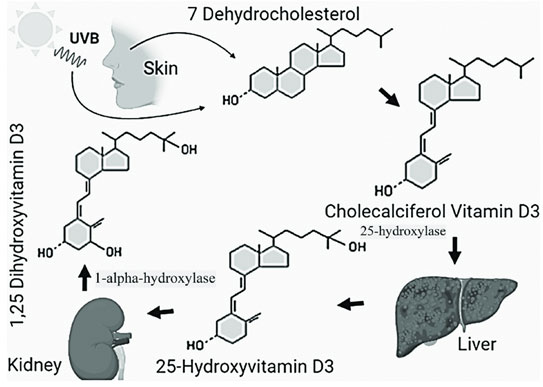
Synthesis and metabolism of vitamin D: In the human body, diet and photosynthesis in the skin provide all the vitamin D required for the better physiology. The pigmented substance melanin absorbs UVB from sunlight that interacts with 7-dihydrocholesterol, and synthesize vitamin D. The vitamin D3 produced by photosynthesis is an inactive compound that needs hydroxylations in the liver and kidneys to produce an active form of vitamin known as 1,25 dihydroxyvitamin D or calcidiol.
The reaction to activate vitamin D is calalyzed by the enzyme 1-α-hydroxylase (CYP27B1). The active form of hormone also interacts with the interstinal cells to stimulate calcium reabsorption, to promote osteoblast differentiation and matrix calcification. After its utilization the 1,25-OH-D form is metabolized to the 1,24,25-OH vitamin D by 24-hydroxylase (CYP24) (Khairy et al., 2021).
The binding interaction of active vitamin D with its relevant receptor (VDR) regulates the genes associated with the vitamin D-VDR combination (Marozik et al., 2021). The synthesis and activation of vitamin D has been described in the Figure 1.
Figure 1: A schematic representation of synthesis and activation of vitamin
D in the human body (adopted from Gilani et al., 2021)
Vitamin D and immunity: The immune system provides a defense against the invading pathogens, microbes, viruses and unwanted hazardous bodies or substances. It helps in the maintenance of healthy status of body by protecting against diseases. Recently, the vitamin D has been well implicated with the human immune system. Vitamin D serves as the promoter of immune system and its deficiency leads to an increased susceptibility, increased severity and mortality by many infectious diseases (Carpagnano et al., 2021).
The immune system consists of a set of cells, with receptors and soluble proteins. All of these components of immune system are affected, either individually or in the form of a signaling cascade by the deficiency of vitamin D. As for example, vitamin D inhibits the proliferation of beta cells, blocks B cell immunoglobulin secretion by these cells (Bui et al., 2021).
Vitamin D promotes the shift of Th1 to Th2 cells as a suppressor of T cell proliferation (Laird et al., 2020). It also helps in the maturation of T cells by twisting them away from Th17 phenotype that has inflammatory effects, and triggers the formation of T regulatory cells (Fakhoury et al., 2020). All these activities result in the reduced production of IL-17 and IL-21 cytokines that have inflammatory impact, and enhance the production of IL-10 cytokines that have been associated with anti-inflammatory response of cells (Leal et al., 2020).
The physiology of dendritic cells (DCs) and monocytes is also regulated by vitamin D by an inhibition in the production of inflammatory cytokines by monocyte such as TNFα, IL-1, IL-6, IL-8, and IL-12 (Nastri et al., 2020). Differentiation, maturation, and preservation of cellular phenotypes are inhibited by a reducing the expression of co-stimulatory molecules, MHC class II molecules, and IL12 (Aygun et al., 2020). The deficiency of vitamin D has also been associated with the onset of autoimmune diseases. In such diseases, vitamin D has found to have an ameliorative effect indicating the beneficial role of vitamin D supplements.
Vitamin D and respiratory diseases: In context with the available information about the role of vitamin D on the calcium homeostasis, bone formation, bone health and strengthening of immune system, the present review article aims at highlighting the possible correlation between vitamin D levels and susceptibility to respiratory disease.
Vitamin D and tuberculosis: Tuberculosis (TB) caused by Mycobacterium tuberculosis (MTB) is an infectious disease that spreads by aerosols. The disease generally affects respiratory system, especially the lungs, it can also damage other parts of body. The disease is associated with poor living conditions, and prevalent worldwide, causing more than 2 million deaths every year. Deficiency of vitamin D has been linked with the spread of infection in the human body, its severity and mortality.
Level of vitamin D has also been associated with the successful treatment and time of recovery. The genetic variability can also affect the level of susceptibility for infection among the world populations. may influence host susceptibility to developing active tuberculosis and treatment response (Ganmaa et al., 2020).
A study from Pakistani populations has shown that the low levels of vitamin D has been found to increase the risk of tuberculosis infections by 5-times than those having normal levels of plasma vitamin D levels (Jaimni et al., 2021). Vitamin D deficient populations have risk of rapid spread of disease among healthy individuals. One of the similar studies has shown that the African populations migrated to Australia with low levels of vitamin D had high probability of tuberculosis infections than those with normal vitamin D levels (Acen et al., 2021). The findings from other studies have shown a rapid spread and progression of infection among the people with low levels of vitamin D (Faniyi et al., 2021).
The mechanism adopted by vitamin D to prevent the onset of infection or to inhibit the rapid progression of disease has been clearly described. According to the findings, vitamin D limits the Mycobacterium tuberculosis infection by binding to the VDR receptor, later is a polymorphic nuclear receptor responsible to manage the regulation of many genes for their expression. Most of these genes are involved in the strengthening of human immune system by regulation of the production of cytokines (Bishop et al., 2021).
VDR is found in almost all types of cells and it is up regulated by specific toll–like receptors. The receptor (VDR) is essential component of immune cells, and cells of pulmonary epithelial walls. The vitamin D based mechanism is recognized for the production of many antimicrobial proteins including cathelicidin LL-37 and β defensin (Acen et al., 2021). The mechanism is also responsible to suppress the activity of metalloproteinase enzymes to prevent the degradation of extracellular matrix of pulmonary tissues (Sutaria et al., 2014; Meca et al., 2021).
Vitamin D status has been found to be affected by many variants of VDR in the cells (Le Pavec et al., 2008). The difference of vitamin D levels in the populations from different geographic areas and with different ethnicity have also found to affect the susceptibility to disease and resistance of bacteria to the drugs (Griffin et al., 2021). Many studies from Ethiopia, Tanzania, Uganda and other countries have positively correlated the vitamin D deficiency with the onset, spread and mortality rate due to tuberculosis (Jovanovich et al., 2014).
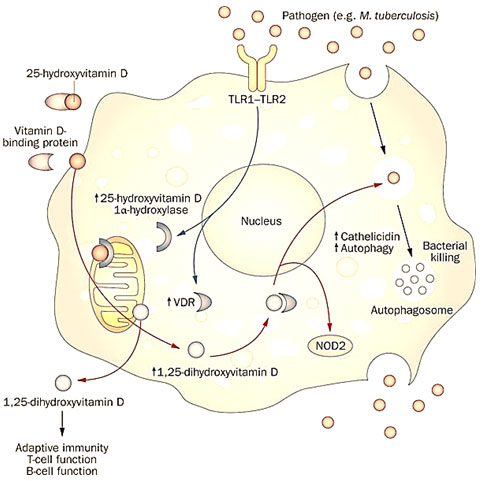
These investigations have also found that the low BMI has also been associated with the deficiency of vitamin D and both have been associated with the onset of TB (Rhodes et al., 2021; Lungu et al., 2021). Trials based on vitamin D supplementation have also shown an improvement of human immunity against tuberculosis (Xiong et al., 2021). A vitamin D based mechanism involved in the in the autophagy and removal of M. tuberculosis has been described (Figure 2).
Figure 2: The TLR receptors interact with pathogen (M. tuberculosis) and results in the induction of transcrption of genes coding for vitamin D receptor (VDR), the enzyme responsible to activate vitamon D named 25-hydroxyvitamin D-1α-hydroxylase, upregulating the expression of these genes. Once the vitamin D enters a monocyte with the help of vitamin D binding protein (DBP), the vitamin gets activated, by mitochondrial 25-H-D-1α-hydroxylase and subsequently binds with the VDR. The vitamin-VDR binding triggers the upregulation of many proteins including cathelicidin, intracellular pathogen recognition receptor NOD2 and defensin beta 2 protein. These proteins and enzymes promote autophagy and clearance of bactria from the cells (adopted from Liu et al., 2006).
Vitamin D and pneumonia: Pneumonia is the infection of alveolisacs of respiratory tract. The main signs and symptoms include dry, productive cough or combination of both, difficulty in breathing, chest pain and fever. The headache and body ache are also observed as common symptoms, but these are common with many other conditions. The intensity and severity of symptoms variable depending upon the human immune response and degree of infection (Jovanovich et al., 2014). The causative agents of disease can be usually a virus, bacteria or other microorganisms.
Pneumonia can be hospital-acquired, community-associated, and healthcare-associated depending upon the site of infection. Smoking history, sickle cell disease, chronic obstructive pulmonary disease (COPD), asthma, cystic fibrosis,heart failure, diabetes, weak immune system, and poor ability to cough are common risk factors of pneumonia (Zhou et al., 2019).
Recently, there has been sufficient evidence indicating the association of vitamin D deficiency with the community-acquired pneumonia (CAP) (Bergman et al., 2013), it resulted in the extensive research on the applications of vitamin D on the human defense mechanisms and immune responses (Camargo et al., 2011). It has been reported by many studies that the blood levels of vitamin D < 37 nmol/L has been associated to an increase in the susceptibility and severity of disease (Hashemian and Heidarzadeh, 2017; Oktaria et al., 2021).
The studies including 5660 individuals of all age limits, investigated in 11 randomized placebo-controlled trial have shown a significant decrease in the risk of respiratory diseases especially pneumonia in case of vitamin D supplementation (Oktaria et al., 2021a; Labib et al., 2021). The populations with low vitamin D levels have significantly higher (2.5 times) risk of contracting pneumonia as compared to those with normal levels of vitamin.
Low levels of vitamin D in the umbilical cord has been linked with the high risk of respiratory infections in the new borns in the early 3 years of their life childhood (Oktaria et al., 2021 b). A direct relationship has been reported between the vitamin D levels among children and onset of pneumonia (Leow et al., 2011). The normal levels of vitamin D has shown a preventive role against all kinds of pneumonia among the age groups of 24 to 60 months (Chowdhury et al., 2021), similar findings have been reported by a study in Bangladeshi children of 1 to 18 months age group.
According to many studies, the infection leads to the synthesis of antimicrobial proteins and peptides in the mucosal and epithelial surface cells in multicellular organisms. These molecules or peptides serve as the first line of defense against viral or bacterial infections. Some of these peptides have a role in the modulation of immune responses. Defensins and cathelicidins are the most widely studied proteins that are responsible to fight against pneumonia infections (Aygun et al., 2020).
The mechanism followed by the defense system is similar to that described in the figure 2. In short, the TLRs activate the defense cells, subsequent upregulation of vitamin D receptor and CYP27B1 enzyme. The enzyme is also associated with the conversion of 25-hydroxyvitamin D to 1,25- dihydroxyvitamin D, the latter being an active form of vitamin D (Parsanathan and Jain, 2019; Campolina-Silva et al., 2021).
Vitamin D and influenza: Influenza, is a respiratory infectious disease also known as flu or common cold. The causative agent of is a virus known as influenza virus. The complicated forms of influenza are known as viral pneumonia, sinus infections, if the infection is caused by bacteria, it is also named as secondary bacterial pneumonia. The disease is associated with worsening of existing respiratory problems including heart diseases and asthma. With more than 290,000 infections and about 650,000 annual deaths, the disease is found worldwide, especially common during winters (Goncalves-Mendes et al., 2019).
Vaccine is available against influenza, but the whole world population is not vaccinated yet. According to the estimates, about 10% unvaccinated adults and 20% unvaccinated children are infected every year (Martineau et al., 2017; Pham et al., 2021). In the northern and opposite hemispheres, the infection occurs mostly in winters. However, in the rest of the world and near to the equator, the outbreaks can be observed at any time of the year (Zhou et al/. 2018; Goncalves-Mendes et al., 2019).
Very young, old populations and those with existing respiratory and heart diseases are populations at high death risk by influenza. As the antiviral medicines and vaccines are limited in availability and efficacy against influenza, non-pharmaceutical interventions including herbal medications and supplements of immune boosting vitamins and minerals are essential to control the spread and severity of infection. By stimulating the naturally produced antimicrobial proteins and peptides, vitamin D serves as an important promoter of innate and adoptive immune systems that lead to the destruction of invading pathogens (Chung et al., 2020; Bleakley et al., 2021).
Particularly, in the cell lining of upper and lower respiratory tract, these peptides and proteins are able to fight the viruses and bacteria directly. Vitamin D is responsible to shift the Th1 (T helper 1) to Th2-mediated cells in their response, and reduce the inflammatory responses (Briceno Noriega and Savelkoul, 2021). This results in the suppression of major symptoms of common cold or flu. Vaccination is often recommended to fight against flu infections.
However, the vaccines have very low (17–53%) efficacy in old people and 70–90% among the young adults. Vitamin D has been also reported to increase the levels of TGFβ in response to influenza vaccination and promote the defense mechanisms (Singh et al., 2020). Also, the populations subjected to vitamin D supplementation along with vaccination have shown high levels of protection against flu as compared to those with vaccination and no vitamin D supplements (Jolliffe et al., 2021).
Studies on infants have shown that the high dose with up to 1200IU per day of vitamin D has proven significantly useful in the prevention against seasonal influenza, rapid decrease in viral load, decreased intensity of symptoms and early recovery. The high dose was found safe for children (Abioye et al., 2021). Less or unavailability of sun light has been linked to the deficiency of vitamin D and consequently the susceptibility to influenza. Vitamin D supplementation is therefore, recommended in that particular season or areas (Urashima et al., 2010; Ma et al., 2021).
Studies involving 11,000 participants of all age groups (0 and 95 years), has shown that the daily dose of vitamin D reduced the frequency of flu infections and supported the general health of respiratory tract. As described in the previous two sections, vitamin D activates the synthesis of antimicrobial peptides, strengthens the immune system and improves the immune responses by significantly lowering the inflammatory events of infection process.
Vitamin D and COVID 19: The world population is threatened by coronavirus disease 19 (COVID-19) that is a respiratory infection with high rate of transmission and severe health consequences. The disease is caused by a zoonotically transmitted virus known as SARS-CoV-2. The disease started in December 2019 from Chinese city Wuhan (WHO, 2020) and spread all over the globe very rapidly. SARS-CoV-2 has more than 80% genome similarity with the causative agent of recent coronavirus disease in the last decade (2003-2004) (Rajapakse and Dixit, 2021).
There is no specific cure for the COVID-19 and only protective and supportive managements are being conducted. Most of the deaths caused by COVID-19 are due to acute respiratory distress syndrome (ARDS) and respiratory failure and multiorgan failure. Vaccination has been initiated in many countries in the recent times. However, the efficacy of these vaccines is still under question. Moreover, the demand for the vaccines is very high, especially in third world countries which neither have the technical know how to produce them nor the economic means to procure them. In the wake of this situation, it would be interesting to probe the association between vitamin D deficiency and susceptibility to COVID-19 as well as recovery rate.
In COVID-19 patients the presence of pneumonia/acute respiratory distress syndrome (ARDS), microvascular thrombosis and/or cytokine storm, myocarditis, all of which involve underlying inflammation are main indicators of disease severity. While the COVID-19-specific CD8 T cells and the specific antibodies produced by B cells are critical for eliminating the virus, uncontrolled non-specific inflammation and cytokine release can cause catastrophic injury to the lungs and other vital organs. Consequently, decreasing this early non-specific inflammation during COVID-19 may provide time for the development of specific acquired immunity against COVID-19 (Nadeem et al., 2020).
T regulatory lymphocytes (Tregs), are responsible to provide a principal defense line against high intensity inflammatory response in vital infections. The levels of Tregs have been reported to be low in one group of COVID-19 patients, and ‘markedly lower in severe cases (Leila et al., 2020; Weir et al., 2020). In a study of older nursing home patients, high Treg blood levels were found to be associated with a reduced level of respiratory viral disease. These observations suggest that if Treg levels can be increased, this might be of benefit in diminishing the severity of viral disease and perhaps of COVID-19. Treg levels can be increased by vitamin D supplementation (Ali, 2020; Gilani et al., 2021).
One of the major devastating effects on immune system produced by covid 19 is the cytokine storm that leads to rapid deterioration of lung cells. It is a well-known fact that vitamin D is capable of reducing the inflammatory cytokine production. A study of healthy women in the USA found a significant inverse relationship between the serum levels of 25(OH)D and TNF-alpha (Khemka et al., 2020). Thrombotic complications are common in COVID-19 patients. Of those with severe disease, over half have been found to have elevated D-dimer levels.
Interestingly, vitamin D is also involved in the regulation of thrombotic pathways, and vitamin D deficiency is associated with an increase in thrombotic episodes (Mohan et al., 2020; Gilani et al., 2021). An increased risk of death with COVID-19 is also observed in black, Asian and minority ethnic (BAME) groups. As melanin reduces the production of vitamin D asociated with exposure to the ultraviolet radiation in sunlight, this may help to explain the observed frequent occurrence of vitamin D deficiency in BAME groups.
CONCLUSION
Vitamin D, one of the fat-soluble vitamins has been reviewed for its association with the onset and severity of respiratory diseases. Vitamin D serves as a double-edged sword, one one hand it operates as an immunomodulator and on the other side it promotes autophagy to remove the pathogenic viruses and bacteria from the cells. It influences both the innate and adaptive immune systems, and reduces inflammatory cytokines. The molecular pathways of these immunomodulatory effects have been well established, thereby making Vitamin D and important candidate for development of therapeutic as well as prophylactic applications against various infectious diseases.
REFERENCES
Abioye, A.I., Bromage, S. and Fawzi, W., (2021). Effect of micronutrient supplements on influenza and other respiratory tract infections among adults: a systematic review and meta-analysis. BMJ Global Health, 6(1), p.e003176.
Acen, E.L., Biraro, I.A., Worodria, W., Joloba, M.L., Nkeeto, B., Musaazi, J. and Kateete, D.P., (2021). Impact of vitamin D status and cathelicidin antimicrobial peptide on adults with active pulmonary TB globally: A systematic review and meta-analysis. PloS one, 16(6), p.e0252762.
Ali, N., (2020). Role of vitamin D in preventing of COVID-19 infection, progression and severity. Journal of infection and public health, 13(10), pp.1373-1380.
Aygun, H., (2020). Vitamin D can prevent COVID-19 infection-induced multiple organ damage. Naunyn-schmiedeberg’s Archives of Pharmacology, 393(7), pp.1157-1160.
Aygun, H., (2020). Vitamin D can prevent COVID-19 infection-induced multiple organ damage. Naunyn-schmiedeberg’s Archives of Pharmacology, 393(7), pp.1157-1160.
Bergman, P., Lindh, Å.U., Björkhem-Bergman, L. and Lindh, J.D., (2013). Vitamin D and respiratory tract infections: a systematic review and meta-analysis of randomized controlled trials. PloS one, 8(6), p.e65835.
Bleakley, A.S., Licciardi, P.V. and Binks, M.J., (2021). Vitamin D Modulation of the Innate Immune Response to Paediatric Respiratory Pathogens Associated with Acute Lower Respiratory Infections. Nutrients, 13(1), p.276.
Briceno Noriega, D. and Savelkoul, H.F., (2021). Vitamin D and allergy susceptibility during gestation and early life. Nutrients, 13(3), p.1015.
Bruins, M.J. and Létinois, U., (2021). Adequate Vitamin D Intake Cannot Be Achieved within Carbon Emission Limits Unless Food Is Fortified: A Simulation Study. Nutrients, 13(2), p.592.
Bui, L., Zhu, Z., Hawkins, S., Cortez-Resendiz, A. and Bellon, A., (2021). Vitamin D regulation of the immune system and its implications for COVID-19: A mini review. SAGE Open Medicine, 9, p.20503121211014073.
Camargo, C.A., Ingham, T., Wickens, K., Thadhani, R., Silvers, K.M., Epton, M.J., Town, G.I., Pattemore, P.K., Espinola, J.A., Crane, J. and New Zealand Asthma and Allergy Cohort Study Group, (2011). Cord-blood 25-hydroxyvitamin D levels and risk of respiratory infection, wheezing, and asthma. Pediatrics, 127(1), pp. e180-e187.
Campolina-Silva, G.H., Barata, M.C., Werneck-Gomes, H., Maria, B.T., Mahecha, G.A.B., Belleannée, C. and Oliveira, C.A., (2021). Altered expression of the vitamin D metabolizing enzymes CYP27B1 and CYP24A1 under the context of prostate aging and pathologies. The Journal of Steroid Biochemistry and Molecular Biology, 209, p.105832.
Carpagnano, G.E., Di Lecce, V., Quaranta, V.N., Zito, A., Buonamico, E., Capozza, E., Palumbo, A., Di Gioia, G., Valerio, V.N. and Resta, O., (2021). Vitamin D deficiency as a predictor of poor prognosis in patients with acute respiratory failure due to COVID-19. Journal of endocrinological investigation, 44(4), pp.765-771.
Chowdhury, F., Shahid, A.S.M.S.B., Tabassum, M., Parvin, I., Ghosh, P.K., Hossain, M.I., Alam, N.H., Faruque, A.S.G., Huq, S., Shahrin, L. and Homaira, N., (2021). Vitamin D supplementation among Bangladeshi children under-five years of age hospitalised for severe pneumonia: A randomised placebo-controlled trial. PloS one, 16(2), p.e0246460.
Chung, C., Silwal, P., Kim, I., Modlin, R.L. and Jo, E.K., (2020). Vitamin D-cathelicidin axis: at the crossroads between protective immunity and pathological inflammation during infection. Immune network, 20(2).
Fakhoury, H.M., Kvietys, P.R., AlKattan, W., Al Anouti, F., Elahi, M.A., Karras, S.N. and Grant, W.B., (2020). Vitamin D and intestinal homeostasis: Barrier, microbiota, and immune modulation. The Journal of steroid biochemistry and molecular biology, 200, p.105663.
Faniyi, A.A., Lugg, S.T., Faustini, S.E., Webster, C., Duffy, J.E., Hewison, M., Shields, A., Nightingale, P., Richter, A.G. and Thickett, D.R., (2021). Vitamin D status and seroconversion for COVID-19 in UK healthcare workers. European Respiratory Journal, 57(4).
Ganmaa, D., Uyanga, B., Zhou, X., Gantsetseg, G., Delgerekh, B., Enkhmaa, D., Khulan, D., Ariunzaya, S., Sumiya, E., Bolortuya, B. and Yanjmaa, J., (2020). Vitamin D supplements for prevention of tuberculosis infection and disease. New England Journal of Medicine, 383(4), pp.359-368.
Gilani, S.J., Bin-Jumah, M., Nadeem, M.S. and Kazmi, I., (2021). Vitamin D attenuates COVID-19 complications via modulation of proinflammatory cytokines, antiviral proteins, and autophagy. Expert Review of Anti-infective Therapy, (just-accepted).
Giménez, V.M.M., Inserra, F., Ferder, L., García, J. and Manucha, W., (2021). Vitamin D deficiency in African Americans is associated with a high risk of severe disease and mortality by SARS-CoV-2. Journal of Human Hypertension, 35(4), pp.378-380.
Goncalves-Mendes, N., Talvas, J., Dualé, C., Guttmann, A., Corbin, V., Marceau, G., Sapin, V., Brachet, P., Evrard, B., Laurichesse, H. and Vasson, M.P., (2019). Impact of vitamin D supplementation on influenza vaccine response and immune functions in deficient elderly persons: a randomized placebo-controlled trial. Frontiers in immunology, 10, p.65.
Griffin, G., Hewison, M., Hopkin, J., Kenny, R.A., Quinton, R., Rhodes, J., Subramanian, S. and Thickett, D., (2021). Perspective: Vitamin D supplementation prevents rickets and acute respiratory infections when given as daily maintenance but not as intermittent bolus: implications for COVID-19. Clinical Medicine, 21(2), p.e144.
Hanel, A. and Carlberg, C., (2020). Vitamin D and evolution: Pharmacologic implications. Biochemical pharmacology, 173, p.113595.
Hashemian, H. and Heidarzadeh, A., (2017). Role of Vitamin D [25 (OH) D] deficiency in development of pneumonia in children. Archives of Pediatric Infectious Diseases, 5(3).
Jaimni, V., Shasty, B.A., Madhyastha, S.P., Shetty, G.V., Acharya, R.V., Bekur, R. and Doddamani, A., (2021). Association of Vitamin D Deficiency and Newly Diagnosed Pulmonary Tuberculosis. Pulmonary Medicine, 2021.
Jolliffe, D.A., Camargo Jr, C.A., Sluyter, J.D., Aglipay, M., Aloia, J.F., Ganmaa, D., Bergman, P., Bischoff-Ferrari, H.A., Borzutzky, A., Damsgaard, C.T. and Dubnov-Raz, G., (2021). Vitamin D supplementation to prevent acute respiratory infections: a systematic review and meta-analysis of aggregate data from randomised controlled trials. The Lancet Diabetes & Endocrinology.
Jovanovich, A.J., Ginde, A.A., Holmen, J., Jablonski, K., Allyn, R.L., Kendrick, J. and Chonchol, M., (2014). Vitamin D level and risk of community-acquired pneumonia and sepsis. Nutrients, 6(6), pp.2196-2205.
Khairy, E.Y. and Attia, M.M., (2021). Protective effects of vitamin D on neurophysiologic alterations in brain aging: role of brain-derived neurotrophic factor (BDNF). Nutritional neuroscience, 24(8), pp.650-659.
Khemka, A., Suri, A., Singh, N.K. and Bansal, S.K., (2020). Role of Vitamin D Supplementation in Prevention and Treatment of COVID-19. Indian Journal of Clinical Biochemistry, 35(4), pp.502-503.
L Bishop, E., Ismailova, A., Dimeloe, S., Hewison, M. and White, J.H., (2021). Vitamin D and immune regulation: antibacterial, antiviral, anti‐inflammatory. JBMR plus, 5(1), p.e10405.
Labib, J.R., Ibrahem, S.K., Ismail, M.M., Abd El Fatah, S.A., Sedrak, A.S., Attia, M.A.S., El-Hanafi, H.M. and Kamel, M.H., (2021). Fewer children died of pneumonia after getting 100,000 IU of vitamin D–RCT March 2021. Medicine (Baltimore), 100(13), p.e25011.
Laird, E., Rhodes, J. and Kenny, R.A., (2020). Vitamin D and inflammation: potential implications for severity of Covid-19. Ir Med J, 113(5), p.81.
Lamberg-Allardt, C., (2006). Vitamin D in foods and as supplements. Progress in biophysics and molecular biology, 92(1), pp.33-38.
Le Pavec, J., Souza, R., Herve, P., Lebrec, D., Savale, L., Tcherakian, C., Jaïs, X., Yaïci, A., Humbert, M., Simonneau, G. and Sitbon, O., (2008). Portopulmonary hypertension: survival and prognostic factors. American journal of respiratory and critical care medicine, 178(6), pp.637-643.
Leal, L.K.A.M., Lima, L.A., de Aquino, P.E.A., de Sousa, J.A.C., Gadelha, C.V.J., Calou, I.B.F., Lopes, M.J.P., Lima, F.A.V., Neves, K.R.T., de Andrade, G.M. and de Barros Viana, G.S., (2020). Vitamin D (VD3) antioxidative and anti-inflammatory activities: Peripheral and central effects. European journal of pharmacology, 879, p.173099.
Leila, M. and Sorayya, G., (2020). Genotype and phenotype of COVID-19: Their roles in pathogenesis. Journal of Microbiology, Immunology and Infection, 10.
Leow, L., Simpson, T., Cursons, R., Karalus, N. and Hancox, R.J., (2011). Vitamin D, innate immunity and outcomes in community acquired pneumonia. Respirology, 16(4), pp.611-616.
Liu, P.T., Stenger, S., Li, H., Wenzel, L., Tan, B.H., Krutzik, S.R., Ochoa, M.T., Schauber, J., Wu, K., Meinken, C. and Kamen, D.L., (2006). Toll-like receptor triggering of a vitamin D-mediated human antimicrobial response. Science, 311(5768), pp.1770-1773.
Lungu, P.S., Kilembe, W., Lakhi, S., Sukwa, T., Njelesani, E., Zumla, A.I. and Mwaba, P., (2021). A comparison of vitamin D and cathelicidin (LL-37) levels between patients with active TB and their healthy contacts in a high HIV prevalence setting: a prospective descriptive study. Transactions of The Royal Society of Tropical Medicine and Hygiene.
Ma, H., Zhou, T., Heianza, Y. and Qi, L., (2021). Habitual use of vitamin D supplements and risk of coronavirus disease 2019 (COVID-19) infection: a prospective study in UK Biobank. The American journal of clinical nutrition, 113(5), pp.1275-1281.
Marozik, P., Rudenka, A., Kobets, K. and Rudenka, E., (2021). Vitamin D Status, Bone Mineral Density and VDR Gene Polymorphism in a Cohort of Belarusian Postmenopausal Women. Nutrients, 13(3), p.837.
Martineau, A.R., Jolliffe, D.A., Hooper, R.L., Greenberg, L., Aloia, J.F., Bergman, P., Dubnov-Raz, G., Esposito, S., Ganmaa, D., Ginde, A.A. and Goodall, E.C., (2017). Vitamin D supplementation to prevent acute respiratory tract infections: systematic review and meta-analysis of individual participant data. bmj, 356.
Meca, A.D., Ștefănescu, S., Bogdan, M., Turcu‑Stiolică, A., Nițu, F.M., Matei, M., Cioboată, R., Bugă, A.M. and Pisoschi, C.G., (2021). Crosstalk between vitamin D axis, inflammation and host immunity mechanisms: A prospective study. Experimental and Therapeutic Medicine, 21(6), pp.1-7.
Mohan, M., Cherian, J.J. and Sharma, A., (2020). Exploring links between vitamin D deficiency and COVID-19. PLoS pathogens, 16(9), p.e100887
Nadeem, M.S., Zamzami, M.A., Choudhry, H., Murtaza, B.N., Kazmi, I., Ahmad, H. and Shakoori, A.R., (2020). Origin, potential therapeutic targets and treatment for coronavirus disease (COVID-19). Pathogens, 9(4), p.307.
Nastri, L., Guida, L., Annunziata, M., Ruggiero, N. and Rizzo, A., (2018). Vitamin D modulatory effect on cytokines expression by human gingival fibroblasts and periodontal ligament cells. Minerva stomatologica, 67(3), pp.102-110.
Oktaria, V., Danchin, M., Triasih, R., Soenarto, Y., Bines, J.E., Ponsonby, A.L., Clarke, M.W. and Graham, S.M., (2021). The incidence of acute respiratory infection in Indonesian infants and association with vitamin D deficiency. PloS one, 16(3), p.e0248722.
Oktaria, V., Triasih, R., Graham, S.M., Bines, J.E., Soenarto, Y., Clarke, M.W., Lauda, M. and Danchin, M., (2021). Vitamin D deficiency and severity of pneumonia in Indonesian children. Plos one, 16(7), p.e0254488.
Ono-Ohmachi, A., Ishida, Y., Morita, Y., Kato, K., Yamanaka, H. and Masuyama, R., (2021). Bone mass protective potential mediated by bovine milk basic protein requires normal calcium homeostasis in mice. Nutrition, 91, p.111409.
Oonincx, D.G.A.B., Van Keulen, P., Finke, M.D., Baines, F.M., Vermeulen, M. and Bosch, G., (2018). Evidence of vitamin D synthesis in insects exposed to UVb light. Scientific Reports, 8(1), pp.1-10.
Panfili, F.M., Roversi, M., D’argenio, P., Rossi, P., Cappa, M. and Fintini, D., (2021). Possible role of vitamin D in Covid-19 infection in pediatric population. Journal of endocrinological investigation, 44(1), pp.27-35.
Parsanathan, R. and Jain, S.K., (2019). Glutathione deficiency alters the vitamin D-metabolizing enzymes CYP27B1 and CYP24A1 in human renal proximal tubule epithelial cells and kidney of HFD-fed mice. Free Radical Biology and Medicine, 131, pp.376-381.
Pham, H., Waterhouse, M., Baxter, C., Romero, B.D., McLeod, D.S., Armstrong, B.K., Ebeling, P.R., English, D.R., Hartel, G., Kimlin, M.G. and Martineau, A.R., (2021). The effect of vitamin D supplementation on acute respiratory tract infection in older Australian adults: an analysis of data from the D-Health Trial. The Lancet Diabetes & Endocrinology, 9(2), pp.69-81.
Rajapakse, N. and Dixit, D., (2021). Human and novel coronavirus infections in children: a review. Paediatrics and international child health, 41(1), pp.36-55.
Rhodes, J.M., Subramanian, S., Laird, E., Griffin, G. and Kenny, R.A., (2021). Perspective: Vitamin D deficiency and COVID‐19 severity–plausibly linked by latitude, ethnicity, impacts on cytokines, ACE2 and thrombosis. Journal of internal medicine, 289(1), pp.97-115.
Singh, M., Vaughn, C., Sasaninia, K., Yeh, C., Mehta, D., Khieran, I. and Venketaraman, V., (2020). Understanding the Relationship between Glutathione, TGF-β, and Vitamin D in Combating Mycobacterium tuberculosis Infections. Journal of Clinical Medicine, 9(9), p.2757.
Sutaria, N., Liu, C.T. and Chen, T.C., (2014). Vitamin D status, receptor gene polymorphisms, and supplementation on tuberculosis: a systematic review of case-control studies and randomized controlled trials. Journal of clinical & translational endocrinology, 1(4), pp.151-160.
Urashima, M., Segawa, T., Okazaki, M., Kurihara, M., Wada, Y. and Ida, H., (2010). Randomized trial of vitamin D supplementation to prevent seasonal influenza A in schoolchildren. The American journal of clinical nutrition, 91(5), pp.1255-1260.
Weir, E.K., Thenappan, T., Bhargava, M. and Chen, Y., (2020). Does vitamin D deficiency increase the severity of COVID-19?. Clinical Medicine, 20(4), p.e107.
Xiong, K., Wang, J., Zhang, B., Xu, L., Hu, Y. and Ma, A., (2021). Vitamins A and D fail to protect against tuberculosis-drug-induced liver injury: A post hoc analysis of a previous randomized controlled trial. Nutrition, 86, p.111155.
Zhou, J., Du, J., Huang, L., Wang, Y., Shi, Y. and Lin, H., (2018). Preventive effects of vitamin D on seasonal influenza A in infants: a multicenter, randomized, open, controlled clinical trial. The Pediatric infectious disease journal, 37(8), pp.749-754.
Zhou, Y.F., Luo, B.A. and Qin, L.L., (2019). The association between vitamin D deficiency and community-acquired pneumonia: A meta-analysis of observational studies. Medicine, 98(38).

