1,4MPT (Orthopaedics), College of Physiotherapy, PGIMS, Rohtak, India
2MPT (Sports), College of Physiotherapy, PGIMS, Rohtak, India
3Assistant Professor, College of Physiotherapy, PGIMS, Rohtak, India
Corresponding author email: kusumyadav910@gmail.com
Article Publishing History
Received: 15/01/2023
Accepted After Revision: 25/03/2023
Processing of sensory input entails recognizing, categorizing, and interpreting data to generate an adaptive reaction. The sensory sub-types include barognosis, stereognosis, graphesthesia, two-point discrimination, and tactile localization. Stereognosis is the capacity to recognise the form and shape of a three-dimensional item and, consequently, its identity, by tactile manipulation of that object in the absence of visual and aural inputs. Therefore, manual stereognosis is necessary for integrating all hand sensations. So, the aim of this study is to determine the normal reaction time of manual stereognosis in adults.A pilot cross-sectional study was done on age group of 18-40 years. The stereognosis test was performed first on dominant hand and then on non-dominant hand using 5 objects (key, coin, safety pin, comb, pencil) with participant’s eyes closed during the test.
The time taken to identify the objects was recorded using stopwatch. Then, mean normal reaction time was calculated. Student t-test was used to compare any differences between right & left-hand side stereognosis and between male & female gender.Results from the study show normal mean values of reaction time in seconds was 3.04 for right hand and 2.09 for left hand in adults. Data also shows that there were statistically significant differences between right & left-hand side stereognosis. However, no differences were found between male and female stereognosis using independent t-test.These normative results of data will serve as a useful, simple, reproducible, rapid assessment of stereognosis and also aid in planning of treatment.
Adults, Hand Skills, Normative Values, Stereognosis, Sensory Integration.
Malika, Kusum, Choudhry D, Kumar P. Normative Reference Value for Stereognosis Among Adult Population: A Cross-Sectional Pilot Study. Biosc.Biotech.Res.Comm. 2023;16(1).
Malika, Kusum, Choudhry D, Kumar P. Normative Reference Value for Stereognosis Among Adult
Population: A Cross-Sectional Pilot Study. Biosc.Biotech.Res.Comm. 2023;16(1). Available from: <a href=”https://bit.ly/3xmuiTB“>https://bit.ly/3xmuiTB</a>
INTRODUCTION
Processing of sensory input entails recognizing, categorizing, and interpreting data to generate an adaptive reaction. Kilroy (2019) Exteroceptive and interoceptive functions of somatosensory system govern how we perceive and react to stimuli coming from outside and inside the body, respectively. Abraira (2013) There are 3 categories of sensations i.e., superficial feeling, deep experience and integrated cortical sensations. The sensory sub-types include barognosis, stereognosis, graphesthesia, two-point discrimination, and tactile localization, Spillane (2013).Stereognosis is a complex and multi-faceted evaluation that is typically included in the sensory examination. Carlson (2009) Stereognosis is the ability to recognise the form and shape of a three-dimensional item and, consequently, its identity, by tactile manipulation of that object in the absence of visual and aural inputs, Fujii (2015).
In order to obtain discriminative touch and proprioceptive information, manual stereognosis requires healthy peripheral sensory pathways, specifically the dorsal column-medial lemniscus tract (DCMLT). Receiving this information is necessary but insufficient for stereognosis because parietal lobe cortex’s processing centres must be operational as well. The deterioration of this ability can be detrimental, especially in tasks requiring fine motor skills, as impaired stereognosis is linked to decreased manual dexterity in people, Schermann (2021).
Therefore, manual stereognosis is necessary for integrating all hand sensations. Stroke is commonly the cause of manual stereognosis impairment, which has a debilitating effect. Fujii (2015) According to Reitan and Wolfson, stereognosis varies between individuals with brain injury and their unaffected peers. Reitan (2002) Other researchers have reported stereognosis impairments to differing degrees (42% to 97%) and have pushed for adding stereognosis ability as a crucial evaluation factor. Goldner (1966) & Van Heest (1993) Because the hand cannot receive and perceive information from the environment, decreased stereognosis is considered to predict limited functional capacity. Carlson (2009) Many assessment methods employ stereognosis as a measure of the upper extremity’s functional potential, with lower stereognosis suggesting a lower possibility of functional improvements following surgery, Goldner (1966) , Van Heest (1993), Zancolli (1983), Hoffer (1988), Thometz (1988).
To compare the value of stereognosis in affected people with normal value, main focus of the study is to determine the normal reaction time of manual stereognosis in adults. These normative results of data will serve as useful, simple, reproducible, rapid assessment of stereognosis and also aid the planning of treatment. Normative value of stereognosis is important to check hand sensory functions. There was no standard normative reference value available for stereognosis among adults. Hence to fill this gap in the knowledge, the need of this study was to establish the normative value of stereognosis among adults of age 20-40 years. This study will also help to recognise abnormal sensory function of hand in diseased individuals by comparing it with normative values of stereognosis in normal individuals. The aim of the present study is to find the normative reference value of stereognosis in adults. The objective was to compare normative reference value of stereognosis between right and left hand side and male & female participants.
MATERIAL AND METHODS
This study was a pilot cross-sectional study conducted at College of Physiotherapy, PGIMS Rohtak. This study was done on 40 adults individuals with age group 20-40 years in which 16 males and 24 females were included. There was 3 people with left hand dominance and 37 with right hand dominance. Convenient sampling method was used to recruit the subjects. Duration of study was 2 months. Inclusion criteria: Both male and female participants who were willing to participate in the study were selected with age group of 20-40 years. Exclusion criteria: Participants with neurological illness, any congenital deformity of hand, with recent hand injuries and fractures, with psychological condition that interferes with the test were excluded from the study. Materials used: Paper, Table, Chair, Pen, Stopwatch, Key, Pencil, Comb, Coin, Safety pin.
The procedure of stereognosis was explained to the participants. Participants were sitting in comfortable position with eyes closed. The stereognosis test included 5 daily used objects i.e., key, coin, pencil, comb and safety pin. Each object was placed separately first in dominant hand and then in non-dominant hand. The time taken to identify the objects was recorded using stopwatch. The test was repeated 3 times to obtain an average value and 1 min rest was given between each reading, Kinnucan (2010).
The SPSS statistical package (version 25.0) was used to analyse the data. Descriptive statistics was used to calculate the mean and standard deviation of time taken to identify various objects. Student independent t-test was used to find any difference between right- & left-hand side and gender difference between male & females. For all statistical tests, a p-value ≤ 0.05 was taken as a significant difference.
RESULTS AND DISCUSSION
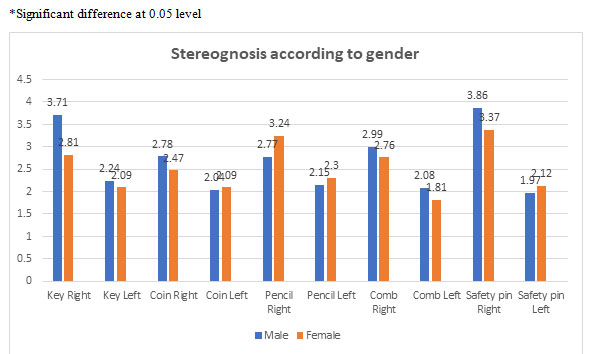
There were 16 males with mean age 27.48±5.35 years and 24 females with mean age 26.76±4.84 years. Table 1 shows mean±SD value of stereognosis with various objects for right & left hand side and also shows that there was statistically significant difference in stereognosis between right & left hand side with various objects i.e., key, coin, pencil, comb and safety pin (p≤0.05). Table 2 shows mean±SD value of stereognosis using various objects in both male & female and no statistically significant difference between male and female stereognosis with various objects i.e., key, coin, pencil, comb and safety pin (p≥0.05). Figure 1 represents bar graph showing comparison of stereognosis mean value between male and female participants.
Table 1: Comparison of right and left hand side stereognosis using independent t-test
| Stereognosis | Right | Left | t-value | p-value | ||
| Mean | SD | Mean | SD | |||
| Key | 3.17 | 2.74 | 2.15 | 0.64 | 2.30 | 0.02* |
| Coin | 2.59 | 0.89 | 2.07 | 0.67 | 2.95 | 0.00* |
| Pencil | 3.05 | 1.50 | 2.24 | 0.92 | 2.90 | 0.01* |
| Comb | 2.85 | 1.31 | 1.92 | 0.77 | 3.88 | 0.00* |
| Safety pin | 3.56 | 1.85 | 2.06 | 0.73 | 4.80 | 0.00* |
* Significant difference at 0.05 level
Table 2. Comparison of male and female stereognosis using independent t-test
| Stereognosis | Male (16) | Female (24) | t-value | p-value | |||
| Mean | SD | Mean | SD | ||||
| Key | Right | 3.71 | 4.18 | 2.81 | 0.98 | 1.08 | 0.32 |
| Left | 2.24 | 0.81 | 2.09 | 0.50 | 0.71 | 0.48 | |
| Coin
|
Right | 2.78 | 1.21 | 2.47 | 0.59 | 1.09 | 0.28 |
| Left | 2.04 | 0.88 | 2.09 | 0.50 | 0.26 | 0.80 | |
| Pencil
|
Right | 2.77 | 1.65 | 3.24 | 1.40 | 0.96 | 0.34 |
| Left | 2.15 | 0.89 | 2.30 | 0.95 | 0.50 | 0.62 | |
| Comb
|
Right | 2.99 | 1.55 | 2.76 | 1.15 | 0.50 | 0.60 |
| Left | 2.08 | 1.10 | 1.81 | 0.44 | 1.07 | 0.29 | |
| Safety pin | Right | 3.86 | 2.52 | 3.37 | 1.23 | 0.83 | 0.41 |
| Left | 1.97 | 0.95 | 2.12 | 0.56 | 0.61 | 0.55 | |
*Significant difference at 0.05 level
Figure 1: Showing comparison of stereognosis mean value between male and female participants
The normative value of stereognosis is not present in the existing data. There is dearth of study on stereognosis. Hence this study was done to find the normative value of stereognosis in adult population. Previous studies have been conducted on subjects with carpal tunnel syndrome, Hsu (2014) cerebral palsy, Dahlin (1988) comparison of oral versus manual stereognosis, such as of Fujii (2015) in stroke patients and of Uma Maheswari (2021) worked after hand surgery and stereognosis in older subjects.
This study was done on a population of 40 adults with age group of 20-40 years. Three trials were done with eyes closed and average of 3 trails was taken to obtain the normative value for stereognosis. The present study confirmed that there was significant difference between dominant and non-dominant side of hand performance of stereognosis. Mean values show that dominant hand i.e., right hand in mostly individuals has taken more time in recognising objects as compare to non-dominant hand i.e., left hand. This may be due to maturation effect as the test was first performed on dominant side than on non-dominant side.
Results show that there were no significant differences between male & female stereognosis mean values. Average reaction time to recognise objects in females was less as compare to males but it fails to reach statistically significance level. So, females have better stereognosis as compare to males. These results are consistent with a previous study by Dhanalakshmi et al. (2019) in which they found hand dexterity function was performed faster by females as compare to males.
CONCLUSION
Normative value of stereognosis is important to know for comparing it with any disease. Normative value of right hand is 3.04 sec. and of left hand is 2.09 sec. in age group of 20-40 years. Normative value of males & females in right hand are 3.11 sec. & 3.04 sec. respectively and in left hand are 2.08 sec. & 2.08 sec. respectively. These reference normative values can be used for the assessment of stereognosis and can also be used to compare with any disease so that treatment can be planned accordingly.
Future recommendations: The future study should include large sample size with equal numbers of male and female participants for better efficacy of result. Number of objects used for stereognosis should be more.
ACKNOWLEDGEMENTS: – Thanks to all the participants for their support to complete the study.
Conflict of Interest: – Authors declare no conflict of interests to disclose.
Funding: This research work did not have any particular funding.
REFERENCES
Abraira, V.E. and Ginty, D.D., 2013. The sensory neurons of touch. Neuron, 79(4), pp.618-639.
Carlson, M.G. and Brooks, C., 2009. The effect of altered hand position and motor skills on stereognosis. The Journal of hand surgery, 34(5), pp.896-899.
Dahlin, L.B., Komoto-Tufvesson, Y. and Sälgeback, S., 1998. Surgery of the spastic hand in cerebral palsy: improvement in stereognosis and hand function after surgery. Journal of Hand Surgery, 23(3), pp.334-339.
Fujii, R., Takahashi, T., Toyomura, A., Miyamoto, T., Ueno, T. and Yokoyama, A., 2011. Comparison of cerebral activation involved in oral and manual stereognosis. Journal of Clinical Neuroscience, 18(11), pp.1520-1523.
GoLDNER, J.L. and FERLIC, D.C., 1966. 10 Sensory Status of the Hand as Related to Reconstructive Surgery of the Upper Extremity in Cerebral Palsy. Clinical Orthopaedics and Related Research®, 46, pp.87-92.
Green, D.P., 1988. Operative hand surgery. In Operative hand surgery(pp. xxv-811).
Hsu, H.Y., Kuo, Y.L., Jou, I.M., Su, F.C., Chiu, H.Y. and Kuo, L.C., 2014. Diagnosis from functional perspectives: usefulness of a manual tactile test for predicting precision pinch performance and disease severity in subjects with carpal tunnel syndrome. Archives of physical medicine and rehabilitation, 95(4), pp.717-725.
Kilroy, E., Aziz-Zadeh, L. and Cermak, S., 2019. Ayres theories of autism and sensory integration revisited: What contemporary neuroscience has to say. Brain sciences, 9(3), p.68.
Kinnucan, E., Van Heest, A. and Tomhave, W., 2010. Correlation of motor function and stereognosis impairment in upper limb cerebral palsy. The Journal of hand surgery, 35(8), pp.1317-1322.
MR, D., Mangalvedhe, P.V. and Paul, J., NORMATIVE VALUES OF MOBERG PICKUP TEST IN YOUNG ADULTS.
Reitan, R.M. and Wolfson, D., 2002. Using the Tactile Form Recognition Test to differentiate persons with brain damage from control subjects. Archives of clinical neuropsychology, 17(2), pp.117-121.
Schermann, T. and Tadi P., 2021. Stereognosis. StatPearls Publishing.
Spillane, J., 2008. Bickerstaff’s neurological examination in clinical practice. John Wiley & Sons.
Thometz, J.G. and Tachdjian, M., 1988. Long-term follow-up of the flexor carpi ulnaris transfer in spastic hemiplegic children. Journal of Pediatric Orthopaedics, 8(4), pp.407-412.
Uma Maheswari, K., Gayatri Devi, R. and Jothi Priya, A., 2021. Estimation of Tactile Sensation by Two Point Discrimination among 18 Years Old People.
Van Heest, A.E., House, J. and Putnam, M., 1993. Sensibility deficiencies in the hands of children with spastic hemiplegia. The Journal of hand surgery, 18(2), pp.278-281.
Zancolli, E.A., Goldner, L.J. and Swanson, A.B., 1983. Surgery of the spastic hand in cerebral palsy: report of the committee on spastic hand evaluation. The Journal of hand surgery, 8(5), pp.766-772.

