Faculty of Economics and Social Sciences, An-Najah National University, Nablus, Palestine
Corresponding author email: shadi.k@najah.edu
Article Publishing History
Received: 12/07/2020
Accepted After Revision: 15/09/2020
The current study aims to investigate the long-term effects of war and occupation among Palestinian children in West Bank.The situation in the West Bank is uncommon in the frequency with which children are exposed to war-related traumatic events on a daily basis and because of the long-term nature of the conflict. The study sample was basic school students in West Bank; that consisted of 537 students; 242 (45%) were males and 295 (55%) were females and the mean of age in the sample was (14.8 ± 1.12). There were 341 (64%) of the students from villages and there were 196 (36%) students from cities. The participants completed a Checklist of Traumatic Experiences (CTE).The study found that almost every Palestinian child of the sample had been exposed traumatic experiences (chronic trauma). There is more than 22% of the participants exposes from 11 – 15 traumatic experiences from the total 34 traumatic experiences; such as any of your friends, neighbours, or relatives been injured by the occupying forces, inhaling tear gas, any of your friends, neighbours, or relatives been killed by occupying forces, witnessed anyone being arrested by the occupying forces, and the occupied forces used your house, block, camp, or zone as a cordon. Also, the study found that males are more exposed to traumatic experiences than females; moreover, there were significant differences between residences; students from villages are more exposed to traumatic experiences than cities.The study provides valuable evidence that demographic and socioeconomic factors mediate the relationship between different war traumatic events. Interventions should take into account the children’s background including their gender, age, where they live, and their socioeconomic status (e.g., family income, parents’ educational level, family size) to alleviate the psychological symptoms and to enhance their resilience.
Traumatic Experiences, Youth, Palestine, Collective Trauma, CTE
Abualkibash S. K. The Exposure to Traumatic Experiences Among the Palestinian Students in the West Bank. Biosc.Biotech.Res.Comm. 2020;13(3).
Abualkibash S. K. The Exposure to Traumatic Experiences Among the Palestinian Students in the West Bank. Biosc.Biotech.Res.Comm. 2020;13(3). Available from: https://bit.ly/2ZHepqK
Copyright © Abualkibash This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-BY) https://creativecommons.org/licenses/by/4.0/, which permits unrestricted use distribution and reproduction in any medium, provide the original author and source are credited.
INTRODUCTION
For more than half a century, Palestinians have suffered from various levels of traumatic experiences. Since the beginning of the second Intifada, which began in September 2000, the Palestinian people have been exposed to violence. The Palestinian nation suffers from traumatic events imposed by armed and/or military violence together with restriction of movement through checkpoints, closures and curfews. Traumatic events such as shootings, bombings, destruction of houses, fields, physical violence and deaths occur on a daily basis, El-Khodary Samara 2019a & 2019b).The Palestinian children who are part of the society living under occupation suffer from insomnia, fear of the dark, phobias, depression, bedwetting, social withdrawal, negative social-interaction, aggressive behaviour, forgetfulness and truancy from school. These indicators reveal that it is almost impossible to have a normal childhood in Palestine under the current circumstances and it is affecting their future psychological well-being (Altawil, 2008, El-Khodary Samara 2019a & 2019b).
Gaboulaud et al. (2010) presented data of 1773 children and adults who received treatment by psychotherapists between November 2000 and January 2006, in the Gaza Strip and in the West Bank. Nearly half of the patients were children between 4 and 14 years. The three main diagnoses were a) anxiety disorder, b) mood disorder, and c) PTSD.In addition, most of the studies regarding psychological health and recovery in Palestine were conducted in the Gaza Strip. The results have revealed that Palestinian children who live in war zones are at high risk of suffering from PTSD, somatic disorders and psychosocial problems (Kanninen, Punamäki, & Qouta, 2003; Qouta & El-Sarraj, 2004; Thabet & Vostanis, 2000). Palestinian students who grew up in the Intifada depicted students in their drawings as being beaten or shot by soldiers (Garbarino, Kostelny, & Dubrow, 1991; Holt, 2001). Furthermore, the number of traumatic experiences was related to higher levels of neuroticism and the lack of attention, concentration and memory (Qouta, Punamäki, & Sarraj, 1995).
A study by Abu Hein, Qouta, and El Sarraj (1993) found a high rate, about (25%), of the Palestinian students that were living in Gaza strip they were exposed to traumatic experiences during the first intifada. Another study revealed that Palestinian children who living in the West Bank they were mainly suffer from behavior and psychosomatic problems (Baker, 1990). Therefore, it seems that Palestinian children are surviving from traumatic events. They need to stand up, adapt, bounce back, recover and endeavor to overcome all difficulties in spite of the circumstances that surround them. Given that the majority of the people are exposed to traumatic events, the question is not only the type of oppression from which they suffer, but how to foster the capacity to overcome such difficult circumstances. Researchers and psychologists have emphasized disappointment and unhappiness as well as anxiety and depression rather than the strengths and potentialities of the people of Palestine, but still the main question remains how to facilitate overcoming traumas or how to grow up with a good mental health in spite of the traumatic events. (El-Khodary Samara 2019a & 2019b).
The Diagnostic and Statistical Manual of Mental Disorders, 4th edition, Text Revision (American Psychiatric, 2000), defines trauma including the events, and the person response to it. Trauma as direct personal experience of an event that involves actual or threatened death or serious injury, or other threat to one’s physical integrity; or witnessing an event that involves death, injury, or a threat to the physical integrity of another person; or learning about unexpected or violent death, serious harm, or threat of death or injury experienced by a family member or other close associate (Criterion A1). And criterion A2, as the person’s response to the event must involve intense fear, helplessness, or horror (or in children, the response must involve disorganized or agitated behavior) (Criterion A2). (American Psychiatric, 2000).
Several studies have revealed that exposure to previous traumatic war experiences and events is a risk factor for the development of post-traumatic stress disorder (PTSD), grief, and depression. The exposure to traumatic events, specifically physical injuries, loss of loved ones, immediate risk of life, injury of a family member or friend and losing a family member are the strongest risk factors for PTSD (El-Khodary Samara 2019a & 2019b).
Individuals or groups exposed to traumatic experiences generally demonstrate some form of stress that is why it is often referred to as traumatic stress. Responses of Traumatic stress has been widely researched by a psychologists; (Awadh, Vance, El-Beblawi, & Pumariega, 1998; Barber, 2009; Benjamin & Crawford-Browne, 2010; Bonanno, 2004; Breslau, Davis, & Andreski, 1995; Daniel, Jane, & Ann, 2005; Elbedour, Onwuegbuzie, Ghannam, Whitcome, & Hein, 2007; Espié et al., 2009, Palosaari, Punamäki, Diab, & Qouta, 2013; Stevens, Eagle, Kaminer, & Higson-Smith, 2013; Thabet, Abu Tawahina, El Sarraj, & Vostanis, 2008; Thabet & Vostanis, 1999; Yule, 2000 Dimitry, 2012; Dubow et al., 2012; Eagle & Kaminer, 2013; Khamis, 2015).
Posttraumatic Stress Disorder (PTSD) is included in the DSM-5 on a new chapter called Trauma and Stress or Related Disorders, (American Psychiatric, 2013).The diagnostic criteria for the manual’s next edition identify the trigger to PTSD as exposure to actual or threatened death, serious injury or sexual violation. The exposure must result from one or more of the following scenarios, in which the individual experiencing the traumatic event in a direct way, witnessing the traumatic event personally,and an indirect experience of the traumatic event that occurred to a close family member or close friend (with the actual or threatened death being either violent or accidental); or immediate repeated experiences or extreme exposure to cruel forms of the traumatic event (not through media, unless work-related). (American Psychiatric, 2013).
However, traumatic stress does not necessarily lead to PTSD or other mental disorders; in fact, the majority of cases resolve themselves over time and does not create any lasting psychopathology (J. Breslau, 2004). This is especially important given that evidence demonstrates that cross-cultural differences exist in the manner by which emotional and behavioral disorders and problems are expressed (Rahman, Mubbashar, Harrington, & Gater, 2000). Moreover, in situations of war and conflict, violence and trauma are often experienced collectively, with repercussions for a sense of community security, and not merely individually (Giacaman, Shannon, Saab, Arya, & Boyce, 2007).
In this regard, some scholars have also attempted to resolve this disjuncture by harmonizing different perspectives of individual and collective trauma (e.g. Abramowitz, 2005; Kienzler, 2008)). In response to this, new dimensional approaches to trauma are being developed, which integrate the biological, cultural and clinical dimensions of trauma in the explanatory framework of trauma (e.g. Kirmayer et al., 2007). There is a need to assess if Palestinian children live under traumatic situations. Individuals who are directly or indirectly exposed to war and conflict experience a variety of adverse short and long-term psychological reactions. Common symptoms and reactions in the aftermath of potentially traumatic experiences include anger, sleeping difficulties, nightmares, and avoidance of situations that are reminders of the trauma, impairment of concentration, and guilt due to survival or lack of personal injury during the traumatic event. A number of studies have found a high prevalence of symptoms, including Post Traumatic Stress Disorders (PTSD) among children exposed to war trauma, state-sponsored terrorism or interpersonal violence (Palestinian Center for Human Rights, 2009).
Research have been mainly done in Gaza, and few data are coming from the West Bank; assessing traumatic experiences is not only to assess PTSD, but also checking how everyone perceive their situation according to their especial context, and specially under a collective traumatic situation. These information will allow to take measures to increase not only individual psychotherapeutic attention, but community psycho-social attentions in war torn zones (Shalhoub‐Kevorkian, 2008). The war and the long term occupation of Palestinian territory expose students to recurrent traumatic experiences which violate their human rights: the right to live, to learn, to be healthy, to live with his/her family and community, to develop his/her personality, to be nurtured and protected, and the right to enjoy childhood. The potential for having a normal childhood in Palestine is unlikely in the current circumstances and the future psychological well-being of Palestinian children is at risk of being compromised by on-going traumatic experiences.
MATERIAL AND METHODS
Participants and Procedure:The sample consisted of 537 Palestinian public-school students of 13 and 14 years old living in the West Bank (OPT Occupied Palestinian Territories). They were 55% girls and 45% boys. About two thirds (64%) were from rural areas and (36%) from urban areas. For the study, 25 schools were randomly selected as representative of schools in the North directorate of the West Bank. At each school 10 students from 8th grade and 10 students from 9th grade, were randomly selected. The High Ministry of Education provided the permission to access the public schools, and then researcher informed the pupils, their parents, and headmaster about the purpose of study, obtaining their consent for participation.
Measures:Traumatic war experiences: The Checklist of Traumatic Experiences (CTE) (Altawil, 2008), is a 34-item scale that covers events that are typical in the Palestinian Israel-occupied territories, such as being arrested, threated, injured, exposure to shelling or house demolition. Adolescents reported whether they had been exposed to the events (Yes = 1; No = 0), and the number of times that they have experienced such event. In this study, each item has been analysed individually, taking the frequency that students reported that they have experienced each situation. Frequencies reported higher than 10 times were recoded as 10.
RESULTS AND DISCUSSION
Research findings presented in this study, contain two parts; the first part presents descriptive statistics of Exposure to traumatic experiences: frequency and percentage of the traumatic experiences. The second part presents descriptive statistics of constructs exposure to traumatic experiences, according to the effects of Demographic Factors as gender, place and area.
First part: How Palestinian adolescents are exposed to traumatic experiences, data shows that all of the forms suffered by the sample, being the most often the explosions and sound bombs, tear gas, and funerals; while the lowest is being shouted or house being bulldozed (see table 1, 2 & 4)
Table 1. Exposure to traumatic experiences: frequency and percentage of traumatic experiences
| # | The items of traumatic experiences | yes | % |
| 24 | Have you been exposed to the hearing of the explosion sounds or the sound bombs? | 429 | .7989 |
| 3 | Have you been exposed to inhaling tear gas? | 384 | .7151 |
| 29 | Have you witnessed a martyr’s funeral? | 344 | .6406 |
| 32 | Have you witnessed anyone being arrested by the occupying forces? | 311 | .5791 |
| 11 | Have the occupied forces used your house, block, camp, or zone as a cordon? | 287 | .5364 |
| 30 | Have you witnessed the occupying forces beating anyone? | 278 | .5177 |
| 15 | Has any of your friends, neighbours, or relatives been killed by occupying forces? | 277 | .5158 |
| 31 | Have you witnessed injuring by the occupying forces? | 258 | .4804 |
| 27 | Have you witnessed the occupying forces opening fire against people? | 250 | .4655 |
| 17 | Has any of your friends, neighbours, or relatives been injured by the occupying forces? | 241 | .4488 |
| 20 | Have you attended to martyr’s funeral? | 214 | .3985 |
| 19 | Has anyone been killed in front of your eyes by occupying forces? | 206 | .3836 |
| 33 | Have you witnessed the occupying forces destroying trees or farms? | 169 | .3147 |
| 34 | Have you witnessed the occupying forces not allowing an ambulance to reach a hospital? | 167 | .3110 |
| 16 | Has any of your close family members been injured by occupying forces? | 160 | .2980 |
| 23 | Have the occupied forces destroyed a land or farm of yours or of a dear person by a bulldozer. | 142 | .2644 |
| 14 | Has any of your close family members (father, mother, brother, sister) been killed by occupying forces? | 126 | .2346 |
| 22 | Has anyone of your close family members been exposed to humiliation by occupying forces? | 122 | .2272 |
| 25 | Have you witnessed the occupying forces destroying house(s). | 108 | .2011 |
| 28 | Have you witnessed people being shelled and bombed? | 105 | .1955 |
| 8 | Have you been exposed to live fire by occupying forces, but you were not injured? | 100 | .1862 |
| 7 | Have you been injured to the degree that you lost consciousness? | 82 | .1527 |
| 12 | Have the occupied forces threatened you with the possibility of not allowing access to your home? | 78 | .1453 |
| 21 | Have you been exposed to humiliation by occupying forces? | 71 | .1322 |
| 26 | Have you witnessed shelling by tanks, artillery, or military planes? | 63 | .1173 |
| 18 | Has anyone of your close family members been killed in front of your eyes by occupying forces? | 57 | .1061 |
| 9 | Have you been exposed to shelling by tanks, artillery, or military planes, but you were not injured? | 56 | .1043 |
| 10 | Have you been beaten by occupied forces? | 34 | .0636 |
| 6 | Have you been shot with a rubber bullet by occupying forces? | 33 | .0615 |
| 4 | Have you been injured by shelling (e.g. wounds, burns, or bone break) by tanks, artillery, or military planes? | 32 | .0596 |
| 2 | Has your house been partially destroyed by shelling or bulldozing? | 22 | .0410 |
| 13 | Have you been arrested by occupying forces? | 18 | .0336 |
| 1 | Has your house been completely destroyed by shelling or bulldozing? | 16 | .0298 |
| 5 | Have you been shot with live ammunition by occupying forces? | 9 | .0168 |
Table 2. Number of traumatic experiences and percentages according to the types (N: 537)
| Types | N. of Traumas | Frequency | Percent % | Valid Percent | Cumulative Percent |
| F | 0-5 | 134 | 25.0 | 25.0 | 25.0 |
| E | 6-10 | 183 | 34.1 | 34.1 | 59.0 |
| D | 11-15 | 120 | 22.3 | 22.3 | 81.4 |
| C | 16-20 | 82 | 15.3 | 15.3 | 96.6 |
| B | 21-25 | 14 | 2.6 | 2.6 | 99.3 |
| A | 26-34 | 4 | .7 | .7 | 100.0 |
| Total | 537 | 100 | 100.0 | ||
According to the dimensions of traumatic experiences, the researcher found that the most dimension exposed among the respondents was the Distant exposure with; (M: 0.42, SD: 0.30) and the least dimension was Material Exposure with; (M: 0.11, SD: 0.18), (see table 4, and Figure 1).
Table 3. The means of exposure to traumatic events according to the dimension, in descending order
| Dimension | N | Range | Minimum | Maximum | Mean | Std. Deviation | |
| V | Distant Exposure | 537 | 1.00 | .00 | 1.00 | .4195 | .30115 |
| III | Indirect Exposure | 537 | 1.00 | .00 | 1.00 | .3175 | .26579 |
| IV | Proximate Exposure | 537 | 1.00 | .00 | 1.00 | .3051 | .24216 |
| I | Direct Exposure | 537 | 1.00 | .00 | 1.00 | .2431 | .15587 |
| II | Material Exposure | 537 | 1.00 | .00 | 1.00 | .1117 | .17964 |
Figure 1: The means of exposure to traumatic events according to the dimension
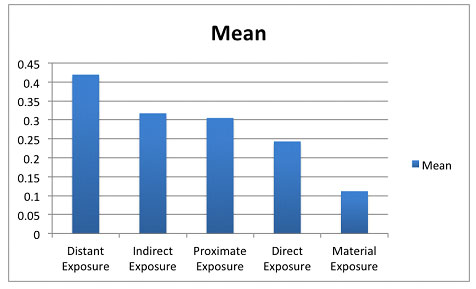
Table 4. Frequency and percentages of traumatic experiences (N: 537)
| The statements of traumatic experiences | Item no | Type | Frequency | (%) |
| Has any of your friends, neighbors, or relatives been injured by the occupying forces? | 17 | IV | 242 | .4488 |
| Have you witnessed the occupying forces opening fire against people? | 27 | V | 250 | .4655 |
| Have you witnessed injuring by the occupying forces? | 31 | V | 258 | .4804 |
| Has any of your friends, neighbors, or relatives been killed by occupying forces? | 15 | IV | 277 | .5158 |
| Have you witnessed the occupying forces beating anyone? | 30 | V | 278 | .5177 |
| Have the occupied forces used your house, block, camp, or zone as a cordon? | 11 | I | 287 | .5364 |
| Have you witnessed anyone being arrested by the occupying forces? | 32 | V | 311 | .5791 |
| Have you witnessed a martyr’s funeral? | 29 | III | 344 | .6406 |
| Have you been exposed to inhaling tear gas? | 3 | I | 384 | .7151 |
| Have you been exposed to the hearing of the explosion sounds or the sound bombs? | 24 | I | 429 | .7989 |
Second part: this part of the Effects of Demographic Factors will answer the question if there are significant differences in the level of exposure to traumatic experiences according to (gender, place, age and Area). In order to test the differences between the respondents in study variables, according to gender, place, and Age the researcher used independent sample t-test. Table 6 shows the results.
Table 5. The Results of Independent Sample T-Test for the Differences in Study Variables According to Gender, Place, and Age
| Constructs | Mean | S.D. | Mean | S.D. | T-value | P-value |
| Gender | Males n = 242 | Females n = 295 | ||||
| CTE | 0.321 | 0.17 | 0.260 | 0.157 | 3.99** | 0.000 |
| Place | Cities n = 196 | Villages n = 341 | ||||
| CTE | 0.263 | 0.162 | 0.301 | 0.166 | -2.95** | 0.009 |
| Age | Age 13 n = 268 | Age 14 n = 269 | ||||
| CTE | 0.31 | 0.19 | 0.34 | 0.21 | -1.55 | 0.120 |
As illustrated in table 6, there are significant differences between males and females in CTE in benefit to males (p < 0.05), also there are significant differences between Cities and Villages in CTE in benefit to Villages (p < 0.05). And no significant differences according to the Age.In order to test the differences between the respondents according to Gender, the researcher used one-way ANOVA test, tables 7 and 8 show the results.
Table 6. The Results of Descriptive statistics For the Study Variables According to Gender
| N | Mean | Std. Deviation | Std. Error | 95% Confidence Interval for Mean | Minimum | Maximum | |||
| Lower Bound | Upper Bound | ||||||||
| Direct Exposure | Male | 242 | .2863 | .16905 | .01087 | .2649 | .3077 | .00 | .93 |
| Female | 295 | .2075 | .13287 | .00774 | .1923 | .2227 | .00 | .71 | |
| Total | 537 | .2430 | .15516 | .00670 | .2299 | .2562 | .00 | .93 | |
| Material Exposure | Male | 242 | .1253 | .19536 | .01256 | .1006 | .1501 | .00 | 1.00 |
| Female | 295 | .1006 | .16513 | .00961 | .0816 | .1195 | .00 | .67 | |
| Total | 537 | .1117 | .17964 | .00775 | .0965 | .1270 | .00 | 1.00 | |
| Indirect Exposure | Male | 242 | .3502 | .26072 | .01676 | .3172 | .3832 | .00 | 1.00 |
| Female | 295 | .2907 | .26734 | .01556 | .2600 | .3213 | .00 | 1.00 | |
| Total | 537 | .3175 | .26579 | .01147 | .2950 | .3400 | .00 | 1.00 | |
| Proximate Exposure | Male | 242 | .3202 | .23607 | .01518 | .2904 | .3501 | .00 | .83 |
| Female | 295 | .2927 | .24675 | .01437 | .2644 | .3209 | .00 | 1.00 | |
| Total | 537 | .3051 | .24216 | .01045 | .2846 | .3256 | .00 | 1.00 | |
| Distant Exposure | Male | 242 | .4604 | .30016 | .01930 | .4224 | .4985 | .00 | 1.00 |
| Female | 295 | .3860 | .29828 | .01737 | .3518 | .4201 | .00 | 1.00 | |
| Total | 537 | .4195 | .30115 | .01300 | .3940 | .4451 | .00 | 1.00 | |
| CTE Total | Male | 242 | .3215 | .16967 | .01091 | .3000 | .3429 | .00 | .82 |
| Female | 295 | .2596 | .15705 | .00914 | .2416 | .2776 | .00 | .76 | |
| Total | 537 | .2875 | .16559 | .00715 | .2735 | .3015 | .00 | .82 | |
Table 7. The Results of One Way ANOVA for the Differences in Study Variables According to Gender
| Sum of Squares | df | Mean Square | F | Sig. | ||
| Direct Exposure | Between Groups | .825 | 1 | .825 | 36.564* | .000 |
| Within Groups | 12.078 | 535 | .023 | |||
| Total | 12.904 | 536 | ||||
| Material Exposure | Between Groups | .082 | 1 | .082 | 2.537 | .112 |
| Within Groups | 17.214 | 535 | .032 | |||
| Total | 17.296 | 536 | ||||
| Indirect Exposure | Between Groups | .471 | 1 | .471 | 6.740* | .010 |
| Within Groups | 37.394 | 535 | .070 | |||
| Total | 37.865 | 536 | ||||
| Proximate Exposure | Between Groups | .101 | 1 | .101 | 1.728 | .189 |
| Within Groups | 31.332 | 535 | .059 | |||
| Total | 31.433 | 536 | ||||
| Distant Exposure | Between Groups | .738 | 1 | .738 | 8.244* | .004 |
| Within Groups | 47.871 | 535 | .089 | |||
| Total | 48.609 | 536 | ||||
| CTE Total | Between Groups | .508 | 1 | .508 | 19.171* | .000 |
| Within Groups | 14.189 | 535 | .027 | |||
| Total | 14.697 | 536 | ||||
There are significant differences between males and females in the dimension; Direct Exposure, Indirect Exposure, Distant Exposure and CTE total in benefit to males (p < 0.01). Thus the males are more likely to expose to traumatic experiences than female.
In order to test the differences between the respondents according to Place the researcher used one-way ANOVA test, tables 9 and 10 show the results.
Table 8. The Results of Descriptive statistics For the Study Variables According to Place
| N | Mean | Std. Deviation | Std. Error | 95% Confidence Interval for Mean | Minimum | Maximum | |||
| Lower Bound | Upper Bound | ||||||||
| Direct Exposure | Village | 341 | .2570 | .15735 | .00852 | .2403 | .2738 | .00 | .79 |
| City | 196 | .2187 | .14854 | .01061 | .1977 | .2396 | .00 | .93 | |
| Total | 537 | .2430 | .15516 | .00670 | .2299 | .2562 | .00 | .93 | |
| Material Exposure | Village | 341 | .1163 | .18210 | .00986 | .0969 | .1357 | .00 | 1.00 |
| City | 196 | .1037 | .17544 | .01253 | .0790 | .1285 | .00 | .67 | |
| Total | 537 | .1117 | .17964 | .00775 | .0965 | .1270 | .00 | 1.00 | |
| Indirect Exposure | Village | 341 | .3468 | .26530 | .01437 | .3185 | .3750 | .00 | 1.00 |
| City | 196 | .2666 | .25952 | .01854 | .2300 | .3031 | .00 | 1.00 | |
| Total | 537 | .3175 | .26579 | .01147 | .2950 | .3400 | .00 | 1.00 | |
| Proximate Exposure | Village | 341 | .3123 | .24647 | .01335 | .2861 | .3386 | .00 | 1.00 |
| City | 196 | .2925 | .23456 | .01675 | .2595 | .3256 | .00 | .83 | |
| Total | 537 | .3051 | .24216 | .01045 | .2846 | .3256 | .00 | 1.00 | |
| Distant Exposure | Village | 341 | .4349 | .29809 | .01614 | .4031 | .4666 | .00 | 1.00 |
| City | 196 | .3929 | .30533 | .02181 | .3498 | .4359 | .00 | 1.00 | |
| Total | 537 | .4195 | .30115 | .01300 | .3940 | .4451 | .00 | 1.00 | |
| CTE Total | Village | 341 | .3015 | .16632 | .00901 | .2838 | .3193 | .00 | .79 |
| City | 196 | .2631 | .16184 | .01156 | .2403 | .2859 | .00 | .82 | |
| Total | 537 | .2875 | .16559 | .00715 | .2735 | .3015 | .00 | .82 | |
Table 9. The Results of One Way ANOVA for the Differences in Study Variables According to Place
| Sum of Squares | df | Mean Square | F | Sig. | ||
| Direct Exposure | Between Groups | .183 | 1 | .183 | 7.702* | .006 |
| Within Groups | 12.721 | 535 | .024 | |||
| Total | 12.904 | 536 | ||||
| Material Exposure | Between Groups | .020 | 1 | .020 | .610 | .435 |
| Within Groups | 17.276 | 535 | .032 | |||
| Total | 17.296 | 536 | ||||
| Indirect Exposure | Between Groups | .800 | 1 | .800 | 11.553* | .001 |
| Within Groups | 37.065 | 535 | .069 | |||
| Total | 37.865 | 536 | ||||
| Proximate Exposure | Between Groups | .049 | 1 | .049 | .832 | .362 |
| Within Groups | 31.384 | 535 | .059 | |||
| Total | 31.433 | 536 | ||||
| Distant Exposure | Between Groups | .220 | 1 | .220 | 2.427 | .120 |
| Within Groups | 48.390 | 535 | .090 | |||
| Total | 48.609 | 536 | ||||
| CTE Total | Between Groups | .184 | 1 | .184 | 6.794* | .009 |
| Within Groups | 14.513 | 535 | .027 | |||
| Total | 14.697 | 536 | ||||
There are significant differences between respondents from cities and villages in the dimension; Direct Exposure, Indirect Exposure, and CTE total in benefit to villages (p < 0.01). Thus the respondents from villages are more likely to expose to traumatic experiences than respondents from cities.
The differences between the respondents according to areas (Directorates) the researcher used one-way ANOVA test and tables 11 and 12 show the results.
Table 10. The Results of Descriptive statistics For the Study Variables According to Directorate
| Construct | Directorate | N | Mean | S.D. |
| CTE | Jenin | 82 | 0.37 | 0.21 |
| Qabatya | 45 | 0.45 | 0.23 | |
| Nablus | 132 | 0.24 | 0.17 | |
| S. Nablus | 43 | 0.44 | 0.15 | |
| Salfit | 40 | 0.41 | 0.18 | |
| Tubas | 26 | 0.25 | 0.20 | |
| Tulkarm | 103 | 0.27 | 0.18 | |
| Qalqilya | 66 | 0.38 | 0.17 |
Table 11. The Results of One Way ANOVA for the Differences in Study Variables According to Directorate
| Directorate | Source of variance | Sum of Squares | df | Mean Square | F | Sig. |
| CTE | Between Groups | 3.339 | 7 | 0.477 | 13.815** | 0.000 |
| Within Groups | 18.265 | 529 | 0.035 | |||
| Total | 21.604 | 536 |
Figure 2: The Results of Descriptive statistics For the Study Variables According to Directorate
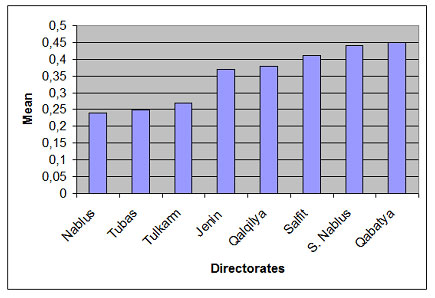
The result of one-way ANOVA test shows there are significant differences among respondents in exposing to traumatic experiences according to directorate (CTE F = 13.82, p < 0.01). The most significant finding in this study was that a high proportion of Palestinian children reported that they had exposed to traumatic experiences; Most of participants had been exposed to all 34 traumatic experiences, there are more than 22% of the participants exposes at least to 15 traumatic experiences from the total of 34 traumatic experiences
The study found that boys suffer more traumatic experiences than girls, which is similar to the findings of many previous studies (Husain et al., 1998; Khamis, 2005; Thabet, Tawahina, El Sarraj, & Vostanis, 2008; Thabet & Vostanis, 1999) (Kuterovac, Dyregrov, & Stuvland, 1994). However, it contrasts with another study that found that boys and girls in Palestine, both of them have the same level of traumatic experiences (Miller, El‐Masri, Allodt, & Qouta, 1999, El-Khodary , Samara 2019a & 2019b), which lead us to understand the difference between traumatic events in Gaza and in the West Bank.
In Gaza we find a general bombing which facilitates the exposure and suffering for everyone, including children, while in the West Bank traumatic events are mostly found in some specific areas; check points, some villages and even houses, as the exposure cannot be experienced by all the population.The results found that the percentage of exposure to traumatic experiences increase for those whom living in the villages than those whom living in the cities, specially in the dimension; Direct Exposure and Indirect Exposure to traumatic events. This is consistent with previous studies ( Thabet & Vostanis, 2000; Thabet, Abed, & Vostanis, 2004; Thabet & Vostanis, 2019).
According to Areas or directorate, there are more exposure to traumatic events on some areas like Qabatya, south Nablus and Salfit, These directorates include many villages and communities as well as their closeness to settlements, military checkpoints, and the apartheid wall, all of these factors might be leading to increase clashes with settlers and soldiers, therefore increased exposure to traumatic events.The war and the long term occupation of Palestinian territory expose students to recurrent traumatic experiences which violate their human rights: the right to live, to learn, to be healthy, to live with his/her family and community, to develop his/her personality, to be nurtured and protected, and the right to enjoy childhood. The potential for having a normal childhood in Palestine is unlikely in the current circumstances and the future psychological well-being of Palestinian children is at risk of being compromised by on-going traumatic experiences.
CONCLUSION
Results show that childhood in the West Bank suffers from traumatic situations; in addition to that the results, which come from Gaza, are worst. Therefore, intervention must go on two directions: 1) stop oppression and aggressive acts that provoke traumatic experiences, and 2) increasing the resistance and resilience of the oppressed population. The current study proves that the surrounding environment of the child has an influence on the development of many kind of mental disorders either as a risk or as a protective factor. The application of the ecological framework theory with children exposed to difficult situations as here involve the relationships between risk and protective factors in the various levels of the ecological model which are the individual (e.g., age, gender), family (e.g., family size, SES), and environment (type and place of residence, citizenship, war trauma and political situation) (El-Khodary Samara & Askew 2020).
At the end, this paper showed how adolescents are affected by Israel occupation, assessed with a questionnaire of traumatic experiences checklist show that the situation is hard, but still bearable comparing to Gaza. This means that oppressed and occupation forces can oppress even more, and also that recovering is easier.Nevertheless, this paper brings the most important point the need to develop appropriate tools to assess traumatic experiences or aggression to adolescents, taking into consideration if the aggression is collective or individual, and the type and frequency, as a way to improve ways to intervene and help to recover.
REFERENCES
Altawil, M. A. S. (2008). The effect of chronic traumatic experience on Palestinian children in the Gaza Strip. (PhD Doctoral dissertation). University of Hertfordshire,
American Psychiatric, A. (2000). diagnostic criteria from dsM-iV-tr: American Psychiatric Pub.
American Psychiatric, A. (2013). Diagnostic and Statistical Manual of Mental Disorders (DSM-5®): American Psychiatric Pub.
Awadh, A. M., Vance, B., El-Beblawi, V., & Pumariega, A. J. (1998). Effects of Trauma of the Gulf War on Kuwaiti Children. Journal of Child & Family Studies, 7(4), 493-498.
Baker, A. M. (1990). The psychological impact of the Intifada on Palestinian children in the occupied West Bank and Gaza: An exploratory study. American Journal of Orthopsychiatry, 60(4), 496.
Barber, B. K. (2009). Making sense and no sense of war: Issues of identity and meaning in adolescents’ experience with political conflict. In Adolescents and war: How youth deal with political violence. (pp. 281-311): Oxford University Press, New York, NY.
Benjamin, L., & Crawford-Browne, S. (2010). The psychological impact of continuous traumatic stress–limitations of existing diagnostic frameworks. Paper presented at the Unpublished paper at a Continuous Traumatic Stress in South Africa Workshop: Department of Psychology, University of Cape Town.
Bonanno, G. A. (2004). Loss, Trauma, and Human Resilience: Have We Underestimated the Human Capacity to Thrive after Extremely Aversive Events? American Psychologist, 59(1), 20-28.
Breslau, J. (2004). Introduction: Cultures of trauma: Anthropological views of posttraumatic stress disorder in international health. Culture, Medicine and Psychiatry, 28(2), 113-126.
Breslau, N., Davis, G. C., & Andreski, P. (1995). Risk factors for PTSD-related traumatic events: A prospective analysis. The American Journal of Psychiatry, 152(4), 529-535.
Daniel, S. P., Jane, C., & Ann, M. (2005). Trauma, proximity, and developmental psychopathology: The effects of war and terrorism on children. Neuropsychopharmacology, 30(10), 1781-1792. doi:10.1038/sj.npp.1300814
Dimitry, L. (2012). A systematic review on the mental health of children and adolescents in areas of armed conflict in the Middle East. Child: Care, Health & Development, 38(2), 153-161. doi:10.1111/j.1365-2214.2011.01246.x
Dubow, E. F., Boxer, P., Huesmann, L. R., Landau, S., Dvir, S., Shikaki, K., & Ginges, J. (2012). Cumulative Effects of Exposure to Violence on Posttraumatic Stress in Palestinian and Israeli Youth. Journal of Clinical Child and Adolescent Psychology, 41(6), 837-844.
Eagle, G., & Kaminer, D. (2013). Continuous traumatic stress: Expanding the lexicon of traumatic stress. Peace and Conflict: Journal of Peace Psychology, 19(2), 85-99. doi:10.1037/a0032485
Elbedour, S., Onwuegbuzie, A. J., Ghannam, J., Whitcome, J. A., & Hein, F. A. (2007). Post-traumatic stress disorder, depression, and anxiety among Gaza Strip adolescents in the wake of the second Uprising (Intifada). Child Abuse & Neglect, 31(7), 719-729.
El-Khodary, B., & Samara, M. (2019). The mediating role of trait emotional intelligence, prosocial behaviour, parental support and parental psychological control on the relationship between war trauma, and PTSD and depression. Journal of Research in Personality, 81, 246-256.
Espié, E., Gaboulaud, V., Baubet, T., Casas, G., Mouchenik, Y., Yun, O., . . . Moro, M. R. (2009). Trauma-related psychological disorders among Palestinian children and adults in Gaza and West Bank, 2005-2008. International Journal Of Mental Health Systems, 3(1), 21-21. doi:10.1186/1752-4458-3-21
Gaboulaud, V., Reynaud, C., Moro, M.-R., Roptin, J., Lachal, C., Brown, V., & Baubet, T. (2010). Psychological support for Palestinian children and adults: an analysis of data from people referred to the Médecins Sans Frontières programme for behavioural and emotional disorders in the occupied Palestinian territory. Apoyo psicosocial para niños y adultos palestinos: un análisis de datos de personas remitidas al programa MSF para trastornos emocionales y de conducta en los Territorios Palestinos Ocupados., 8(2), 131-142.
Garbarino, J., Kostelny, K., & Dubrow, N. (1991). What children can tell us about living in danger. American Psychologist, 46(4), 376.
Hein, F. A., Qouta, S., Thabet, A., & El Sarraj, E. (1993). Trauma and mental health of children in Gaza. BMJ: British Medical Journal, 306(6885), 1130.
Holt, M. (2001). Right of the Child Denied: Palestinian Children under Occupation: Council for the Advancement of Arab-British Understanding.
Kanninen, K., Punamäki, R.-L., & Qouta, S. (2003). Personality and Trauma: Adult Attachment and Posttraumatic Distress Among Former Political Prisoners. Peace and Conflict: Journal of Peace Psychology, 9(2), 97-126. doi:http://dx.doi.org/10.1207/S15327949PAC0902_01
Khamis, V. (2015). Coping with war trauma and psychological distress among school-age Palestinian children. The American Journal Of Orthopsychiatry, 85(1), 72-79. doi:10.1037/ort0000039
Palestinian Center for Human Rights. (2009). Targeted civilians: A PCHR report on the Israeli military offensive against the Gaza strip (27 December 2008 – 12 January 2009). Retrieved from http://www. pchrgaza.org/files/Reports/English/pdf_spec/gazawarreport. pdf.
Palosaari, E., Punamäki, R.-L., Diab, M., & Qouta, S. (2013). Posttraumatic cognitions and posttraumatic stress symptoms among war-affected children: A cross-lagged analysis. Journal of Abnormal Psychology, 122(3), 656-661. doi:16/S0005-7967(99)00123-016/j.janxdis.2009.03.00137/a001694500092676[pii]10.1159/000092676
http://dx.doi.org/10.1037/a0033875
Qouta, S., & El-Sarraj, E. (2004). Prevalence of PTSD among Palestinian children in Gaza Strip. Arabpsynet journal, 2, 8-13.
Qouta, S., Punamäki, R.-L., & Sarraj, E. E. (1995). The relations between traumatic experiences, activity, and cognitive and emotional responses among Palestinian children. International Journal of Psychology, 30(3), 289-304.
Shalhoub‐Kevorkian, N. (2008). The gendered nature of education under siege: a Palestinian feminist perspective. International Journal of Lifelong Education, 27(2), 179-200.
Stevens, G., Eagle, G., Kaminer, D., & Higson-Smith, C. (2013). Continuous traumatic stress: Conceptual conversations in contexts of global conflict, violence and trauma. Peace and Conflict: Journal of Peace Psychology, 19(2), 75-84. doi:10.1037/a0032484
Thabet, A. A., Abu Tawahina, A., El Sarraj, E., & Vostanis, P. (2008). Exposure to war trauma and PTSD among parents and children in the Gaza strip. European Child & Adolescent Psychiatry, 17(4), 191-199. doi:10.1007/s00787-007-0653-9
Thabet, A. A., & Vostanis, P. (2000). Post traumatic stress disorder reactions in children of war: a longitudinal study. Child Abuse & Neglect, 24(2), 291-298.
Thabet, A. A. M., & Vostanis, P. (1999). Post-traumatic Stress Reactions in Children of War. The Journal of Child Psychology and Psychiatry and Allied Disciplines, 40(03), 385-391.
Yule, W. (2000). Posttraumatic stress disorder in the general population and in children. The Journal of clinical psychiatry, 62, 23-28.

