Department of Restorative Dental Sciences, Division of Endodontics, College
of Dentistry, King Saud University, Riyadh, Saudi Arabia.
Corresponding author email: Almadikhalid40@gmail.com
Article Publishing History
Received: 28/06/2021
Accepted After Revision: 17/09/2021
Among all the causes of root canal failure, incapability to identify and negotiate additional canals is one which is of prime value, from treatment point of view. Mandibular molars display anatomical variations in the form of an additional root located lingually (radix entomolaris) or buccally (radix paramolaris). It is critical to understand the root morphology and canal patterns of teeth indicated for canal treatments for successful treatment outcomes. This case report presents a re-root treatment of a failed root canal treatment of a first molar tooth with Radix Entomolaris.
Correct interpretation of angled radiographs and careful examination of the access cavity chamber floor and use of recent concepts in access cavity preparation along with the sound knowledge of the variable anatomy helps clinician to locate and treat the root canals in case of Radix Entomolaris. The findings of the present case report suggests that correct interpretation of angled radiographs and careful examination of the access cavity chamber floor is pivotal in managing Radix Entomolaris. The use of recent concepts in access cavity preparation along with the accurate understanding of variable anatomy helps clinician to locate and treat the root canals in case of Radix Entomolaris
Failure, Molar teeth, Radix Entomolaris, Root canal treatment, Treatment success.
Almadi K. H. The Radix Entomolaris: Management of a Failed Root Treatment : A Case Report. Biosc.Biotech.Res.Comm. 2021;14(3).
Almadi K. H. The Radix Entomolaris: Management of a Failed Root Treatment : A Case Report. Biosc.Biotech.Res.Comm. 2021;14(3). Available from: <a href=”https://bit.ly/3tzpU19“>https://bit.ly/3tzpU19</a>
Copyright © This is an Open Access Article distributed under the Terms of the Creative Commons Attribution License (CC-BY). https://creativecommons.org/licenses/by/4.0/, which permits unrestricted use distribution and reproduction in any medium, provided the original author and sources are credited.
INTRODUCTION
The healing of periapical pathology is influenced by comprehensive cleaning via chemo-mechanical means and shaping of the infected radicular canals (Parashar et al. 2015). Among all the causes of root canal failure, incapability to identify and negotiate additional canals is one of them. Thus, the understanding of the dentist towards the unusual root canal anatomy is an important aspect during an endodontic treatment. The mandibular first molar tooth because of its age, position and pattern of eruption is the most commonly involved tooth with endodontic requirement (Campos 1989; Calberson et al. 2007). It displays the most significant morphological variation related to number of canals and the roots among the entire dentition (Sarangi and Uppin 2014; Lima et al. 2020).
Carabelli in (1844), accidently found mandibular molar a supernumerary third root which is found to be located on disto-lingually side of the tooth and named it as “radix entomolaris” (RE) (Pai et al. 2014). RE can be found in any of the mandibular molars with least occurring in second molars (Sinha et al. 2016). Literature revealed that RE most commonly displayed vertucci type 1 canal configuration (Meidyawati et al. 2016). It occurs most frequently in Mongoloid race with a frequency of 5-30%. Whereas, in white Caucasian, African, Eurasian and Indian populations frequency was less than 5% (Kuzekanani et al. 2017; Duman et al. 2020).
Radiographic analysis is a prerequisite to identify and instrument the extra canals, which if overlooked will later be responsible for future failure of root canal treatment (RCT). Previous studies rely on an additional angulated periapical radiograph by tube shifting mesially and distally at 20–30 degrees angle (Parallax technique). This technique helps to identify extra root and canal manifestation and its position using Buccal Object Rule. Nowadays, cone beam volumetric tomography (CBVT) has gained more importance due to its highly informative nature when compared to tube shifted periapical radiographs.
Case Report Presentation: A 26-year-old female patient visited the dental OPD with a complain of spontaneous pain on biting in lower right area from 1 month. Medical history revealed that patient is not allergic to any drug. BP and pulse was in the normal range i.e. 124/85, 70 respectively. On the basis of medical history patient was classified as ASA I which corresponds to normal healthy patient. Patient also revealed that she had undergone RCT, 5 years ago from a general dental practitioner. An extra-oral examination showed a symmetric face with no head and neck lymph node involvement. TMJ examination revealed no clicking sound with limited mouth opening. Upon intraoral clinical examination it was found that that tooth was previously restored with PFM crown and it is sensitive to percussion and palpation.
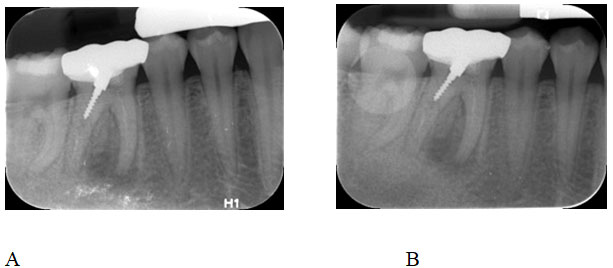
Gingiva around the tooth appeared infected and swollen. In order to get a clearer picture a periapical radiograph was performed. From the routine radiographic examination it was found the roots were poorly obturated with metal post on the distal canal and displaying PDL widening (Fig 1 A). On detailed examination of the periapical radiograph it was found that there was a third root present between the mesial and distal roots, which was confirmed by additional, angulated periapical radiograph (Fig 1B). A periapical radiolucency was observed at the disto-lingual canal and mesial canal of the tooth (Fig.1A).
Figure 1: Pre-operative radiographs of the tooth
Re-endodontic treatment was planned and patient was informed regarding the treatment for informed consent. Before starting the dental treatment, local anesthetic was injected and access cavity was prepared (Fig 2A). Removal of the metal screw post was achieved using ultrasonic tip (Fig 2B & C).
Figure 2: Clinical Removal of post form the tooth prior to root canal treatment.

All the canal orifices were negotiated with the help of DG-16 explorer. Four canals were found under operating microscope magnification (M320 dental microscope, Leica Microsystems, Germany). The apex locator (Root ZX II, J Morita, Germany) was used to determine the working length. After the conventional hand filing, universal protaper was used to prepare all the four canals. The canals were constantly irrigated using 6% sodium hypochlorite (NaOCL) After instrumentation was completed, calcium hydroxide was placed for 7 days and patient was recalled.
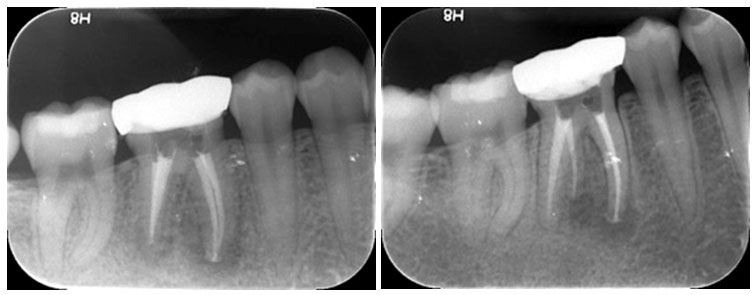
On the patient visit after 7 days intra canal medicament was removed by irrigating the canal with NaOCL and hand instrument followed by final rinse with 17% Ethylenediaminetetraacetic acid (EDTA). The canals were dried using paper points and obturated using warm vertical compaction with Gutta-percha and AH Plus sealer (Maillefer Dentsply, Ballaigues, Switzerland) (Fig 3 & 4).
Figure 3: Working Radiograph taken for assessing the working length for root filling
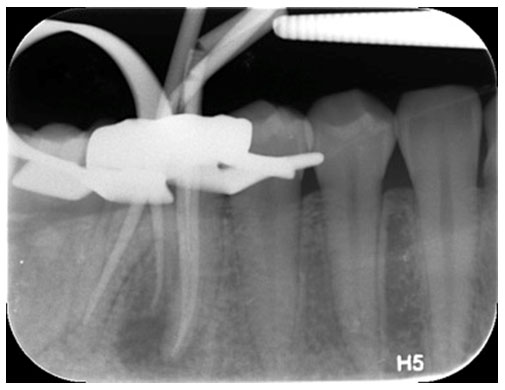
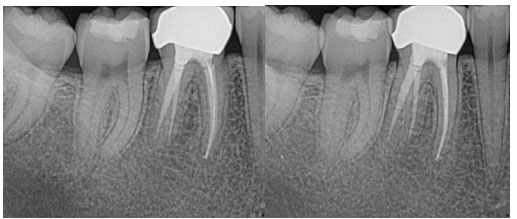
Figure 4: Final Radiographs of the root treated tooth after completion of re-root treatment
The patient was reviewed regularly at 12 months interval and a radiograph was taken after two-year follow up (Fig 5).
Figure 5: Radiogrpahs of the re root treated tooth at 2 years follow up with no radiological signs of pathology.
Comparative Analysis: A thorough and deep understanding of canal morphology is an important aspect which determines the clinical success of the RCT. With the introduction of latest techniques and expertise related to access cavity preparation, location of canals in atypical chamber morphology becomes less challenging (Tu et al. 2019). Missed canals due to inadequate knowledge of anatomy usually leads to root canal failure. Available literature revealed that approximately 97.8% of lower first molars exhibit two roots (Vertucci 1984; Christie and Thompson 1994; Pattanshetti et al. 2008).
Out of which, 64.4% displayed three canals with two within the mesial root and one in the distal root. However, 28% of cases showed two canals in the distal root (Iwanaga et al. 2020; Alkahtany et al. 2021). RE which is comparatively a rare finding during root dental procedure. The actual causes of its occurrence are still not discovered. However, some researchers assumed that this may be due to some disruption of pathway during odontogenesis or it may be due to genetic predisposition (Carlsen and Alexandersen 1990; Iwanaga et al. 2021).
Accessory roots and canals can be identified using conventional periapical radiographs at different angulations (Kang et al. 2014). There are multiple ways including law of symmetry, dentinal map visualization, bleeding point from the orifice, ultrasonic tips, 1% methylene blue dye for chamber staining, champagne bubble test, and CBCT to identify the accessory or missed canals (Rouas et al. 2007; Oliveira et al. 2018; Lima et al. 2020).
If RE is identified before initiation of endodontic procedure it is preferred to prepare a modified trapezoidal access cavity for canal location (López-Rosales et al. 2015) . De Moor et al. in their study revealed that in most of the RE cases the canals were curved (De moor et al. 2004). Therefore, exploration of canals with K patency file (size 10 or less) followed by working length and curvature determination using periapical radiograph to avoid procedural accident is preferred (Chaganti, 2017; Duman et al. 2020).
Most of the time it was observed that, radix ento-molaris canal orifice are covered and occluded with secondary dentinal tissue. The preparation of access cavity in such cases may result in perforation (Attam et al. 2012; Różyło et al. 2014). Hence, it should be kept in mind that secondary dentin is mostly white and opaque in color whereas pulp chamber is comparatively darker and gray in appearance (Gupta et al. 2013). The visual access and greater control of instruments during access preparation will help to prevent any mishap (Mahendar et al. 2013; Duman et al. 2020).
CONCLUSION
The findings of the present case report suggests that correct interpretation of angled radiographs and careful examination of the access cavity chamber floor is pivotal in managing Radix Entomolaris. The use of recent concepts in access cavity preparation along with the accurate understanding of variable anatomy helps clinician to locate and treat the root canals in case of Radix Entomolaris.
Case Report (Human Studies) Ethical Clearance Statement: The Current Case Report/ Studies were Conducted as Per the Guidelines of SCARE.
Riaz A Agha et al., (2020). The SCARE 2020 Guideline: Updating Consensus Surgical Case Report (SCARE) Guidelines. doi: 10.1016/j.ijsu.2020.10.034. Epub 2020 Nov 9.
Conflict of Interests: Author declares no conflict of interest to disclose.
REFERENCES
Calberson, F.L., De Moor, R.J. and Deroose, C.A., (2007). The radix entomolaris and paramolaris: clinical approach in endodontics. Journal of endodontics, 33(1), pp.58-63.
Carlsen, O.L.E. and Alexandersen, V., (1990). Radix entomolaris: identification and morphology. European Journal of Oral Sciences, 98(5), pp.363-373.
Chaganti, A., (2017). Radix Entamolaris And Paramolaris: A Review. Accessed on 5 June 2021. https://pesquisa.bvsalud.org/portal/resource/pt/sea-184678.
Christie, W.H. and Thompson, G.K., (1994). The importance of endodontic access in locating maxillary and mandibular molar canals. Journal (Canadian Dental Association), 60(6), pp.527-32.
De Moor, R.J.G., Deroose, C.A.J.G. and Calberson, F.L.G., (2004). The radix entomolaris in mandibular first molars: an endodontic challenge. International endodontic journal, 37(11), pp.789-799.
Oliveira, R.D.S., Oliveira, A.M.G., Junqueira, J.L.C. et al. (2018). Association between the anatomy of the mandibular canal and facial types: a cone-beam computed tomography analysis. International journal of dentistry, 20 (3), pp 124-131
Duman, S.B., Duman, S., Bayrakdar, I.S. et al. (2020). Evaluation of radix entomolaris in mandibular first and second molars using cone-beam computed tomography and review of the literature. Oral radiology, 36(4), pp.320-326.
Campos, H.F., (1989). Three canals in the mesial root of mandibular first permanent molars: a clinical study. International endodontic journal, 22(1), pp.39-43.
Gupta, N., Goswami, M. and Singh, K. (2013). Bilateral radix entomolaris with primary and permanent mandibular first molars. Case Reports, 2013, p.bcr2013200018.
Iwanaga, J., Katafuchi, M., Matsushita, Y., et al. (2020). Anatomy of the mandibular canal and surrounding structures: Part I: Morphology of the superior wall of the mandibular canal. Annals of Anatomy-Anatomischer Anzeiger, 232, p.151580.
Iwanaga, J., Kunisada, Y., Masui, M., et al. (2021). Comprehensive review of lower third molar management: A guide for improved informed consent. Clinical Anatomy, 34(2), pp.224-243.
Kuzekanani, M., Walsh, L.J., Haghani, J. et al. (2017). Radix entomolaris in the mandibular molar teeth of an Iranian population. International journal of dentistry, 23 (4) pp. 139-145.
Kang, J.H., Lee, K.S., Oh, M.G., et al. (2014). The incidence and configuration of the bifid mandibular canal in Koreans by using cone-beam computed tomography. Imaging science in dentistry, 44(1), pp.53-60.
Lima, C.O., Barbosa, A.F.A., Ferreira, C.M., et al. (2020). The impact of minimally invasive root canal preparation strategies on the ability to shape root canals of mandibular molars. International Endodontic Journal, 53(12), pp.1680-1688
López-Rosales, E., Castelo-Baz, P., De Moor, R., et al. (2015). Unusual root morphology in second mandibular molar with a radix entomolaris, and comparison between cone-beam computed tomography and digital periapical radiography: a case report. Journal of medical case reports, 9(1), pp.1-6.
Mahendra, M., Verma, A., Tyagi, S., et al. (2013). Management of complex root canal curvature of bilateral radix entomolaris: three-dimensional analysis with cone beam computed tomography. Case reports in dentistry. 20 (2). Pp. 31-37
Meidyawati, R. and Suprastiwi, E., (2016). Root Canal Treatment of Mandibular First Molar with Radix Entomolaris. Open Journal of Stomatology, 6(9), pp.193-200.
Pai, A.V., Jain, R. and Colaco, A.S., (2014). Detection and endodontic management of radix entomolaris: Report of case series. Saudi Endodontic Journal, 4(2), p.77-79
Parashar, A., Gupta, S., Zingade, A. et al. (2015). The radix entomolaris and paramolaris: A review and case reports with clinical implications. J Interdiscipl Med Dent Sci, 3(1), pp.161-6.
Pattanshetti, N., Gaidhane, M. and Al Kandari, A.M., (2008). Root and canal morphology of the mesiobuccal and distal roots of permanent first molars in a Kuwait population–a clinical study. International Endodontic Journal, 41(9), pp.755-762.
Rouas, P., Nancy, J. and Bar, D., (2007). Identification of double mandibular canals: literature review and three case reports with CT scans and cone beam CT. Dentomaxillofacial Radiology, 36(1), pp.34-38.
Sarangi, P. and Uppin, V.M., (2014). Mandibular first molar with a radix entomolaris: An endodontic dilemma. Journal of Dentistry (Tehran, Iran), 11(1), p.118.
Sinha, D.J., Mahesh, S., Jaiswal, N. et al. (2016). Radix entomolaris: A report of two cases. The Bulletin of Tokyo Dental College, 57(4), pp.253-258.
Tu, M.G., Huang, H.L., Hsue, S.S., et al. (2009). Detection of permanent three-rooted mandibular first molars by cone-beam computed tomography imaging in Taiwanese individuals. Journal of endodontics, 35(4), pp.503-507.
Vertucci, F.J., (1984). Root canal anatomy of the human permanent teeth. Oral surgery, oral medicine, oral pathology, 58(5), pp.589-599.

