Associate Professor, and Consultant in Orthodontics, Department of Pediatric Dentistry and Orthodontics
College of Dentistry, King Saud University P.O. Box 60169-38 Riyadh 11545 Saudi Arabia.
Corresponding author email: nalmosa@ksu.edu.sa
Article Publishing History
Received: 25/07/2024
Accepted After Revision: 29/08/2024
The presence of supplementary teeth is a frequent developmental abnormality that can cause a variety of clinical issues. Impaction, delayed eruption, ectopic eruption, crowding, etc. are examples of clinical issues. Depending on their morphology, a single extra tooth might be conical, tuberculate, or supplementary. There are two types of multiple extra teeth: syndromic and non-syndromic. Their nature and position following appropriate clinical and radiographic tests determine how it should be managed. This case report describes a patient who has three maxillary central incisors, which are permanent and completely separated.
It was determined to be the midline unilateral left supplemental central incisor. In these situations, setting up an appropriate treatment strategy is crucial. A comprehensive clinical and radiographic examination, as well as a detailed history, especially the family history in the event of a systemic anomaly, are required. Its consequences and aesthetic issues can be reduced by following a thorough treatment plan. In these situations, a fixed orthodontic treatment plan that includes the extraction of the supplemental central incisor may be the best course of treatment.
Supernumerary Teeth; Central Incisor; Supplemental Teeth; Mesiodens; Crowding of Teeth;
Almosa N. Third Central Incisor as Supplemental Supernumerary Tooth: A Case Report. Biosc.Biotech.Res.Comm. 2024;17(3).
Almosa N. Third Central Incisor as Supplemental Supernumerary Tooth: A Case Report. Biosc.Biotech.Res.Comm. 2023;17(3). Available from: <a href=”https://shorturl.at/a5u91“>https://shorturl.at/a5u91</a>
INTRODUCTION
Any structure or teeth that are present in excess of the regular dentition are referred to as supernumerary teeth. Teeth may become misaligned as a result of them being impacted or ectopically erupted (Suljkanovic et al, 2021). There are numerous theories that attempt to explain their poorly understood origin. A few significant theories include the theories of hyperactivity, the dichotomy of the tooth bud (tooth germ producing two or more separate units), inheritance, excessive dental lamina growth, atavism (a reversion to a more primitive type of dentition), and that they are just remnants of the Anthropoids, who had more teeth than Homosapiens (Ata-Ali et al, 2014). Gardner syndrome, cleidocranial dysplasia, and cleft lip and palate are frequently linked to an increased frequency of extra teeth. The number, shape, and position of supernumerary teeth determine their classification (Subasioglu et al, 2015).
Depending on number, they may be single or multiple. According to their morphology, a single supernumerary tooth can be conical, tuberculate, odontome, closely resemble the natural tooth, or be supplemental. There are two types of multiple extra teeth: syndromic and non-syndromic (Shetty et al, 2019). The majority of syndromic multiple supernumerary teeth cases are observed in individuals with cleft lip and palate. The morphology of a supplemental tooth is identical to that of the normal neighbouring teeth, showing no anatomical differences. Although they can form anywhere along the dental arches, they are more common in the permanent dentition than in the deciduous dentition, and they are primarily seen in the maxillary anterior region (Tbeishat et al, 2024).
In the deciduous dentition, the prevalence of extra teeth ranges from 0.3% to 0.8%, whereas in the permanent dentition, it ranges from 1.5% to 3.5%. Males are more likely than females to have extra teeth (2:1), and Asian groups are more likely to have them. They may develop at any point in time prior to birth or up to ten years later (Ata-Ali et al, 2014).
Teeth that are supernumerary might remain in their positions for a long time without causing any clinical problems to the dentition. They could become eruptive, remain impacted, seem inverted, or take on an unusual ectopic posture (Gupta and Marwah 2012). The majority of the time, though, they result in local disruptions like midline diastema, crowding and malalignment of the incisors, displacement and rotation of the neighbouring teeth, potential dentigerous cyst development, root resorption or dilaceration, and migration into the maxillary sinus or nasal cavity.
In the maxillary anterior region, extra teeth can also be an aesthetic concern. In these situations, interceptive orthodontics is crucial in preventing the development of malocclusion (Sarne O et al, 2018). The severity of the malocclusion will undoubtedly be lessened if caught early enough to prevent negative consequences (Männchen et al 2022). This case study describes the unusual occurrence of an additional maxillary central incisor in the midline of a seventeen-year-old male with permanent dentition.
CASE REPORT
The Department of Pediatric Dentistry and Orthodontics at King Saud University in Riyadh, Saudi Arabia received a complaint from a seventeen-year-old male Saudi young adult. He was mostly upset about his “crooked teeth,” or lacklustre appearance. He had no prior health concerns, based on the patient history. Nonetheless, the dental history did reveal several previous endodontic and restorative operations. Examining the patient’s siblings produced no meaningful findings.
Figures 1 and 2 show the intraoral images and the patient profile, respectively. Tables 1 and 2 contain a list of the intraoral and extraoral examination details.
| Table 1. Details of the extra oral facial profile/parameters of the patient. | |||
| View | Parameters | Classification | Figure |
|
Frontal View |
Face Type | Mesocephalic |
1a |
| Symmetry | Fairly symmetrical | ||
| LAFH: | WNL | ||
| Lip Competency | Competent | ||
| Inter-labial Gap | None | ||
|
Frontal Smiling View |
Incisal Display | 90% |
1b |
| Gingival Display | IDP of posteriors | ||
| Buccal Corridors | Asymmetrical (Rt. wider) | ||
| U Midline to Face | M of #11 to Rt. 3mm | ||
| L Midline to Chin | Coincident | ||
|
Profile View |
Profile Type | Convex |
1c |
| Malar Prominence | Flat | ||
| Naso-Labial Angle | Slightly increased | ||
| Upper Lip Thickness | WNL | ||
| Upper Lip Length | 16mm | ||
| Lower Lip Length | 44mm | ||
| Lower Lip Thickness | WNL | ||
| Mento-Labial Sulcus | Average | ||
| Chin Morphology | Slightly retruded | ||
| Throat-Neck Angle | Slightly Obtuse | ||
| Table 2. Details of the intra oral features/parameters of the patient | |||
| View | Parameters | Classification | Figure |
|
Intraoral Frontal View |
Oral Hygiene | Poor |
2c |
| Soft Tissue | Thin & Inadequate attached gingiva related to L 3-3 | ||
| OB | Open bite #14-#25 of 1-4.5 mm | ||
| U/L dental midline | L to Lt. 3 mm to M of #11 | ||
| CR/CO shift | None | ||
| Cross-bite | Edge to edge #16, 4s & 5s | ||
|
Intraoral Right View |
Over Jet | 2 mm |
2b |
| Canine Classification | ½ unit Cl II | ||
| Molar Classification | Cl I | ||
|
Intraoral Left View |
Over Jet | 2 mm |
2e
|
| Canine Classification | ½ unit Cl III | ||
| Molar Classification | Cl I | ||
|
Upper Arch View |
Form | Ovoid |
2a |
| Arch Symmetry | Asymmetrical (A-P) | ||
| U 3s | displaced B | ||
| #12 | blocked P | ||
| Supernumerary tooth | b/w centrals | ||
|
Lower Arch View |
Form | Ovoid | 2d |
| Arch Symmetry | Asymmetrical (A-P) | ||
| Teeth | Multiple rotated | ||
| Space Analysis | Upper | -11 mm | – |
| Lower | -6 mm | ||
| Bolton Analysis | Mandibular | Excess | – |
| Anterior ratio (3-3) | 1.8 mm | ||
| Overall ratio (6-6) | 1 mm | ||
Figure 1: a: Frontal view of the patient.; b: Frontal smiling view of the patient.;
c: Lateral Profile view of the patient.
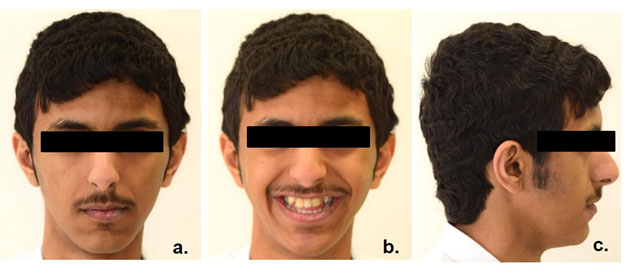
Figure 2: a: Occlusal view of the upper arch.; b: Right lateral view of the upper/lower teeth in occlusion.;
c: Frontal view of the upper/lower teeth in occlusion.; d: Occlusal view of the lower arch.;
e: Left lateral view of the upper/lower teeth in occlusion.
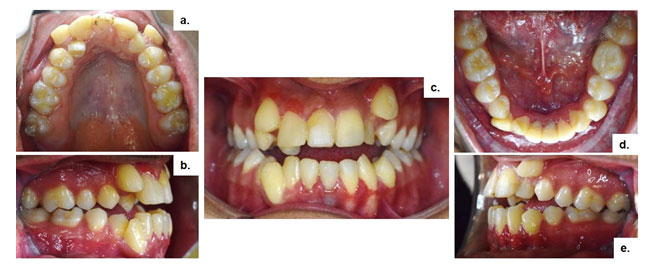
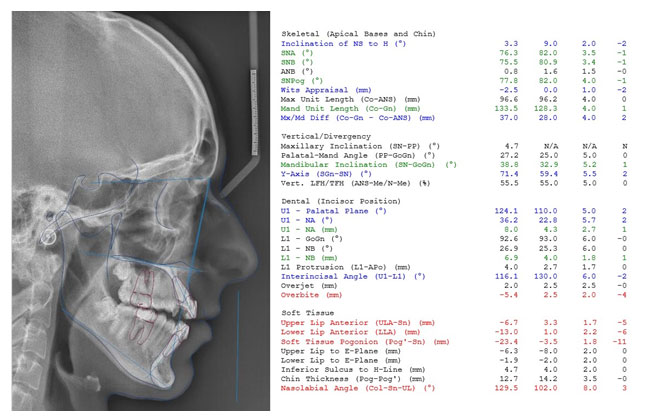
Because it resembled the nearby normal central incisors morphologically, the central incisor that faced the midline was referred to as a supernumerary or supplemental central incisor. A difference in arch length resulted in a minor rotation of the central incisors (Table 2 & Figure 3). Three maxillary central incisors were visible on an orthopantomogram (OPG) (Figure 4). Multiple restored teeth and lower central incisors with endodontic treatment were also seen on the OPG. Thermal and electric pulp tests yielded positive results for all three upper central incisors. Figure 5 displays the specific readings of the different parameters obtained from the lateral cephalogram. The diagnosis and treatment plan was explained in details to the patient and his parents.
Figure 3: Casts fabricated and used for space analysis of the
patients upper and lower arches.
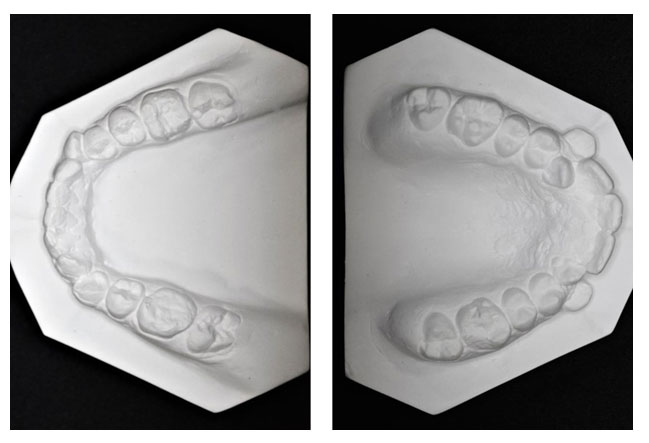
Figure 4: OPG of the patient showing permanent dentition 7-7 with the supernumerary, all 8s are present.
Dilacerated roots of #22, #34 & #44. WNL Asymmetrical condyles (left side smaller).

Figure 5: Lateral Cephalogram of the patient with all the measurements.
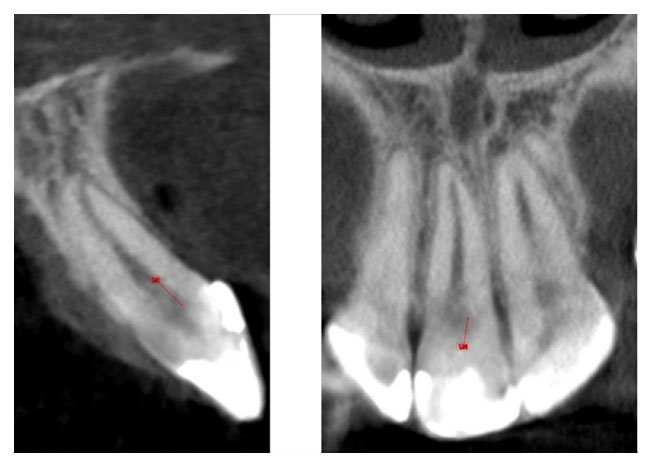
Further radiographic investigations were also carried out in the form of CBCT which revealed normal
apex closure for the three central incisors (Figure 6).
Figure 6: CBCT images of the supernumerary/supplemental
permanent central incisor tooth.
DISCUSSION
A third central incisor that is a supernumerary or supplemental tooth is the subject of this extremely uncommon case report. The majority of extra teeth typically occur in the maxillary midline and are referred to be mesiodens; general dentists are well-versed in treating these types of teeth (Akitomo et al, 2023). The extra or supernumerary tooth in this unusual case report, however, was a fully grown central incisor. Although they have been documented in the literature, bilateral supernumerary/supplemental central incisors are uncommon; even more uncommon are occurrences of solitary supernumerary/supplemental central incisors. In fact, there have only been five occurrences documented in the literature to date (Kumar et al, 2012).The majority of supplemental teeth are still unerupted, and this has been linked to a number of pathological problems, including an
kylosis, expanded follicular space, dentigerous cyst formation, dental pulp necrosis, pulp canal obliteration, and root resorption. Common issues include permanent tooth rotations, diastema development, and disturbances in eruption (Chalakkal et al, 2018). Because they are typically aberrant in size and shape, most erupted supernumerary teeth are excised for cosmetic reasons. On the other hand, Holtzman L, reports an example of a preserved erupted conical supernumerary tooth (Holtzman 1998).
In men, supernumerary/supplemental cases are marginally more prevalent (Mathew et al, 2023). The male case in ours is 17 years old young adult. In between the supplementary central incisor are two permanent central incisors. The lateral incisors erupted palatally, while the canines erupted buccally. All of the lower incisors had erupted, but the lower arch teeth were largely normal. Since the supernumerary/supplemental tooth in this case study is likewise positioned in the upper jaw, the incidence of hyperdontia in the upper jaw is eight times higher than in the lower jaw (Mathew et al, 2023).
Most supernumerary teeth are unable to erupt normally, and when they do, it’s usually ectopically, emerging alongside regular teeth. In our instance, however, an extra permanent central incisor tooth (supernumerary/supplemental) erupted in the upper arch precisely between the two regular permanent central incisor teeth, taking its position within the arch without becoming ectopic (Ata-Ali et al, 2014; Kumar et al, 2012). Regarding the extra permanent tooth, its future impact on the dental arch is uncertain as it has not yet broken through. Removal of a supernumerary premolar should be done to reduce crowding and/or prevent occlusal discrepancies if it is erupting or is crowded after eruption, according to Khalaf K et al, 2018.
To restore the natural appearance and functionality in this instance, it was determined to extract the erupted supernumerary/supplemental central incisor. The rehabilitation was to begin with the standard protocol of periodontal/restorative assessment and management before the extraction of the supernumerary/supplemental tooth, followed by fixed orthodontic treatment in order to establish a good occlusion, because the patient came to the clinic at an age when all of his permanent teeth had fully erupted and he had a full set of dentition (Suljkanovic et al, 2021).
Before a final diagnosis and treatment plan are developed, it is imperative to count and detect supernumerary/supplemental teeth both clinically and radiographically. A good treatment strategy requires accurate identification of every tooth both clinically and radiographically. Creating the perfect treatment strategy for every patient with extra or supernumerary teeth may be challenging (Kumar et al, 2012; Suljkanovic et al, 2021).
However, an attempt can undoubtedly be made. Depending on the type, quantity, and location of any extra teeth—whether impacted or erupted—as well as any accompanying pathology and how it affects the neighboring teeth, treatment of any extra teeth should be approached carefully, taking into account issues with oral cleanliness and aesthetics (Gupta and Marwah 2012). The course of treatment might range from simple elimination of unnecessary teeth to extraction and orthodontic correction to create a healthy occlusion. Although there isn’t a set course of treatment for this illness, most experts advise extraction. This is, in fact, the methodology that is taught in undergraduate and graduate textbooks (Baxi et al, 2023).
Common issues include permanent tooth rotations, diastema development, and disturbances in eruption. Finding and identifying issues related to additional or supernumerary teeth is the initial step in the management process. The teeth are routinely pulled, which usually requires surgery, if issues are present (Ahammed et al, 2021). Early extraction of supernumerary/supplemental teeth that produce incisor impaction may reduce loss of eruptive potential, space loss, and centerline displacement. Early extraction of the supplemental or supernumerary tooth that is causing the rotation of the unerupted incisors can lead to self-correction and proper alignment, even in cases when the rotation is severe (Acharya 2015).
The possibility that early removal will interfere with the development of neighboring roots is the biggest worry. It takes anywhere from six months to three years for the unerupted tooth to erupt following the extraction of supernumerary teeth. On the other hand, fully erupted supernumerary/supplemental maxillary central incisors may cause a significant crowding of the upper arch teeth, pushing the lateral incisors toward the palate and dislodging the canines to the buccal region, leading to malocclusion. Managing the gap left after the supernumerary or supplemental tooth is extracted presents one of the biggest hurdles in these circumstances (Meighani and Pakdaman 2010).
CONCLUSION
When a patient has extra or supernumerary maxillary central incisors, the practitioner should be made aware of the possible risks. Any patient who has extra or supernumerary maxillary central incisors should undergo a comprehensive evaluation. During a patient’s initial assessment, a comprehensive clinical examination should always be carried out in addition to any recommended radiographic imaging. CBCT may be used when additional information is required for a precise diagnosis and treatment plan. Early detection and therapy, essential components of preventive dentistry, can help prevent orthodontic issues and dental pathology related to supernumerary/supplemental maxillary central incisors. This could have a significant positive impact on the quality of life for young patients. Depending on the kind, quantity, and placement of the teeth as well as any potential issues, especially those involving aesthetics, a thorough treatment plan should include both surgical extraction and orthodontic correction followed by long-term retention.
Patient Consent Declaration:The authors certify that they have all required patient consent paperwork in their possession. The consent form for the patient(s) and/or their parents allows the publication of the patient(s)’ photos and other clinical data in the journal. The patients are aware that although every attempt will be made to hide their identity, anonymity cannot be guaranteed and that their names and initials will not be published.
Financial assistance and sponsorship: Nil.
Potential conflicts of interest: There are no competing interests to disclose.
REFERENCES
Acharya S. Supernumerary Teeth in Maxillary Anterior Region: Report of Three Cases and Their Management. Int J Sci Stud 2015;3(3). Int J Sci Stud 2015;3(3):122-127
Ahammed H, Seema T, Deepak C, Ashish J. Surgical Management of Impacted Supernumerary Tooth: A Case Series. Int J Clin Pediatr Dent. 2021 Sep-Oct;14(5):726-729. doi: 10.5005/jp-journals-10005-2008. PMID: 34934291; PMCID: PMC8645632.
Akitomo T, Asao Y, Iwamoto Y, Kusaka S, Usuda M, Kametani M, Ando T, Sakamoto S, Mitsuhata C, Kajiya M, Kozai K, Nomura R. A Third Supernumerary Tooth Occurring in the Same Region: A Case Report. Dent J (Basel). 2023 Feb 12;11(2):49. doi: 10.3390/dj11020049. PMID: 36826194; PMCID: PMC9955779.
Arandi NZ, Abu-Ali A, Mustafa S. Supernumerary teeth: a retrospective cross-sectional study from Palestine. Pesqui Bras Odontopediatria Clín Integr. 2020; 20:e5057. https://doi.org/10.1590/pboci.2020.029
Ata-Ali F, Ata-Ali J, Peñarrocha-Oltra D, Peñarrocha-Diago M. Prevalence, etiology, diagnosis, treatment and complications of supernumerary teeth. J Clin Exp Dent. 2014 Oct 1;6(4):e414-8. doi: 10.4317/jced.51499. PMID: 25593666; PMCID: PMC4282911.
Baxi S, Bhatia V, Tripathi AA, Kumar P, Pandey A, Dilip Taide P. Asymmetric Extraction Decision in Orthodontics. Cureus. 2023 Jun 8;15(6):e40162. doi: 10.7759/cureus.40162. PMID: 37431361; PMCID: PMC10329744.
Chalakkal P, Krishnan R, De Souza N, Da Costa GC. A rare occurrence of supplementary maxillary lateral incisors and a detailed review on supernumerary teeth. J Oral Maxillofac Pathol. 2018 Jan-Apr;22(1):149. doi: 10.4103/jomfp.JOMFP_213_15. PMID: 29731581; PMCID: PMC5917532.
Gupta S, Marwah N. Impacted supernumerary teeth-early or delayed intervention: decision making dilemma? Int J Clin Pediatr Dent. 2012 Sep;5(3):226-30. doi: 10.5005/jp-journals-10005-1173. Epub 2012 Dec 5. PMID: 25206175; PMCID: PMC4155876.
Holtzman L. Conservative treatment of supernumerary maxillary incisor with dens invaginatus. Journal of Endodontics1998; 24 (5): 378 – 380
Khalaf K, Al Shehadat S, Murray CA. A Review of Supernumerary Teeth in the Premolar Region. Int J Dent. 2018 Dec 3;2018:6289047. doi: 10.1155/2018/6289047. PMID: 30631362; PMCID: PMC6304893.
Kumar A, Namdev R, Bakshi L, Dutta S. Supernumerary teeth: Report of four unusual cases. Contemp Clin Dent. 2012 Apr;3(Suppl 1):S71-7. doi: 10.4103/0976-237X.95110. PMID: 22629072; PMCID: PMC3354792.
Männchen R, Serafin M, Fastuca R, Caprioglio A. Does Early Treatment Improve Clinical Outcome of Class II Patients? A Retrospective Study. Children (Basel). 2022 Feb 9;9(2):232. doi: 10.3390/children9020232. PMID: 35204952; PMCID: PMC8870289.
Mathew JA, Kamble R, Das S, Nerurkar S. A Case of Supernumerary Incisors in a Young Male Child: A Rare Occurrence of Four Central Incisors in the Maxillary Anterior Region. Cureus. 2023 Feb 16;15(2):e35047. doi: 10.7759/cureus.35047. PMID: 36942181; PMCID: PMC10024247.
Meighani G, Pakdaman A. Diagnosis and management of supernumerary (mesiodens): a review of the literature. J Dent (Tehran). 2010 Winter;7(1):41-9. Epub 2010 Mar 31. PMID: 21998774; PMCID: PMC3184724.
Sarne O, Shapira Y, Blumer S, Finkelstein T, Schonberger S, Bechor N, Shpack N. Supernumerary Teeth in the Maxillary Anterior Region: The Dilemma of Early Versus Late Surgical Intervention. J Clin Pediatr Dent. 2018;42(1):55-61. doi: 10.17796/1053-4628-42.1.10. Epub 2017 Sep 22. PMID: 28937895.
Shetty S, Agarwal N, Shetty P, Iqbal AM. Twin supernumerary teeth: A tale of two cases. Can J Dent Hyg. 2019 Feb 1;53(1):67-71. PMID: 33240343; PMCID: PMC7533809.
Subasioglu A, Savas S, Kucukyilmaz E, Kesim S, Yagci A, Dundar M. Genetic background of supernumerary teeth. Eur J Dent. 2015 Jan-Mar;9(1):153-158. doi: 10.4103/1305-7456.149670. PMID: 25713500; PMCID: PMC4319293.
Suljkanovic N, Balic D, Begic N. Supernumerary and Supplementary Teeth in a Non-syndromic Patients. Med Arch. 2021 Feb;75(1):78-81. doi: 10.5455/medarh.2021.75.78-81. PMID: 34012205; PMCID: PMC8116093.
Tbeishat M, Odeibat AM, Ersheidat A, Mahasneh A. Non-syndromic Bilateral Supernumerary Teeth in the Primary and Secondary Dentition: A Rare Case Report. Cureus. 2024 Mar 2;16(3):e55385. doi: 10.7759/cureus.55385. PMID: 38562341; PMCID: PMC10982841.

