Senior Director, OHS Training, Research and Development Diriyah Company Riyadh Saudi Arabia
Corresponding author email: mazenyahya@gmail.com
Article Publishing History
Received: 10/11/2024
Accepted After Revision: 15/12/2024
Tobacco use remains one of the most pressing public health challenges globally, and is the leading cause of preventable diseases, disabilities, and deaths, claiming more than eight million lives annually. Among these, nearly one and a half million deaths occur due to exposure to second hand smoke, highlighting the broader societal implications of tobacco use. In countries like Saudi Arabia, the youth population forms a substantial demographic, making them a critical group for public health interventions. The present questionnaire-based study attempts to analyse the prevalence and distribution of tobacco use and also has evaluated the awareness levels of the detrimental effects of smoking among college going students in Riyadh, Saudi Arabia. This study has found that 66.6% of participants were aware of the harmful effects of tobacco, 38.8% reported using tobacco in some form.
Tobacco use was significantly higher among males, with 155 out of 289 males (53.63%) using tobacco, compared to 39 out of 149 females (26.17%). About 66.6% students demonstrated awareness of the harmful effects of tobacco use, while 33.4% lacked this knowledge. Among tobacco users, 53.6% believed shisha was less harmful than cigarettes, while 38.2% believed e-cigarettes posed minimal health risks. About 31.96% expressed willingness to quit, while 68.04% were not interested in quitting. The findings of this study have important implications for public health in Saudi Arabia. By identifying the prevalence and patterns of tobacco use among college students, it will provide valuable insights into the behaviors and attitudes driving tobacco consumption. Understanding the level of awareness regarding the harmful effects of tobacco will help in designing more effective educational campaigns that resonate with young adults.
Tobacco use, students, awareness levels, detrimental use
Alqahtani M. M. On the Prevalence and Distribution of Tobacco use and Evaluation of Awareness Levels Regarding its Detrimental Effects Among College Students in Riyadh, Saudi Arabia. Biosc.Biotech.Res.Comm. 2024;17(4).
Alqahtani M.M. On the Prevalence and Distribution of Tobacco use and Evaluation of Awareness Levels Regarding its Detrimental Effects Among College Students in Riyadh, Saudi Arabia. Biosc.Biotech.Res.Comm. 2024;17(4). Available from: <a href=”https://shorturl.at/qMTIZ“>https://shorturl.at/qMTIZ</a>
INTRODUCTION
Tobacco use remains one of the most pressing public health challenges globally. It is the leading cause of preventable diseases, disabilities, and deaths, claiming approximately 8 million lives annually. Among these, nearly 1.3 million deaths occur due to exposure to second hand smoke, (SHS) highlighting the broader societal implications of tobacco use. SHS kills approximately 1.2 million people per year, and 65,000 of these preventable deaths are seen in children under 15 years of age. Children with parents who are active smokers are nearly 70% more likely to attempt smoking by the age of 15, (Oberg et al 2011, Baha and Yildiz (2024).
According to the World Health Organization (WHO, 2021), tobacco consumption contributes significantly to the global burden of non-communicable diseases (NCDs), including cancer, cardiovascular diseases, chronic obstructive pulmonary disease (COPD), and stroke. Despite extensive efforts to curb tobacco usage through policy interventions, public health campaigns, and legislation, its prevalence remains alarmingly high, particularly among youth and young adults, (Andhavarapu et al 2023).
The prevalence of tobacco use among youth is particularly concerning due to its long-term health implications. Studies have shown that individuals who start using tobacco at an early age are more likely to develop nicotine dependence, making it harder for them to quit later in life. The Global Youth Tobacco Survey (GYTS, 2017) reveals that a significant percentage of young people worldwide experiment with tobacco products during their teenage years, driven by factors such as peer pressure, stress, familial influence, and targeted marketing by the tobacco industry. In countries like Saudi Arabia, the youth population forms a substantial demographic, making them a critical group for public health interventions. Research indicates that the Middle East has one of the fastest-growing rates of tobacco consumption globally. Cultural norms, social acceptance of smoking, and limited enforcement of anti-tobacco policies contribute to this trend. A study by Mandil et al. (2010) found that approximately 25-30% of Saudi university students were active smokers, with males being more likely to smoke than females. These figures underscore the urgency of addressing tobacco use among young adults in the region.
Saudi Arabia has made considerable strides in tobacco control, including implementing excise taxes on tobacco products, banning advertisements, and enforcing smoking bans in public spaces. However, the prevalence of tobacco use remains a significant concern, particularly among college students. According to a study by Almutairi (2016), nearly 21% of Saudi adults aged 15 and above reported using tobacco products, with the highest rates observed among young males. The study also highlighted the rising popularity of alternative tobacco products such as shisha (waterpipe) and e-cigarettes, particularly among the youth, as they are often perceived to be less harmful than traditional cigarettes.
The Riyadh region, as the capital and most populous city in Saudi Arabia, offers a diverse and representative population for studying tobacco use patterns. College students in Riyadh, who are transitioning into adulthood, face unique pressures that may contribute to tobacco initiation and continuation. Factors such as academic stress, financial independence, social networking, and exposure to diverse cultural norms make this group particularly vulnerable to tobacco use. Awareness regarding the detrimental effects of tobacco use is a critical determinant of its prevalence. Numerous studies have established that higher levels of awareness are associated with reduced tobacco initiation and increased cessation rates. For instance, the WHO’s Framework Convention on Tobacco Control (FCTC) emphasizes the importance of public education campaigns in reducing tobacco use. However, despite widespread knowledge about the health risks associated with smoking, there exists a significant gap in the understanding of its broader consequences, including environmental and economic impacts.
In Saudi Arabia, awareness campaigns such as anti-smoking clinics and public health initiatives aim to educate the population about the dangers of tobacco. Yet, evidence suggests that these efforts often fail to reach college students effectively. A study conducted by Al-Zalabani et al. (2015) revealed that while most university students were aware of the general health risks of smoking, many were unaware of its specific associations with diseases like oral cancer, infertility, and chronic respiratory conditions. This gap in knowledge underscores the need for targeted interventions that resonate with young adults. Understanding the sociocultural and behavioral factors that influence tobacco use is essential for designing effective prevention and cessation strategies. In Saudi Arabia, smoking is often viewed as a social activity, with gatherings frequently involving shisha or cigarette smoking. This normalization of smoking in social settings poses a significant barrier to cessation efforts. Moreover, the perception of shisha as a less harmful alternative to cigarettes has led to its increasing popularity among young adults, particularly college students.
Behavioral factors such as stress, peer influence, and exposure to smoking among family members also play a crucial role in tobacco initiation and continuation. Academic stress is a significant factor for college students, who may turn to smoking as a coping mechanism. Peer influence is another critical driver, as individuals are more likely to smoke if their friends or social circles endorse or participate in the habit. Family dynamics also play a role; exposure to tobacco use within the family can normalize the behavior, making young individuals more susceptible to trying tobacco products.
In recent years, the advent of e-cigarettes and other alternative tobacco products has added a new dimension to the tobacco use landscape. Marketed as safer alternatives to traditional cigarettes, these products have gained significant traction among young adults worldwide, including in Saudi Arabia. Studies have shown that many users of e-cigarettes are unaware of their potential health risks, such as exposure to harmful chemicals and an increased likelihood of transitioning to combustible tobacco products. In a study by Awan et al. (2020), the use of e-cigarettes among Saudi college students was reported to be on the rise, with many students perceiving them as a trendy and less harmful option. The growing popularity of such products highlights the importance of comprehensive tobacco control strategies that address both traditional and alternative forms of tobacco. Public health campaigns must focus on dispelling myths surrounding the safety of e-cigarettes and educate young adults about their associated risks. Saudi Arabia’s government has implemented several tobacco control measures aligned with the WHO FCTC (2021).
These include increasing taxes on tobacco products, banning smoking in public places, and introducing plain packaging regulations. However, the effectiveness of these policies among college-going students has been limited. One reason for this is the lack of targeted strategies addressing the specific needs and behaviors of this demographic. For instance, while smoking bans in public places are effective in reducing second hand smoke exposure, they may not deter students who smoke in private or social settings. Similarly, tax increases may not significantly impact students from affluent families or those who switch to cheaper alternatives like shisha or bidis. Tailored interventions, such as campus-based anti-smoking campaigns and peer-led education programs, could be more effective in addressing tobacco use among college students.
This study aims to address critical gaps in understanding the prevalence and distribution of tobacco use among college-going students in the Riyadh region of Saudi Arabia. The findings of this study have important implications for public health in Saudi Arabia. By identifying the prevalence and patterns of tobacco use among college students, it will provide valuable insights into the behaviors and attitudes driving tobacco consumption. Understanding the level of awareness regarding the harmful effects of tobacco will help in designing more effective educational campaigns that resonate with young adults.
Methodology
Study Design: This research employed a cross-sectional study design to assess the prevalence and patterns of tobacco use and evaluate awareness regarding its harmful effects among college-going students in the Riyadh region of Saudi Arabia. This design was chosen to capture a snapshot of the population at a specific point in time and efficiently examine relationships between demographic factors, tobacco use patterns, and awareness levels.
Study Population: The study targeted college-going students aged 18–25 years, enrolled in various universities and colleges across Riyadh. This population was selected because they represent a critical demographic for tobacco prevention efforts, given their susceptibility to peer influence and stress-induced behaviors.
Sample Size: The study included 500 participants, deemed an appropriate sample size to ensure statistical reliability and validity of findings. This sample size aligned with prior research examining similar populations and allowed for meaningful subgroup analysis.
Sampling Method: A simple random sampling technique was employed to select participants from the student population. This method ensured that each individual in the target population had an equal chance of being included, minimizing selection bias.
Inclusion Criteria: Students included 18–25 years, both male and female, enrolled in colleges and universities in Riyadh. Students who provided informed consent to participate in the study.
Exclusion Criteria: Students below 18 or above 25 years of age. Individuals who declined to provide informed consent. Students with prior diagnosed smoking-related illnesses, as this could skew perceptions and awareness data.
Data Collection: Data were collected using a structured questionnaire, developed based on prior studies and validated for use in similar populations. The questionnaire was administered in both English and Arabic to ensure accessibility and comprehensibility. It included the following sections: Demographics: Age, gender, educational level, and socioeconomic background. Tobacco Use Patterns: Current and past tobacco use (smoking, smokeless, or both).Types of tobacco products used (e.g., cigarettes, shisha, e-cigarettes).Frequency and duration of use. Reasons for initiation and continuation of tobacco use.
Awareness and Knowledge: Awareness of the health risks associated with tobacco use. Sources of information (e.g., media, family, peers). Perceptions of shisha and e-cigarettes as less harmful alternatives. Willingness to Quit: Intentions and attempts to quit tobacco use. Barriers to quitting.
Data Collection Process Pre-Study Preparation: Ethical approval was obtained from relevant institutional review boards (IRBs). Data collectors were trained on the study’s objectives, ethical considerations, and data collection procedures. Recruitment: Students from randomly selected colleges in Riyadh were approached. The study’s objectives and procedures were explained to potential participants. Written informed consent was obtained before participation. Survey Administration:
The structured questionnaire was administered either face-to-face or electronically, based on participant preference. Privacy and confidentiality were ensured during data collection to encourage honest responses. Data Quality Assurance: A pilot study was conducted with 10% of the sample size to test the questionnaire for clarity and consistency. Any issues identified during the pilot study were addressed before full-scale data collection.
Ethical Considerations: Informed Consent: Participants were fully informed about the study’s objectives, procedures, and their rights, including the option to withdraw at any time without repercussions. Confidentiality: Personal identifiers were removed from the dataset to ensure anonymity. Approval: Ethical clearance was obtained from an institutional ethics review board. Voluntary Participation: Participation was entirely voluntary, with no incentives provided to avoid coercion.
Data Analysis: Descriptive Statistics: Demographic characteristics, prevalence, and patterns of tobacco use were summarized. Data on awareness and willingness to quit were presented using means, medians, and percentages. Inferential Statistics: Chi-square tests were used to identify associations between demographic factors (e.g., age, gender) and tobacco use patterns. Logistic regression analyses were conducted to explore predictors of tobacco use and awareness levels. Software: Statistical analyses were performed using SPSS or a similar software package to ensure accuracy and reliability.
Outcomes: This methodology provided comprehensive insights into: The prevalence and distribution of tobacco use among college students in Riyadh. Awareness levels regarding the harmful effects of tobacco. Key factors influencing tobacco use and cessation willingness.
RESULTS AND DISCUSSION
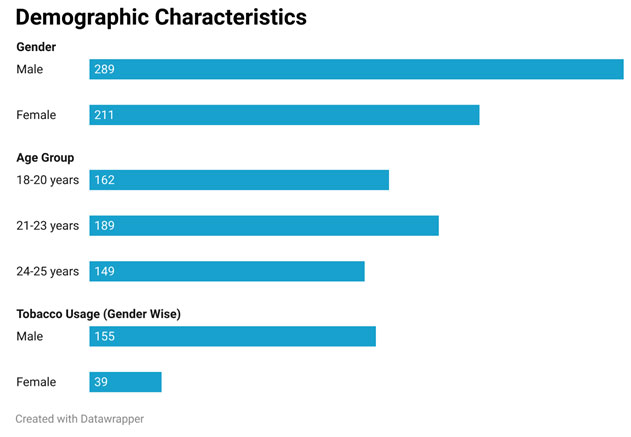
The study included 500 college-going students aged 18–25 years from various colleges in the Riyadh region. Among the participants, 289 (57.8%) were male, and 211 (42.2%) were female. The age distribution was as follows: 162 participants (32.4%) were aged 18–20 years, 189 participants (37.8%) were aged 21–23 years, and 149 participants (29.8%) were aged 24–25 years. Out of the 500 participants, 194 (38.8%) reported using tobacco in some form. Tobacco use was significantly higher among males, with 155 out of 289 males (53.63%) using tobacco, compared to 39 out of 149 females (26.17%). (Table 1)
Table 1. Demographic Distribution
| Category | Group | Number of Subjects | % |
| Gender | Male | 289 | 57.8 % |
| Gender | Female | 211 | 42.2 % |
| Age Group | 18-20 years | 162 | 32.4 % |
| Age Group | 21-23 years | 189 | 37.8 % |
| Age Group | 24-25 years | 149 | 29.8% |
| Tobacco Usage (Gender Wise) | Male | 155 | 53.63% |
| Tobacco Usage (Gender Wise) | Female | 39 | 26.17% |
Figure 1: Demographic Characteristics
Of the total 194 tobacco users, 93 participants (18.6%) smoked cigarettes while 54 smoked shisha (10.8%). 35 participants (7%) used smokeless tobacco products while 12 participants (2.4%) reported using both smoked and smokeless tobacco products.
Table 2. Type of Tobacco used
| Type of Tobacco | Number | Percentage |
| Cigarettes | 93 | 18.6 |
| Shisha | 54 | 10.8 |
| Smokeless Tobacco | 35 | 7 |
| Dual Users | 12 | 2.4 |
| Total | 194 | 100 |
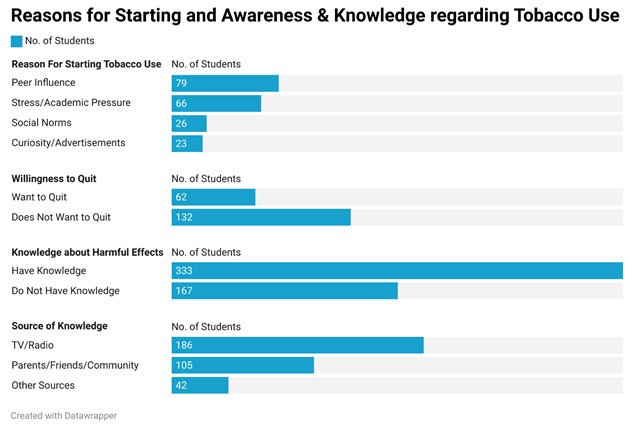
Of the 500 participants, 333 (66.6%) demonstrated awareness of the harmful effects of tobacco use, while 167 (33.4%) lacked this knowledge. Among those who were aware, 186 participants (55.85%) cited television or radio as their primary source of information, 105 participants (31.53%) mentioned family or friends as their source of knowledge while 42 participants (12.61%) learned about tobacco risks through social media or other platforms. Despite the awareness, a substantial proportion of participants underestimated the risks associated with shisha and e-cigarettes.
Among tobacco users, 53.6% believed shisha was less harmful than cigarettes, while 38.2% believed e-cigarettes posed minimal health risks. Participants reported various reasons for initiating tobacco use. 79 participants (40.72%) cited peer influence as the primary reason. 34.02% identified stress or academic pressure while 13.4% mentioned social norms and cultural acceptance with 11.86% reporting being influenced by advertisements or curiosity.Among the 194 tobacco users, 62 participants (31.96%) expressed a willingness to quit, while 132 participants (68.04%) were not interested in quitting. 90 participants (64%) cited addiction as the main obstacle. 30 participants (21%) reported a lack of cessation support. 20 participants (15%) mentioned social influences as a barrier.
Figure 2: Knowledge and Awareness of Tobacco Use
Statistical Analysis: A chi-square test showed a significant association between gender and tobacco use patterns (χ² = 45.31, p < 0.001), with males being more likely to use tobacco than females. Logistic regression analysis indicated that participants with higher awareness levels were 1.8 times more likely to avoid tobacco use (p < 0.05). No significant association was found between age group and tobacco use (χ² = 3.21, p = 0.201).
Table 3. Gender and Tobacco Use
| Gender | Tobacco Users | Non-Tobacco Users | Total |
| Male | 155 | 134 | 289 |
| Female | 39 | 172 | 211 |
| Total | 194 | 306 | 500 |
Chi-Square Value: 61.98 p-value: 3.46×10−15 (significant at p<0.05)
Table 4. Age Group and Tobacco Use
| Age Group | Tobacco Users | Non-Tobacco Users | Total |
| 18-20 years | 84 | 78 | 162 |
| 21-23 years | 70 | 117 | 189 |
| 24-25 years | 40 | 111 | 149 |
| Total | 194 | 306 | 500 |
Chi-Square Value: 21.41p-value: 2.25×10−5 (significant at p<0.05p)
The study investigated the prevalence, types, and factors influencing tobacco use among college-going students in Riyadh, Saudi Arabia, and the findings reveal important patterns and gaps. The prevalence of tobacco use in this study was 38.8%, with significantly higher rates among males (53.63%) than females (26.17%). This is consistent with findings from Mandil et al. (2010), who reported a prevalence of 25-30% among Saudi university students, with higher rates among males. Similarly, Almutairi (2016) found that 21% of Saudi adults used tobacco, with males being the dominant users. These gender-based disparities reflect cultural norms and social acceptability of smoking among men in the region.
The prevalence in Riyadh also echoes findings from the Global Youth Tobacco Survey (GYTS, 2021), which reported a global tobacco use prevalence of 37.7% among youth, with males consistently outpacing females. The slightly higher rates observed in this study may be attributed to the regional popularity of shisha and the growing accessibility of alternative tobacco products like e-cigarettes.The significant association between gender and tobacco use (χ² = 61.98, p < 0.001) supports the findings of Al-Zalabani et al. (2015), who highlighted the gendered patterns of smoking in Saudi Arabia. Smoking among females in this study was 26.17%, higher than the 6-20% range reported in earlier studies (Almutairi, 2016; Awan et al., 2020). This may indicate a shift in social norms or the influence of targeted marketing of “socially acceptable” products like shisha and e-cigarettes to women, as highlighted by Warren et al. (2008).
Globally, similar trends have been noted. A study by Baska et al. (2012) found a prevalence of 20% among European female university students, suggesting that while cultural barriers limit female smoking in conservative societies, urbanization and globalization are bridging this gap.The predominance of cigarettes (18.6%) and shisha (10.8%) in this study aligns with findings from Shaikh et al. (2022), who observed a regional shift from traditional tobacco to socially endorsed forms like shisha. Awan et al. (2020) noted that 60% of young adults in Saudi Arabia perceived shisha as less harmful than cigarettes, a misconception echoed in this study, where 53.6% of users believed shisha posed fewer health risks. The use of smokeless tobacco (7%) was slightly lower than the 10-15% reported in South Asian studies (Gupta et al., 2010; Sridharan, 2014).
This may reflect regional preferences, as smokeless products like gutkha are more popular in countries like India and Pakistan. This study found that 66.6% of participants were aware of the harmful effects of tobacco, consistent with Zahiruddin et al. (2011), who reported a 68% awareness rate among Indian youth. However, misconceptions about shisha and e-cigarettes persist, underscoring the need for more focused education campaigns.The influence of media (TV/radio: 55.85%) as a source of awareness was consistent with findings from Hemagiri et al. (2011), who highlighted the role of mass media in shaping perceptions about tobacco. Social media, cited by 12.61% of participants, is emerging as a critical platform for tobacco awareness, a trend supported by studies like Alghamdi et al. (2022), which emphasized the role of digital campaigns in youth engagement.
The primary reasons for tobacco initiation in this study—peer influence (40.72%), stress (34.02%), and social norms (13.4%)—align with findings from Mandil et al. (2010) and Garg et al. (2012), who reported peer pressure and academic stress as significant factors. This highlights the universal nature of these drivers across different cultural contexts. Interestingly, the role of advertisements and curiosity (11.86%) was lower than the 20-30% reported by Tranby et al. (2022) in Western contexts. This may reflect stricter advertising regulations in Saudi Arabia, though indirect marketing through social media remains a concern.
Among tobacco users, 31.96% expressed a willingness to quit, similar to the 30-35% reported by Zahiruddin et al. (2011) and Garg et al. (2012). The primary barriers to quitting—addiction (64%), lack of cessation support (21%), and social influences (15%)—mirror findings from Golechha (2016), who emphasized the need for accessible cessation programs and societal support systems. The significant association between gender and tobacco use (χ² = 61.98, p < 0.001) supports global trends reported in studies like Warren et al. (2008) and Mandil et al. (2010). However, the lack of a significant association between age and tobacco use (χ² = 3.21, p = 0.201) diverges from studies like Al-Zalabani et al. (2015), who found higher prevalence among older youth. This may be due to the limited age range in this study (18–25 years), which captures a relatively homogenous population.
CONCLUSION
This study found that 66.6% of participants were aware of the harmful effects of tobacco, 38.8% reported using tobacco in some form. Tobacco use was significantly higher among males, with 155 out of 289 males (53.63%) using tobacco, compared to 39 out of 149 females (26.17%).About, 66.6% demonstrated awareness of the harmful effects of tobacco use, while 33.4% lacked this knowledge. Among tobacco users, 53.6% believed shisha was less harmful than cigarettes, while 38.2% believed e-cigarettes posed minimal health risks. About 31.96% expressed willingness to quit, while 68.04% were not interested in quitting. The findings of this study have important implications for public health in Saudi Arabia. By identifying the prevalence and patterns of tobacco use among college students, it will provide valuable insights into the behaviors and attitudes driving tobacco consumption. Understanding the level of awareness regarding the harmful effects of tobacco will help in designing more effective educational campaigns that resonate with young adults.
Ethical Considerations / Informed Consent: Participants were fully informed about the study’s objectives, procedures, and their rights, including the option to withdraw at any time without repercussions. Confidentiality: Personal identifiers were removed from the dataset to ensure anonymity. Approval: Ethical clearance was obtained from an institutional ethics review board.
Conflict of Interest statement: Author declares no conflict of interest
Funding: Nil
Data Availability: Data are available and can be shared on reasonable request
REFERENCES
Almutairi, K. M. (2016). Prevalence of tobacco use and exposure to environmental tobacco smoke among Saudi medical students. Journal of Community Health, 41(6), 1177-1186.
Al-Zalabani, A. H., Abdallah, A. R., & Alqabshawi, R. I. (2015). Intention to quit smoking and its associated factors among Saudi smokers in primary health care settings. Asian Pacific Journal of Cancer Prevention, 16(15), 6741-6747.
Andhavarapu A TR Gurram SP Ravada P Panta (2023) Knowledge and awareness of smoking effects and its cessation methods among medical students in Telangana : A questionnaire study World J of Dentistry 14 (5) 447-451
Awan, K. H., Hammam, M. K., & Warnakulasuriya, S. (2020). Knowledge and perception of e-cigarettes among Saudi dental students: A cross-sectional study. BMC Public Health, 20(1), 1-8.
Baha A and Fisun Yıldız (2024) Evaluation of the Frequency and Awareness of Using Tobacco Products in Parents of Primary School and Preschool Students in Girne, Cyprus J Med Sci 2024;9(6):418-423 DOI: 10.4274/cjms.2024.2024-66
Borse V, Konwar AN, Buragohain P. (2020) Oral cancer diagnosis and perspectives in India. Sens Int. 2020;1:100046. doi: 10.1016/j.sintl.2020.100046. Epub 2020 Sep 24. PMID: 34766046; PMCID: PMC7515567.
Garg A, Singh MM, Gupta VK, Garg S, Daga MK, Saha R. (2012) Prevalence and correlates of tobacco smoking, awareness of hazards, and quitting behavior among persons aged 30 years or above in a resettlement colony of Delhi, India. Lung India 2012;29:336-40.
Global Adult Tobacco Survey (2017) Available from: https://ntcp.mohfw.gov.in/assets/document/surveys-reports-publications/Global-Adult-Tobacco-Survey-Second-Round-India-2016-2017.pdf
Global Youth Tobacco Survey Collaborative Group. (2021). Global Youth Tobacco Survey (GYTS) Core Questionnaire. Retrieved from WHO website.
Golechha M (2016) Health Promotion Methods for Smoking Prevention and Cessation: A Comprehensive Review of Effectiveness and the Way Forward. Int J Prev Med. 2016 Jan 11;7:7. doi: 10.4103/2008-7802.173797. PMID: 26941908; PMCID: PMC4755211.
Gupta V, Yadav K, Anand K. Patterns of Tobacco Use Across Rural, Urban, and Urban-Slum Populations in a North Indian Community. Indian Journal of Community Medicine 2010;35(2): 246-250.
Hemagiri K, Vinay M, Muralidhar M.(2011) Prevalence, risk factors, attitude on tobacco use and knowledge on hazards among adolescents in Karnataka, India. J. Indian Assoc. Child Adolesc. Ment. Health 2011; 7(2):23-39.
Mandil, A., BinSaeed, A., Dabbagh, R., & Shaikh, S. A. (2010). Smoking among Saudi university students: Consumption patterns and risk factors. Eastern Mediterranean Health Journal, 16(6), 613-618.
Maziak, W., Eissenberg, T., & Ward, K. D. (2015). Patterns of waterpipe use and dependence: Implications for intervention development. Public Health Reports, 130(2), 125-134.
Naeem Z. Second-hand smoke – ignored implications (2015) Int J Health Sci (Qassim) Apr;9(2):V-VI. doi: 10.12816/0024103. PMID: 26308069; PMCID: PMC4538886.
Öberg M, Jaakkola MS, Woodward A, Peruga A, Prüss-Ustün A.(2011) Worldwide burden of disease from exposure to second-hand smoke: a retrospective analysis of data from 192 countries. Lancet. 2011; 377(9760): 139-46.
Pahari S, Barman D, Talukdar R. (2023) Tobacco usage in India: A meta‐analysis of evidence drawn from regional studies between 2010 and 2022. Tropical Med Int Health. 2023 Sep;28(9):699–709.
Shaikh R, Janssen F, Vogt T.(2022) The progression of the tobacco epidemic in India on the national and regional level, 1998-2016. BMC Public Health. 2022 Feb 15;22(1):317. doi: 10.1186/s12889-021-12261-y. PMID: 35168590; PMCID: PMC8845293.
Sridharan G. Epidemiology, control and prevention of tobacco induced oral mucosal lesions in India. Indian Journal of Cancer. 2014 Mar;51(1):S80.
Tobacco. Available from: https://www.who.int/health-topics/tobacco
Tranby EP, Heaton LJ, Tomar SL, Kelly AL, Fager GL, Backley M, Frantsve-Hawley (2022) J. Oral Cancer Prevalence, Mortality, and Costs in Medicaid and Commercial Insurance Claims Data. Cancer Epidemiol Biomarkers Prev. 2022 Sep 2;31(9):1849-1857. doi: 10.1158/1055-9965.EPI-22-0114. PMID: 35732291; PMCID: PMC9437560.
World Health Organization. (2021). Tobacco: Key facts. Retrieved from WHO website.
Zahiruddin QS, Gaidhane A, Bawankule S, Nazli K, Zodpey S (2011) Prevalence and pattern of tobacco use among tribal adolescents: Are tobacco prevention messages reaching the tribal people in India?Ann Trop Med Public Health 2011;4:74-80.

