1Department of MSN (Nephrourology) Ramakrishna Mission Nursing School, Itanagar – 791113, India.
2Department of MSN (Neuroscience), Bengaluru-562123, India.
Corresponding author email:Shil.rahul06@gmail.com
Article Publishing History
Received: 26/08/2023
Accepted After Revision: 29/09/2023
Hepatitis is considered a public health challenge on the Asian continent and also in India. But due to the paucity of the data, the exact burden of the condition has not been established. Better disease-related knowledge will help to improve attitudes toward managing the complications and side effects and also prevent the further spread of infection. This study aimed to evaluate the knowledge and attitude regarding management, prevention, complications, and side effects of drugs among hepatitis B patients in Bengaluru, India. A hospital-based pre-experimental study was undertaken with 60 hepatitis-B patients who were admitted to KCG Hospital in Bengaluru. Knowledge and attitude regarding hepatitis-B were assessed using a validated questionnaire containing demographic data, a 30-item knowledge questionnaire, and 16-item Likert scale responses, respectively. SPSS V20.0 was used for data analysis and interpretation.
The descriptive statistics were presented with the mean, standard deviation, frequency, and percentage. The data were analyzed using a paired t-test. Further, to check the association, chi-square analysis was used. In the pre-test, 41 (68.3%) of the participants had inadequate knowledge, 19 (31.7%) had moderate knowledge, and none of the study participants had adequate knowledge. Furthermore, 60 (100%) participants had a neutral attitude, and none of the participants had an unfavorable and favorable attitude towards a hepatitis B patient. The findings of the study indicate that hepatitis B patients have a lack of knowledge and attitude regarding the prevention of complications, management, and side effects of drugs, which may lead to the further spread of infection in the community and hospital itself. Extensive health education, community reach, and health workers participation in campaigns related to hepatitis can have a rational control over the management of the disease.
Multimedia Education Program, Knowledge, Attitude, Prevention Of
Complication, Side Effects Of Drugs, Hepatitis-B Patients.
Biswas R. C, Shil R. Multimedia education program on knowledge and attitude regarding management, prevention of complication and side-effects of drugs on hepatitis-B among hepatitis patients – A pre-experimental study. Biosc.Biotech.Res.Comm. 2023;16(3).
Biswas R.C, Shil R. Multimedia education program on knowledge and attitude regarding management, prevention of complication and side-effects of drugs on hepatitis-B among hepatitis patients – A pre-experimental study. Biosc.Biotech.Res.Comm. 2023;16(3). Available from: <a href=”http://surl.li/lpukn“>http://surl.li/lpukn</a>
INTRODUCTION
Hepatitis B is a viral infection of the liver that is transmitted from an infected person to another through direct blood-to-blood contact, semen, or vaginal fluid. Although the route of transmission is similar to that of the HIV virus (Human Immunodeficiency Virus), the virus is 100 times more virulent and may live outside the body for up to a week. During this time, a virus can infect a person who is not protected from the virus. 1 HBV is present in blood, semen, and vaginal fluids and is transmitted primarily through sexual activity. Another major transmission route is the sharing of injection drug equipment (including needles, cookers, and tourniquets) and, to a lesser extent, non-injection drugs (cocaine straws and crack pipes) due to the possibility of exposure to blood. Pregnant mothers with hepatitis B may spread the virus to their offspring, most likely after childbirth (Ray 20217).
According to the World Hepatitis Alliance report, Africa has some of the highest prevalence rates in the world—over 8% for hepatitis B and 10% for hepatitis C in some areas. In America, it has been found that hepatitis B prevalence ranges from 2–8%. Areas with a high prevalence are those populated by indigenous communities. Hepatitis C prevalence among injecting drug users is 90%; 16–33% are co-infected with hepatitis C and HIV/AIDS. In Europe, it has been seen that 14 million people are chronically infected with hepatitis B and 9 million are chronically infected with hepatitis C, compared with 1.5 million HIV infections. In southeast Asia, about 65% of those with hepatitis B and 75% of those with hepatitis C don’t know they are infected (Puri 2014).
HBV is part of the Hepadnavirdae family in the genus Orthohepana virus. It is the leading cause of hepatitis, cirrhosis, and hepatocellular carcinoma (HCC) worldwide, resulting in 500,000 to 1.2 million deaths per year. The prevalence of HBV infection varies widely, so the risk of HBV infection to travellers will alter depending on destination 2. HBV infection has been associated with travel. Nine percent of all HBV cases reported in the Netherlands between 1992 and 2003 were travel-related, with an estimated incidence of HBV infection of 4.5 per 100,000 travellers. Fifty-one cases of HBV infection were identified from a cohort of ill travellers presenting to geosentinel clinics between 1997 and 2007, with HBV acquisition independently associated with older age and male sex (41–51 cases), possibly reflecting risk-taking behaviour including unsafe sex while abroad. However, given the long intubation period, we were unable to exclude the acquisition of acute HBV infection cases prior to travel. Studies of travellers have demonstrated that new sexual partners and unprotected intercourse are relatively common, particularly in the setting of excessive alcohol intake.
A study reported that India has over 40 million HBV carriers and accounts for 10–15% of the entire pool of HBV carriers in the world. Of the 25 million infants born every year in India, it is estimated that over 1 million run the lifeline risk of developing chronic HBV infection. Every year, over 100,000 Indians die due to illnesses related to HBV infection. There are varying reports of an overall rate of HB positivity ranging between 2-4.7%. Two agents are currently available for prophylaxis against hepatitis B viral infection. The first is hepatitis B immune globulin (HBIG), which provides temporary protection from HBV, (Ahmed et al., 2023).
The second is the hepatitis B vaccine, which has had a significant impact on health care workers to date. Recently, the FDA approved a synthetic nucleoside analog, lamivudine (Epivir-HBV™), for use in patients with chronic hepatitis B viral infection associated with evidence of viral replication and active liver inflammation. But Despite the introduction of hepatitis B virus (HBV) vaccination programs, chronic hepatitis B (CHB) remains an important disease burden worldwide. Currently, HBV treatment has improved in India. However, the effort is limited due to a lack of a hepatitis registry, good community-based epidemiology, and serological epidemiological studies (Ray 2017).
Therefore, this study was planned to assess the knowledge and attitude regarding management, prevention of complications, and side effects of drugs on hepatitis B among the hepatitis B patients. The findings of this study will help the medical and nursing fraternity come up with new ideas to tackle hepatitis B-related drug complications and side effects and also improve patients knowledge regarding hepatitis B (Jarju et al., 2022).
MATERIAL AND METHODS
Study design and population: An hospital-based pre-experimental study with a one-group pre-test and post-test design was undertaken on hepatitis B patients at KCG Hospital, Malleswaram, Bengaluru, in the years 2022–2023. A total of 60 hepatitis-B patients have participated in the study.
Study setting:Bangalore (also known as Bengaluru) is the capital of Karnataka state, India. This study was conducted at KCG Hospital, which is a public hospital situated at Malleswaram Circle, Bengaluru.
Sample size and sampling procedures: 60 patients who were diagnosed with hepatitis B and who were also admitted to the hospital were selected using the non-probability convenience sampling technique based on the inclusion criteria. The data was collected in person from patients at KCG Hospital who were willing to give informed consent and were included in the study. Patients who had developed a hepatitis complication, had an altered level of consciousness, and were not available at the time of data collection were excluded from the study (Ul Haq et al.,2013).
Data collection instrument: The data collection instrument was developed by the investigator. The validity and reliability of the tools were checked with the help of nursing experts and a biostatistician. The data collection instrument was divided into three sections. Section A included demographic characteristics such as age in years, gender, religion, education, occupation, monthly income, and family history of hepatitis. Section B included the structured knowledge assessment questionnaire. The questions were formulated based on general information regarding hepatitis (9 items), management of hepatitis B (7 items), prevention of complications regarding hepatitis B (8 items), and the side effects of drugs regarding hepatitis B (5 items). Furthermore, Section C included Likert’s attitude scale and the responses (strongly agree, agree, uncertain, disagree, strongly disagree).
Further, for the scoring interpretation, ‘1’ was awarded to the correct response and ‘0’ for the wrong response in all items for Section B, and a total score of 30 was allotted to interpret the level of knowledge. For the Likert’s attitude scale, the positive question score of 5’ was awarded for strongly agree, ‘4’ for agree, ‘3’ for being uncertain, ‘2’ for disagree and ‘1’ for strongly disagree. Furthermore, for the negative question, strongly agree was awarded to ‘1’, ‘2’ for agree, ‘3’ for uncertain, ‘4’ for disagree, and ‘5’ for strongly disagree. Thus, a total score of 80 was allotted. In order to establish the reliability of the tool, the split-half method was used. The calculated ‘r’ value was 0.92 for knowledge and 0.82 for Likert’s attitude scale, and the tool was found to be reliable (Mohamed et al., 2012).
Data collection technique: Formal permission was obtained from the concerned authority and the ethical committee of KCG Hospital. The data were collected from February 2 to March 31, 2023, and were collected by the researcher itself. The patients were requested to respond to the questionnaires through pen and paper with a consent form attached. The instructions were given to the auto drivers on the front page and also orally, not to use any materials for reference purposes and not to discuss with other patients to find out the correct answer. Around 15 minutes were taken for each subject to complete the questionnaires (Das & Shil 2022).
Data quality control: Data quality was assured by proper pre-testing and designing of the questionnaires, which were done at a rural community health center far from the original test site on 10% of the total participants to ensure that the questions were clear and easily understood by the respondents, and further questionnaires were refined based on the results of the pilot study (Mohamed et al., 2012).
Data processing and analysis: After the data collection, the data were exported from an Excel sheet to the statistical package for social sciences (SPSS) version 20.0 for analysis and interpretation. The descriptive statistics were presented with the mean, standard deviation, frequency, and percentage. The data were analyzed using a paired t-test. Further, to check the association, chi-square analysis was used (Dahl et al., 2012).
RESULTS
Table.1 Description of socio-demographic variables of patients with hepatitis B
| Sl.no | Demographic variables | Categories | Frequency (f) | Percentage (%) |
| 1 | Age | 21-30 | 24 | 40.0 |
| 31-40 | 19 | 31.7 | ||
| 41-50 | 17 | 28.3 | ||
| 2 | Gender | Male | 43 | 71.7 |
| Female | 17 | 28.3 | ||
| 3 | Religion | Hindu | 28 | 46.7 |
| Muslim | 12 | 20.0 | ||
| Christian | 18 | 30.0 | ||
| Others | 2 | 3.3 | ||
| 4 | Educational status | No formal education | 2 | 3.3 |
| Primary | 13 | 21.7 | ||
| Secondary | 17 | 28.3 | ||
| Hr. Secondary | 24 | 40.0 | ||
| Graduate and above | 4 | 6.7 | ||
| 5 | Occupation | Unemployed | 2 | 3.3 |
| Agriculture | 7 | 11.7 | ||
| Govt. Employee | 13 | 21.7 | ||
| Pvt. Employee | 29 | 48.3 | ||
| Housewife | 5 | 8.3 |
Table 1.a
| 6 | Family income per month(Rs) | <5000 | 10 | 16.7 |
| 5001-10000 | 22 | 36.7 | ||
| 10001-15000 | 19 | 31.7 | ||
| >15000 | 9 | 15.0 | ||
| 7 | Family history hepatitis | Yes | – | – |
| No | 60 | 100.0 | ||
| 8 | Heard about hepatitis | Yes | 60 | 100.0 |
| No | – | – | ||
| 9 | Source of information | Magazine | 12 | 20.0 |
| Health care professional | 18 | 30.0 | ||
| Family members | 18 | 30.0 | ||
| Friends | 12 | 20.0 |
A total of 60 hepatitis B patients participated in this study. Out of the study participants, the majority, 43 (71.7%), were male, and 24 (40%) were in the age group of 21 to 30 years. 28 (46.7%) of the participants were Hindu, and the majority of 29 (48.3%) of them work as private employees. With regards to education, 24 (40%) of the participants had higher secondary education and had an income of 5000 to 10000 rupees per month 22 (36.7%). Furthermore, every participant 60 (100%) heard about hepatitis, and the sources of information were health care professionals and family members 18 (30%). However, none of the 60 (100%) of the study participants had any family history of hepatitis (Das & Shil 2022)
Table.2 Frequency and percentage distribution of patients with hepatitis
B according to pre and post-test level of knowledge
| Sl.no | Level of knowledge | Pre test | Post test | ||
| No. (60) | Percentage (%) | No. (60) | Percentage (%) | ||
| 1 | Inadequate knowledge (<50%) | 41 | 68.3 | – | – |
| 2 | Moderate knowledge (50-75%) | 19 | 31.7 | 60 | 100.0 |
| 3 | Adequate knowledge (>75%) | – | – | – | – |
| Total | 60 | 100 | 60 | 100 | |
Table 2 depicts the pre-test and post-test frequency and percentage distribution of knowledge about hepatitis B. The result shows that in the pre-test, 41 (68.3%) of the participants had inadequate knowledge, 19 (31.7%) had moderate knowledge, and none of the study participants had adequate knowledge. Whereas, in the post-test, the result shows that all 60 participants (100%) had moderate knowledge, and none of them had inadequate or adequate knowledge. It shows that after the multimedia education program, the subject knowledge has improved, and the program is found to be effective (Dahl et al., 2012).
Figure:1 Distribution of patients with hepatitis B according to
pre-test and post-test level of knowledge
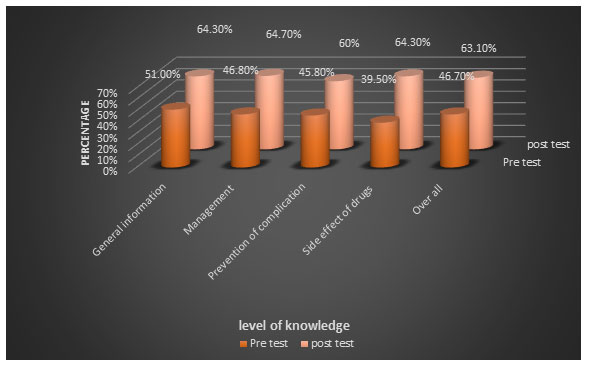
Table. 3 Frequency and percentage distribution of patients with hepatitis
B according to the pre and post-test level of attitude
| Sl.no | Level of attitude | Pre test | Post test | ||
| No. (60) | Percentage (%) | No. (60) | Percentage (%) | ||
| 1 | Unfavorable attitude (<50%) | – | – | – | – |
| 2 | Neutral attitude (50-75%) | 60 | 100.0 | – | – |
| 3 | Favourable attitude (>75%) | – | – | 60 | 100.0 |
| Total | 60 | 100 | 60 | 100 | |
Table 3 depicts the pre-test and post-test frequency and percentage distribution of attitudes towards hepatitis B. The result shows that in the pre-test, 60 (100%) of the participants had a neutral attitude, and none of the participants had unfavourable and favourable attitude towards hepatitis B patient. Whereas after the multimedia education program, all 60 participants (100%) had a favorable attitude towards hepatitis B. Therefore, it shows that the overall attitude has improved and the program has been found to be effective (Jarju et al., 2022).
Figure: 2 Percentage distribution of hepatitis B patients according
to pre-test and post-test level of attitude
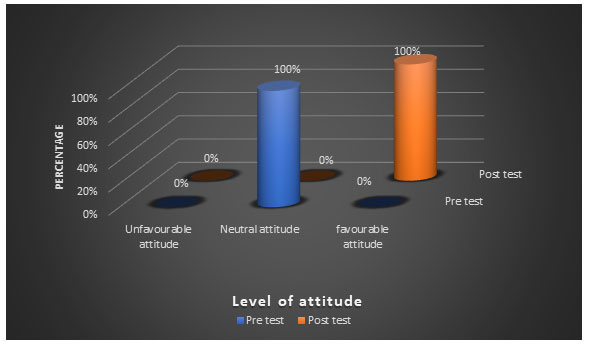
Table.4 Mean, SD and range of pre-test and post-test level of attitude
on hepatitis among patients with hepatitis B
| Sl.no | Attitude | Max. Score | Range | Mean | SD | Mean% |
| 1 | Pre test | 80 | 44-49 | 47.02 | 1.44 | 58.7 |
| 2 | Post test | 80 | 65-71 | 67.80 | 1.86 | 84.7 |
Table 4 depicts the mean, SD, and range of the pre- and post-test attitude levels. The table shows that in the pre-test, the range was 44–49, the mean was 47.02, the SD was 1.44, and the mean percentage was 58.7%. Whereas in the post-test, the range was 65–71, the mean was 67.80, the SD was 1.86, and the mean percentage was 84.7%. and it can be clearly seen that the mean percentage improved after the post-test (Mohamed et al., 2012)
Table. 5 Paired t-test analysis for the significance of pre and post-test level of
knowledge hepatitis among patients with hepatitis B
|
Sl.no |
Knowledge | Max. Score | Mean difference | SD of difference | % of mean difference | Paired t-value | p-value |
| 1 | General information regarding hepatitis B | 8 | 1.06 | 1.26 | 13.2 | 6.55 | p<,0.05 |
| 2 | Management of hepatitis B | 10 | 1.78 | 1.54 | 17.8 | 8.96 | p<,0.05 |
| 3 | Prevention of complication of hepatitis B | 8 | 1.13 | 1.39 | 14.1 | 6.29 | p<,0.05 |
| 4 | Side effects of drugs | 4 | 0.98 | 1.33 | 24.5 | 5.71 | p<,0.05 |
| Over all | 30 | 4.96 | 0.75 | 16.5 | 18.67 | p<,0.05 |
Note: *- denotes significant at 0.05 level at 59df (i.e. p<0.05)
Table 5 depicts the paired t-test analysis for the pre-test and post-test analysis. The table shows the mean difference, SD of difference, mean difference percentage, and statistical significance of knowledge regarding management, prevention of complications, and side effects of drugs on hepatitis among patients with hepatitis. The mean difference was 4.96, the SD was 0.75, the mean difference percentage was 16.5, and the t-value was found to be 18.67, which was highly significant at p<0.05 level (Das & Shil 2022).
Table. 6 Paired t-test analysis for the significance of pre and post-test level
of attitude on hepatitis patients with hepatitis B
| Attitude | Max. Score | Mean difference | SD of difference | % of mean difference | Paired t-value | p-value |
| Over all | 80 | 20.78 | 2.00 | 25.9 | 24.25 | P<0.05 |
Note: *- denotes significant at 0.05 level at 59df (i.e. p<0.05)
A paired “t” test was performed to determine the significance of the pre- and post-test levels of attitude regarding hepatitis. The table shows that the mean, standard deviation, and mean percentage of improvement in attitude regarding hepatitis B among hepatitis B patients where the maximum score was 80, the mean difference was 20.78, the SD of the difference was 2.00, the mean difference percentage was 25.9, and the t-value was found to be 24.25, which was highly significant at p<0.05 level (Mohamed et al., 2012).
Table.7 Correlation between knowledge and attitude on hepatitis among patients with hepatitis B
| Variables | Mean | SD | R | p-value |
| Knowledge | 14.02 | 0.79 | 0.741* | p<0.05 |
| Attitude | 18.98 | 0..83 |
Note: *- Significant at 5% level (i.e., p<0.05).
Table 7 depicts the correlation between knowledge and attitude toward hepatitis among patients with hepatitis. The result shows that there was a strong positive correlation between knowledge and attitude, and the calculated r value is 0.741*.
Figure: 3 Scatter graph of correlation between knowledge and attitude
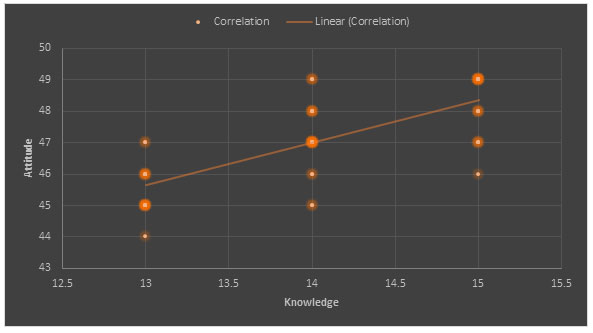
Table. 8 Association between mean difference of knowledge on hepatitis among patient
with hepatitis B with selected demographic variables
| Sl.no | Demographic
variables |
Categories | Sample (60) | Knowledge | χ2–
value |
p-value | |||||
| ≤ median | >median | ||||||||||
| No. | % | No. | % | No. | % | ||||||
| 1 | Age | 21-30 | 24 | 40.0 | 18 | 43.9 | 6 | 31.6 | 4.652,
df=2, NS |
p>0.05 | |
| 31-40 | 19 | 31.7 | 13 | 31.7 | 6 | 31.6 | |||||
| 41-50 | 17 | 28.3 | 10 | 24.4 | 7 | 36.8 | |||||
| 2 | Gender | Male | 43 | 71.7 | 29 | 70.7 | 14 | 73.7 | 0.056, df₌1, NS | p>0.05 | |
| Female | 17 | 28.3 | 12 | 29.3 | 5 | 26.3 | |||||
| 3 | Religion | Hindu | 28 | 46.7 | 19 | 46.3 | 9 | 47.4 | 3.56, df₌3, NS | p>0.05 | |
| Muslim | 12 | 20.0 | 10 | 24.4 | 2 | 10.5 | |||||
| Christian | 18 | 30.0 | 10 | 24.4 | 8 | 42.1 | |||||
| Others | 2 | 3.3 | 2 | 4.9 | 0 | 0 | |||||
| 4 | Educational status | No formal education | 2 | 3.3 | 2 | 4.9 | 0 | 0 | 28.69, df₌4, S | p<0.05 | |
| Primary | 13 | 21.7 | 13 | 31.7 | 0 | 0 | |||||
| Secondary | 17 | 28.3 | 16 | 39.0 | 1 | 5.3 | |||||
| Hr. Secondary | 24 | 40.0 | 10 | 24.4 | 14 | 73.7 | |||||
| Graduate and above | 4 | 6.7 | 0 | 0 | 4 | 21.1 | |||||
Table 8a
| 5 | Occupation | Unemployed | 2 | 3.3 | 2 | 4.9 | 0 | 0 | 19.09, df₌5, S | p<0.05 |
| Agriculture | 7 | 11.7 | 7 | 17.1 | 0 | 0 | ||||
| Govt. Employee | 13 | 21.7 | 3 | 7.3 | 10 | 52.6 | ||||
| Pvt. Employee | 29 | 48.3 | 21 | 51.2 | 8 | 42.1 | ||||
| Housewife | 5 | 8.3 | 5 | 12.2 | 0 | 0 | ||||
| Coolie / Daily wages | 4 | 6.7 | 3 | 7.3 | 1 | 5.3 | ||||
| 6 | Family income per month (Rs) | <5000 | 10 | 16.7 | 8 | 19.5 | 2 | 10.5 | 9.98, df₌3, S | p<0.05 |
| 5001-10000 | 22 | 36.7 | 19 | 46.3 | 3 | 15.3 | ||||
| 10001-15000 | 19 | 31.7 | 8 | 19.5 | 11 | 57.9 | ||||
| >15000 | 9 | 15.0 | 6 | 14.6 | 3 | 10.5 | ||||
| 7 | Family history hepatitis | Yes | – | – | – | – | – | – | Invalid | |
| No | 60 | 100 | 41 | 100 | 19 | 100 | ||||
| 8 | Heard about hepatitis | Yes | 60 | 100 | 41 | 100 | 19 | 100 | Invalid | |
| No | – | – | – | – | – | – | ||||
| 9 | Source information | Magazine | 12 | 20.0 | 8 | 19.5 | 4 | 21.1 | 7.868, df₌3, S | p<0.05 |
| Health care professional | 18 | 30.0 | 10 | 24.4 | 8 | 42.1 | ||||
| Family members | 18 | 30.0 | 11 | 26.8 | 7 | 36.8 | ||||
| Friends | 12 | 20.0 | 12 | 29.3 | 0 | 0 | ||||
Note: S-Significant at 5% level (i.e. p<0.05), NS-Not significant at 5% level (i.e. p>0.05).
Table 8 depicts the knowledge level and demographic variables. The result shows that the association between educational status (χ2 = 28.69), occupation (χ2 = 19.09), family income (χ2 = 9.98), and the source of information (χ2 = 7.868) was found to be statistically significant. Other demographic variables such as age, gender, religion, family history of hepatitis, and heard about hepatitis were found to be statistically non-significant.
Table. 9 Association between mean difference of attitude on hepatitis among patients
with hepatitis B with their selected demographic variables
| Sl.no | Demographic variables | Categories | Sample
(n=60) |
Attitude | χ2– value | p-value | ||||
| ≤median | >median | |||||||||
| No. | % | No. | % | No. | % |
1.58, df₌2, NS |
p>0.05 |
|||
| 1 | Age | 21-30 | 24 | 40.0 | 16 | 42.1 | 8 | 36.4 | ||
| 31-40 | 19 | 31.7 | 11 | 28.9 | 8 | 36.4 | ||||
| 41-50 | 17 | 28.3 | 11 | 29.0 | 6 | 27.3 | ||||
| 2 | Gender | Male | 43 | 71.7 | 26 | 68.4 | 17 | 77.3 | 0.53, df₌1, NS | p>0.05 |
|
Female |
17 | 28.3 | 12 | 31.6 | 5 | 22.7 | ||||
| 3 | Religion | Hindu | 28 | 46.7 | 16 | 42.1 | 12 | 54.5 | 2.36, df₌3, NS | p>0.05 |
| Muslim | 12 | 20.0 | 9 | 23.7 | 3 | 13.6 | ||||
| Christian | 18 | 30.0 | 11 | 28.9 | 7 | 31.8 | ||||
| Others | 2 | 3.3 | 2 | 5.3 | 0 | 0 | ||||
| 4 | Educational status | No formal education | 2 | 3.3 | 2 | 5.3 | 0 | 0 | 14.96, df₌4, S | P<0.05 |
| Primary | 13 | 21.7 | 12 | 31.6 | 1 | 4.5 | ||||
| Secondary | 24 | 28.3 | 12 | 31.6 | 12 | 54.5 | ||||
| Hr. Secondary | 17 | 40.0 | 16 | 39. | 1 | 15 | ||||
| Graduate and above | 4 | 6.7 | 0 | 0 | 4 | 18.2 | ||||
Table 9a
| 5 | Occupation | Unemployed | 2 | 3.3 | 2 | 5.3 | 0 | 0 | 19.064, df₌5,
S |
P<0.05 |
| Agriculture | 7 | 11.7 | 6 | 15.8 | 1 | 4.5 | ||||
| Govt. Employee | 13 | 21.7 | 2 | 5.3 | 11 | 50.0 | ||||
| Pvt. Employee | 29 | 48.3 | 20 | 52.6 | 9 | 40.9 | ||||
| Housewife | 5 | 8.3 | 5 | 13.2 | 0 | 0 | ||||
| Coolie/Daily wages | 4 | 6.7 | 3 | 7.9 | 1 | 4.5 | ||||
| 6 | Family income per month(Rs) | <5000 | 10 | 16.7 | 8 | 21.1 | 2 | 9.1 | 9.950, df₌3, S | P<0.05 |
| 5001-10000 | 22 | 36.7 | 18 | 47.4 | 4 | 18.2 | ||||
| 10001-15000 | 19 | 31.7 | 8 | 21.1 | 11 | 50.0 | ||||
| >15000 | 9 | 15.0 | 4 | 10.5 | 5 | 22.7 | ||||
| 9 | Source of information | Magazine | 12 | 20.0 | 7 | 18.4 | 5 | 22.7 | 2.703, df₌3, NS | P>0.05 |
| Health care professional | 18 | 30.0 | 11 | 28.9 | 7 | 31.8 | ||||
| Family members | 18 | 30.0 | 10 | 26.3 | 8 | 36.4 | ||||
| Friends | 12 | 20.0 | 10 | 26.3 | 2 | 9.1 |
Note: S-Significant at 5% level (i.e., p<0.05), NS-Not significant at 5% level (i.e., p>0.05).
Table 9 depicts the association between attitude level and demographic variables. The result shows that the association between educational status (χ2 = 14.96), family income (χ2 = 9.950), and occupation (χ2 = 19.064) was found to be statistically significant. Furthermore, the rest of the variables, such as age, gender, religion, and source of information, were found to be statistically non-significant.
DISCUSSION
India has an approximately 3.0% HBV career rate, with a high prevalence rate in the tribal population. Due to the lack of basic medical facilities in the remote areas, many of the tribal populations don’t get the required treatment, which can be fatal for the patients and also for the people nearby. Due to this, with a population of more than 1.35 billion, India has more than 37 million HBV carriers, which contributes a large proportion of this HBV burden. 9 The purpose of the present study was to assess the knowledge and attitude regarding management, prevention of complications, and side effects of drugs on hepatitis B among hepatitis B patients. Currently, there is little research data available related to this statement.
The findings of the present study suggest that in the pre-test, 41 (68.3%) of the participants had inadequate knowledge, 19 (31.7%) of them had moderate knowledge, and none of the study participants had adequate knowledge. Whereas, in the post-test, the result shows that all 60 participants (100%) had moderate knowledge, and none of them had inadequate or adequate knowledge. However, the findings were inconsistent when compared with a similar study done in Gambia 10 where the result shows that the majority of the participants have an adequate level of knowledge regarding hepatitis B. This discrepancy might be due to the study setting and large sample size. However, some study findings done in Pakistan 11,12 Malaysia13 and India 14 were consistent with our result.
One of the objectives of our research was to find out the attitude towards hepatitis B. The result shows that in the pre-test, 60 (100%) of the participants had a neutral attitude, and none of the participants had unfavourable and favourable attitude towards hepatitis B patient. However, after the education, all the participants 60 (100%) developed a favorable attitude. The similar negative attitude 309 (79.2%) was found in the study done in Pakistan 11,12 and Malaysia. 13 Although a higher attitude was found in a study done in Gambia 10 where two-third 107 (70%) of the participants had a positive attitude towards hepatitis B infection. This difference in the result could also be due to the fact that African nations have one of the highest numbers of hepatitis B patients. So the health information and higher education the people are receiving could also be more. Due to medical advancement, the ratio of hepatitis B is decreasing in India, which is also impacting the knowledge and attitude towards hepatitis B.
Our research has found multiple associations between knowledge level and demographics that were found to be statistically significant, such as educational status (χ2 = 28.69), occupation (χ2 = 19.09), family income (χ2 = 9.98), and the source of information (χ2 = 7.868). Some of the similar associations were also found in some studies. 11,12,13 Furthermore, a significant association was also found between attitude level and demographic variables such as educational status (χ2 = 14.96), family income (χ2 = 9.950), and occupation (χ2 = 19.064).
A positive correlation between knowledge and attitude was found in this study, which reaffirms the relationship between knowledge and attitude. It can be concluded that adequate knowledge can lead to a positive attitude that can manage and improve the management of complications and side effects of drugs in hepatitis B. The findings are not in line with the result of one of the previous studies, where the study showed no significant predictor of attitude among the sociodemographic and clinical characteristics variables. However, such differentiations in the results could be a representation of people’s education, the governmental approach to tackling hepatitis B, and mass health education to the general public.
To our knowledge, a small number of studies have been conducted regarding hepatitis B in western countries compared to Asian countries, as the majority of hepatitis B cases are found in Asian countries. A study was done in Melbourne, Australia 15 regarding the health literacy of chronic hepatitis B patients, which claimed to be the largest study done in Australia to investigate the knowledge of chronic hepatitis B patients who are attending a special outpatient clinic. The result suggested that most of the participants had a higher level of knowledge (7.5 out of 12 points) compared to previous studies.
Also, the study found a statistically significant association between knowledge score and demographic variables such as gender (P = 0.0268**), English literacy (P = 0.045**), educational level (P = 0.05**), having seen clinician previously (P = 0.010**), knowing anyone else with HBV (P = 0.007**), Friend comfortable (P = 0.049**). However, we have observed that the majority of the study has a significant association between knowledge and educational level, so in conclusion, we can say that patients with a higher educational level have higher knowledge regarding hepatitis B, its treatment, side effects, etc. The higher knowledge score in the study might be due to the higher literacy level and better sources of information in Australia. But different cultural factors and linguistically salient information from different countries can also play a role in the results of different research studies.
Education plays a vital role and has a definite effect on improving knowledge and also shaping negative views and attitudes about this disease. Early education regarding hepatitis B can help improve the knowledge of urban and rural populations. A better understanding of hepatitis B will improve the treatment outcome, reduce negative societal image, and reduce morbidity, stress, and anxiety regarding hepatitis B.
Limitation: The study was conducted at one hospital, which led to a small sample size. Also, the sampling technique used was non-randomized purposive sampling. and the study was limited to only hepatitis B patients. Hence, the findings of the study cannot be generalized to a large population.
CONCLUSION AND RECOMMENDATION
There are substantial burdens of HBV infection in Asia and the Pacific Islands, sub-Saharan Africa, the Amazon Basin, and Eastern Europe, despite the disease’s frequency being unevenly distributed throughout the world. But still, a number of issues in hepatitis B management remain controversial or unresolved, such as identifying treatment candidates, managing partial or nonresponses, and predicting treatment response. The authors hope that the study findings will support the stakeholders teachers, doctors, and nurses in making a significant decision to handle hepatitis B patients more efficiently.
Ethical Consideration: Institutional Ethics Committee approval was obtained before the research and actual data collection. Also, permission was obtained from the KCG hospital medical superintendent and ethical committee. A consent sheet was prepared in English with descriptions of the impact of the study on the respondents and attached to the tool on a separate page.
Authors Contribution: The authors made a significant contribution to the work reported. R.D. made study conception, execution, acquisition of data, analysis, and R.S. did design and interpretation of data. Finally, all the authors read, revised, and drafted the manuscript for publication and also gave final approval of the version to be published based on the selected journal to which the article has been submitted.
Funding: None declared
Conflicts of Interest: The authors reports no conflicts of interest in this research work.
Acknowledgements: We are thankful to the KCG hospital director for their permission to conduct the study also thankful to all of the patients who participated in the study.
REFERRENCES
Das M, Rahul Shil (2022). Awareness And Influencing Lifestyle Modification Factors Regarding Hepatitis B Among Non-Medical Students – Efficacy Of An Educational Package. International Journal Of Advances In Nursing Management. Vol 10(3):285-291.
Diseases-condition of hepatitis-B. 2023 Available fromhttp://wwww.healthsite.com/diseases-condition/hepatitis-B.
Hopkins medicine.http://www.hopkinsmedicine.org/gartroenterology heptology/pdfs/liver/viral hepatitis b pdf) 2023
Jarju L, Sheikh Omar Bittaye, Abdoulie Keita, Saydiba Tamba, Ramou Nije (2022). Knowledge And Attitude Of Hepatitis B Infection Among Patients With The Infection In The Main Liver Clinic In The Gambia. Pan African Medical Journal. Vol 42(252):1-11Mayoclinic.www.mayoclinic.org/diseases-conditions/hepatitis-b/basics/complication-2002210.
Mohamed R , Chirk Jenn Ng, Wen Ting Tong, Suraya Zainol Abidin, Li Ping Wong, Wah Yun Low (2012). Knowledge, Attitudes And Practices Among People With Chronic Hepatitis B Attending A Hepatology Clinic In Malaysia: A Cross Sectional Study. BMC Public Health. Vol 12(601):2-14.
Noman Ul Haq, Mohamed Azmi Hassali, Asrul Akmal Shafie, Fahad Saleem, Maryam Farooqui, Abdul Haseeb et al (2013). A Cross-Sectional Assessment Of Knowledge, Attitude And Practice Among Hepatitis-B Patients In Quetta, Pakistan. BMC Public Health.Vol 13(448):2-9
Puri P (2014). Tackling The Hepatitis B Disease Burden In India. Journal Of Clinical And Experimental Hepatology. Vol 4:312-319.
Ray G (2017). Current Scenario Of Hepatitis B And Its Treatment In India. Journal Of Clinical And Translational Hepatology. Vol 5(3):277-296.
Saba Ahmed, Rosario Yslado Mendez, Shaheyar Naveed, Shaaib Akhter, Iqra Mushtaque, Mareen A. Malik et al, (2023). Assessment Of Hepatitis-Related Knowledge, Attitudes And Practices On Quality Of Life With The Moderating Role Of Internalized Stigma Among Hepatitis B-Positive Patients In Pakistan. Health Psychology And Behavioural Medicine. Vol 11,1:1-18
Tanya FM Dahl, Benjamin C Cowie, Beverley-Ann Biggs, Karin Leder, Jennifer H Maclachlan, Caroline Marshall et al (2014). Health Literacy In Patients With Chronic Hepatitis B Attending A Tertiary Hospital In Melbourne: A Questionnaire-Based Survey. BMC Infectious Diseases. Vol 14(537):2-9
Wikipedia 2023 (the free encyclopedia0 hepatitis B.http://www.en.wikipedia.org/wiki?hepatitis_B
Wileyonlinelibray,journal of travelmedicine.Http://www.onlinelibray.wiley.com/doi/10.1111/jtm.12026/full.
World hepatitis alliance.prevailance and incidence of hepatitis-B. Available from http//ww.worldhepatititisaaliance.org/en/mediamatarial.html?files/worldhepatitisalliance/download/wdh/wdhcampaign%20material/world%/20hepatitis20days%20days/%20package.pdf.
World hepatitis alliance.prevalance and incidence of hepatitis-B. 2020 Available from http//ww.worldhepatititisaaliance.org/en/mediamatarial.html?files/worldhepatitisalliance/download/wdh/wdhcampaign%20material/world%/20hepatitis20days%20days/%20package.pdf.

