1Master in Sports Pathology and Corrective Exercise, Young Researchers and Elite Club, Borujerd Branch, Islamic Azad University, Borujerd, Iran
2Department of Physical Education and Sports Sciences, Borujerd Branch, Islamic Azad University, Borujerd, Iran
Corresponding author Email: bijan35454@yahoo.com
Article Publishing History
Received: 11/03/2017
Accepted After Revision: 11/06/2017
The aim of the present research was to examine the effect of micro needling therapy on quality of life in women suffering from skin- deep varicose leg. For this purpose 20 patients with varicose veins of the lower limb with the height of 6/1 ± 163/1 cm, weight 4/6 ± 70/1 kg and fat content 6/5 ± 32/4 were selected purposefully, as the subjects. After randomization of subjects into two groups of 10 subjects for 20 weeks, every 4 weeks for a total of 5 sessions a meeting with patients was conducted using Micro needling, the control group did not have any therapeutic intervention. To analyze the data, independent t-test at a significance level of 05/0> P were used. The findings show that between the measured values of quality of life index before and after the test respectively, there is significant increase and a significant reduction of 05/0> P. The results showed that the use of micro-needling can be considered as a safe and effective treatment in enhancing the quality of life in patients with varicose veins of lower limbs.
Varicose Veins, Micro Needling, Quality Of Life
Riyahi V, Goodarzi B. The Effect of Micro Needling Therapy on the Quality of Life in Women Suffering from Skin-Deep Varicose Legs. Biosc.Biotech.Res.Comm. 2017;10(3).
Riyahi V, Goodarzi B. The Effect of Micro Needling Therapy on the Quality of Life in Women Suffering from Skin-Deep Varicose Legs. Biosc.Biotech.Res.Comm. 2017;10(2). Available from: https://bit.ly/2XYn9c2
Introduction
The term Varicose veins which stems from its Latin origin Varix meaning “twisted” refers to dilated veins or swelling of the veins. Varicose veins, is the most common human vascular disease that affects about 20-10% of the population. Varicose veins are veins long, dilated and twisted and which often seen on the interior surfaces of the lower limbs. The highest prevalence of varicose veins is estimated in women aged 49-40 years. Varicose veins are large, fully swollen and sometimes palpable, dilated and elongated, and sometimes higher than 4 mm in diameter. Swollen and web-like varicose veins are very common (Harrie and Kendall 2014).
More than 40 percent of women over 50 have the disease. Varicose veins are skin-deep dilated and zigzagged veins due to structural defects and performance of the saphenous veins or inherent weakness of the vein wall or rarely due to the Artery – IV fistulas. More than 20 million adult Americans suffer from varicose vein disease and the disease causes a sickly condition which results in the reduction of a patient’s performance (Chung, McCray et al. 2000). These veins are related to leg swelling, pain, dermatitis, phlebitis and ulcers, Patients with venous insufficiency often complain of pain in their legs that worsen with prolonged standing and relieved by elevating the feet. On examination of the shank diameter, edema, varicose veins and superficial veins with erythematic, dermatitis, and hyper pigmentation can be seen in the lower leg and the skin near the external ankle might become ulcerous. Mostly, varicose veins are asymptomatic and only regarding beauty aspects require medical attention themselves. If symptomatic, the pain, diffuse and non-specific fullness and heaviness in the legs, especially after standing a long time are probable. Sometimes swelling in the ankles and feet can be seen in the prominent vessels (Chung, McCray et al. 2000).
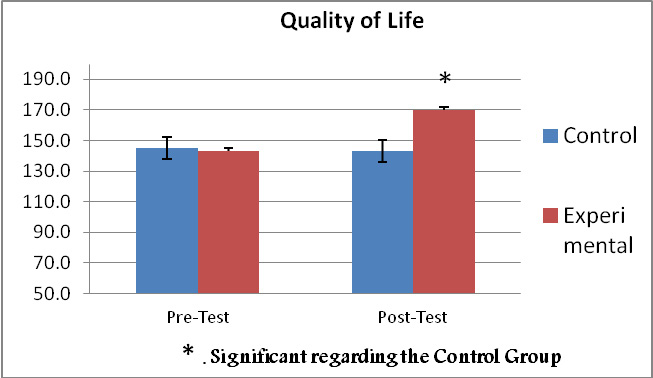 |
Figure 2-4: Comparison of quality of life in both experimental and control groups |
So far, various methods for reducing the symptoms of varicose veins including pain in the legs after prolonged standing or sitting, night pain and feeling of heaviness in the legs are provided. Avoiding long time standing or sitting position, avoiding long-time exposure of legs in the sun and heat or prolonged contact with garter or belt, avoidance of continuous wearing of strip (band) or stockings, avoiding simple sugars and lipids and the use of medications such as Flavonoid derivatives, sodium morrhuate are among the methods of reducing the symptoms of varicose veins (Stiegmann, Sun et al. 1988). Micro needling is a method recently used for skin diseases. Micro needling is a device for general skin needling which has a comparable impact with laser treatments and chemical peelings. This device can be used exclusively or as a complement to other treatment methods. The disposable needles’ points are short and tiny, it includes 12 micro needles that should be discarded after each treatment. For treatment, needle penetration depth must be between 25% to 2/5 mm set with a speed of 25 beats per second and beat for 90 beats per seconds which finally between 300 and 1,000 tiny holes in seconds are created in the surface. Micro needling is used to stimulate the skin to make natural collagen. Furthermore, treatment with this device helps penetration and absorption of drugs to the skin, skin rejuvenation and wrinkles, acne scars healing, improvement of body craze and the overall appearance of the skin and shrinkage of the size of the pores. Backlog and increasing the elasticity of the skin, new collagen production, surface and deep wrinkles reduction, improving crazes, and improving decrements of pigmented lesions’ penetration, materials, creams and vitamins to the skin after treatment with micro needling can be named as the advantages of micro needling (Van Stiegmann and Goff 1988).
The aim of this study is to examine the effect of micro needling on the quality of life in the women suffering from skin-deep varicose foot.
Hypotheses
A 20-week period of micro needling on the surface varicose leg in women has no significant effect on quality of life. A 20-week period micro needling on the surface varicose leg in women has no significant effect on quality of life.
Research Methods
The study population included all women with varicose veins in the age range between 40 to 60 years who have gone to health centers for treatment. The sample consisted of a total of 20 diagnosed women, of those, 10 patients were randomly divided into a control group and 10 other were selected as the experimental group.
After introducing the participants about the purpose of the study, in the first step, measuring pain intensity was performed using questionnaires. After the initial evaluation of samples, micro needling was conducted for 20 weeks and every four weeks for a total of 5 session meetings under the supervision of an expert. It should be noted that the research subjects before the study must not have experience in any use of micro needling. Moreover, the use of any antidepressant medications during the study will be banned and any treatment with these drugs should be avoided for at least 7 days before the study begins. The study regarding the lack of any physical and psychological risks to the subjects will be approved by sports medicine and orthopedic specialists.
Subjects who were 20 patients were divided randomly into two equal groups. Group A: control group, including subjects who during the 20-week study did not have any therapeutic intervention. The second group, the experimental group who used micro needling for 20 weeks and a session for each 4 weeks and a total of 5 sessions. In the present study to determine effects on quality of life of micro needling in two stages: one day before the beginning and one day after the end of the second phase of the 20-week period micro needling was measured using indicators mentioned.
Using deep micro needling (adjustable needle tip 2 mm) by a dermatologist every 4 weeks for 20 weeks and a total of 5 sessions was performed on all the surface varicose veins of the lower limb (Dhurat, et al. 2013) . To evaluate the quality of life, questionnaire FAMAS, Version 2 is used which includes 59 questions under the title of 7 subscales as follows. Motility 7 cases, Symptoms 7 cases, emotional well-being 7 cases, general satisfaction 7 cases, social or family Welfare 7, thinking, and fatigue 9, other concerns 15, and each questionnaire ranges from number zero to the number 236. The questions were in line with the subject and assumptions which after being translated into Persian has been review by several professors and experts and according to them the necessary corrections have been made. It should be noted that in previous studies of content validity of the questionnaire have been made. Regarding the reliability, internal consistency method and Cronbach’s alpha coefficient is studied in a prototype and questions which decrease the reliability (Stability Coefficient) have been modified (Cella, Dineen et al. 1996)
Results and Discussion
In order to classify and regulate the data, descriptive statistics and to analyze the data and raw information inferential statistics are used. In statistical data analysis of the differences of quality of life between the groups, independent t test will be utilized, Paired t-test were used for the detection of pre-test and post-test scores and their significant differences in each group. For statistical analysis, SPSS software was used. At the beginning of the study, after grouping there is no significant differences in age, weight and height of the two groups (0/05> P).
Surveying Normal Data Distribution
To study the normal distribution of data Kolmogorov-Smirnov test was used. According to this test, distribution is normal when the amount is significantly higher than 0/05. The results are provided in table (1-4).
| Table (1-4): Independent t-test for pretest variables | ||
| The significance level | Average and Standard deviation | Variable |
| 0/62 | 5/2±44/5 | Age (years) |
| 0/71 | 6/1±163/1 | Height (Cm) |
| 0/49 | 4/6±70/1 | Weight (kg) |
| 0/81 | 5/6±4/32 | Fat percentage |
Based on the results of Kolmogorov-Smirnov test, distribution data for all studied variables were normal. Therefore, parametric statistical tests were used for data analysis and hypothesis testing.
A 20-week period micro needling has no significant effect on quality of life in women with skin-deep varicose of legs
To check this hypothesis first the statistical paired t-test (paired) were used to compare pre-test and post-test of each group (Table 2-4) and then t-test was used for comparison of independent groups (Table 4-4) at the significant level P ≤.0 / 05.
| Table (2-4): Kolmogorov-Smirnov test results for the variables before and after the test | ||||
| The significance level | Average and Standard deviation | Group | Variables | |
| 491/0 | 2/25±5/145 | pre-Test | Control | Quality of Life |
| 178/0 | 4/22±7/143 | Post-Test | ||
| 491/0 | 6/30±5/143 | Pre-Test | Experimental | |
| 318/0 | 8/28±31/170 | Post-Test | ||
Results showed that the experimental group in post-test after the exercise protocol in comparison to the pre-test show significant difference in the quality of life and because of that the experimental group was significantly increased in the quality of life. But in the control group no significant difference was observed in the quality of life in the pretest and post-test. Also according to the results from the table, in comparing the change in the groups in post-test, significant difference was observed between the changes. Therefore, the null hypothesis of no effect of 20 weeks of micro-needling on the quality of life in the women suffering from skin-deep varicose leg is rejected and it can be stated that this type of intervention is to improve quality of life in these individuals.
| Table 5-4: paired t-test results regarding pretest and posttest of the quality of life | |||||||
| The significance level | t | Degrees of freedom | Within-group mean difference | Post-Test | Pre-Test | Group | Variable |
| 090/0 | 82/0 | 9 | 2/2 | 4/22±7/143 | 2/25±5/145 | Control | Quality of Life |
| 001/0 | 1/6 | 9 | 37/27 | 8/28±31/170 | 6/30±5/143 | Experimental | |
The results of micro needling to enhance quality of life in people with varicose veins might be because microneedle contains 12 short and fine needle with penetration depth of 2 mm and a speed of 25 beats per second to 90 beats per second which ultimately creates between 300 to 1,000 tiny holes in seconds in the surface and it stimulates skin’s natural production of collagen (Pahwa, Pahwa et al. 2012) and leads to ulcer wrinkles removal, improvement of the body crazes, betterment of the overall appearance of the skin and shrinkage of the size of the pores (Majid 2009). In addition, accumulation and increasing elasticity of the skin, new collagen production, surface and deep wrinkles reduction, improvement of body craze and healing of pigmented lesions, happens through micro needling (Aust, Fernandes et al. 2008). Tiny pores made on the skin causes the production of new blood vessels and collagen fibers. Micro needling by stimulating stem cells and fibroblasts in the skin does restorative work in the best way possible. Given that in the skin-deep varicose, faulty and defective veins are at the surface, 20 weeks use of micro needling stimulates vascular and skin tissues, and complications of varicose veins is reduced, thereby enhancing quality of life.
| Table 6-4: results of independent t-test of quality of life in post-test | ||||
| Two-tailed significance level | t | Degrees of freedom | The mean difference between groups | Variable |
| 001/0 | 1/4 | 19 | 17/25 | Quality of life |
The results showed that the use of micro-needling can be used as a safe and effective treatment in enhancing quality of life in patients with varicose veins in lower limbs.
References
- Aust, M. C., D. Fernandes, P. Kolokythas, H. M. Kaplan and P. M. Vogt (2008). Percutaneous collagen induction therapy: an alternative treatment for scars, wrinkles, and skin laxity.Plastic and reconstructive surgery 121(4): 1421-1429.
- Bartsch, T. and P. Goadsby (2005). Anatomy and physiology of pain referral patterns in primary and cervicogenic headache disorders. Headache Currents 2(2): 42-48.
- Cella, D., K. Dineen, B. Arnason, A. Reder, K. Webster, G. Karabatsos, C. Chang, S. Lloyd, F. Mo and J. Stewart (1996). Validation of the functional assessment of multiple sclerosis quality of life instrument. Neurology 47(1): 129-139.
- Chung, C. Y., W. H. McCray, S. Dhaliwal, T. Haywood, M. Black, J.-B. Liu and L. S. Miller (2000). Three-dimensional esophageal varix model quantification of variceal volume by high-resolution endoluminal US. Gastrointestinal endoscopy 52(1): 87-91.
- Cooper, A. and F. Plum (1987). Biochemistry and physiology of brain ammonia. Physiological reviews 67(2): 440-519.
- Crick, S. J., M. N. Sheppard, S. Y. HO, L. Gebstein and R. H. Anderson (1998). Anatomy of the pig heart: comparisons with normal human cardiac structure. Journal of anatomy 193(01): 105-119.
- Dhurat, R., M. Sukesh, G. Avhad, A. Dandale, A. Pal and P. Pund (2013). A randomized evaluator blinded study of effect of microneedling in androgenetic alopecia: a pilot study.” International journal of trichology 5(1): 6.
- Donovan, J. and H. Winfield (1992). Laparoscopic varix ligation. The Journal of urology 147(1): 77-81.
- Gray, H. (2009). Gray’s Anatomy: With original illustrations by Henry Carter, Arcturus Publishing.
- Harrie, R. P. and C. J. Kendall (2014). Case Study 137 Orbital Varix. Clinical Ophthalmic Echography, Springer: 315-315.
- Henwood, T. R., S. Riek and D. R. Taaffe (2008). “Strength versus muscle power-specific resistance training in community-dwelling older adults.” The Journals of Gerontology Series A: Biological Sciences and Medical Sciences 63(1): 83-91.
- Jensen, D., R. Jutabha, T. Kovacs, G. Randall, S. Cheng, M. Freeman, M. Jensen and J. Gornbein (1995). “Endoscopic hemostasis of severe gastric varix hemorrhage in a randomized prospective blinded study of rubber band ligation vS. sclerotherapy.” Gastrointestinal Endoscopy 41(4): 365.
- Katz, A. M. (2010). Physiology of the Heart, Lippincott Williams & Wilkins.
- Lamont, L. A., W. J. Tranquilli and K. A. Grimm (2000). Physiology of pain. Veterinary clinics of North America: Small animal practice 30(4): 703-728.
- Majid, I. (2009). Microneedling therapy in atrophic facial scars: an objective assessment. Journal of cutaneous and aesthetic surgery 2(1): 26.
- Mann, K. G. (1999). Biochemistry and physiology of blood coagulation. Thrombosis and haemostasis 82(2): 165-174.
- Marchand, S. (2008). The physiology of pain mechanisms: from the periphery to the brain.m Rheumatic Disease Clinics of North America 34(2): 285-309.
- Melzack, R. (1975). The McGill Pain Questionnaire: major properties and scoring methods. Pain 1(3): 277-299.
- Melzack, R. (1987). The short-form McGill pain questionnaire. Pain 30(2): 191-197.
- Melzack, R., P. Wall, A. Steptoe and J. Wardle (1994). Pain mechanisms: a new theory. Psychosocial processes and health: A reader: 112-131.
- Pahwa, M., P. Pahwa and A. Zaheer (2012). Tram track effect after treatment of acne scars using a microneedling device. Dermatologic Surgery 38(7pt1): 1107-1108.
- Patel, N. B. (2010). Physiology of pain. Guide to pain management in low-resource settings: 13.
- Rowlands, S. and M. Permezel (1998). 1 Physiology of pain in labour. Baillière’s clinical obstetrics and gynaecology 12(3): 347-362.
- Salavati, M., M. Mazaheri, H. Negahban, S. Sohani, M. Ebrahimian, I. Ebrahimi and A. Kazemnejad (2008). Validation of a Persian-version of Knee injury and Osteoarthritis Outcome Score (KOOS) in Iranians with knee injuries. Osteoarthritis and Cartilage 16(10): 1178-1182.
- Scott, J. and E. Huskisson (1976). Graphic representation of pain.Pain 2(2): 175-184.
- Stiegmann, G., J. Sun and W. Hammond (1988). Results of experimental endoscopic esophageal varix ligation.The American surgeon 54(2): 105-108.
- Van Stiegmann, G. and J. S. Goff (1988). Endoscopic esophageal varix ligation: preliminary clinical experience. Gastrointestinal endoscopy 34(2): 113-117.

