Department of Orthodontics, Saveetha Dental College and Hospitals, Saveetha Institute of
Medical and Technical Science, Saveetha University, Chennai, India.
Corresponding author email: lichisolanki17@gmail.com
Article Publishing History
Received: 19/10/2020
Accepted After Revision: 07/12/2020
Headgears for class II correction in growing children require determination of centre of resistance of maxilla and maxillary dentition accurately. No standard accurate method is available in literature. The objective of this study was to formulate an indigenous simple method to locate the centre of resistance (Cres) of maxillary dentition extraorally (eocres) on the cheek and to determine whether the point marked extraorally coincides with the centre of resistance of the maxillary dentition (iocres) established previously between roots of premolars radiographically. 14 patients without gingival problems seeking Orthodontic treatment were included in this study. A divider tool was indigenously designed to mark a point extraorally on the cheek which coincided with the intraoral point between the roots of the two maxillary premolars, that is believed to be the Cres of the maxillary dentition. Radiopaque gutta percha was stabilized using adhesive transparent tape on the point marked extraorally and an Orthopantomogram was taken to evaluate the position of this point radiographically. The point was located between the roots of the maxillary first molar and second premolar at a mean height of 6.8+/- 0.52 and 6.8 +/- 0.48 respectively in the OPG. It can be concluded that by using a simple divider tool the extraoral Cres of the maxillary dentition can be marked conveniently and accurately. Thus, this novel simple method is a clinical innovation and can be used to determine the centre of resistance of the maxillary dentition extraorally for Class II patients requiring headgears, or bodily distilization intrusion of maxillary arch.
Centre Of Resistance; Distalization; Headgears; Maxillary Dentition
Solanki L. A, Dinesh S. Evaluation of the Accuracy of a Novel Method to Locate the Extraoral Point for the Centre of Resistance of Maxillary Dentition. Biosc.Biotech.Res.Comm. 2020;13(4).
Solanki L. A, Dinesh S. Evaluation of the Accuracy of a Novel Method to Locate the Extraoral Point for the Centre of Resistance of Maxillary Dentition. Biosc.Biotech.Res.Comm. 2020;13(4). Available from: <a href=”https://bit.ly/3p7dwls”>https://bit.ly/3p7dwls</a>
Copyright © Solanki and Dinesh This is an Open Access Article distributed under the Terms of the Creative Commons Attribution License (CC-BY) https://creativecommons.org/licenses/by/4.0/, which permits unrestricted use distribution and reproduction in any medium, provide the original author and source are credited.
INTRODUCTION
Overtime, numerous experimental methods have brought into light the concept that tooth movement is affected by various factors like magnitude, direction and the duration of the forces applied, direction of force playing the most pivotal part, ( Tanne and Sakuda 1991, Burstone 2015; Eliades et al. 2017). Hence, this urged the interest in biomechanics to study the overall effect of extra oral traction devices to the applied forces. The understanding of the relationship of the force vector to the centre of resistance (Cres) of the dentition became vital to appreciate the mechanical properties of the extraoral traction appliances. Centre of resistance is analogous to the centre of mass for restrained bodies i.e. tooth within the restrained boundaries of the periodontal ligament. In previous studies, Cres of a tooth or group of teeth or an entire dentition revealed that an important factor in tooth displacement is the point of application of force and the location of Cres of the maxillary complex and dentition offers integral information with respect to the usage of headgears, (Kragt and Duterloo 1983; Duterloo et al. 1985, Bulcke et al. 1987 Stocker et al 2020).
Extraoral traction forces applied via headgears have been used in many years to completely restrain or redirect the growth of maxilla in Class II malocclusions. (Stocker, Patcas, and Schätzle 2020) (Papageorgiou et al. 2017) .Headgears has numerous applications like anchorage control, distalization of molars (Sadeghi, Hedayati, and Mousavi-Fard 2019, Alosman, Bayome, and Vahdettin 2020), restrict maxillary growth, simultaneous distillation of premolars and molars, ( Biswas 2008) , complete distal displacement of the maxillary complex and maxillary dentition (Deguchi et al. 2008). Commonly encountered adverse effects due to ignorant biomechanics are extrusion and tipping of molar teeth (Rosa et al. 2020) which may cause the mandible to rotate posteriorly causing facial elongation and affecting the function and esthetics.
Force is delivered to the teeth by means of a face-bow attached to an intraoral bow which is placed into buccal tubes on the molar bands or by direct attachment of the arms of headgear on the maxillary arch wire itself by means of hook. The outer bow may be short of the Cres (flattens the occlusal plane) or long (steepens the occlusal plane) or passing through the Cres (no change in the cant of occlusal plane) of the maxillary complex and dentition and coincide with the position of the inner bow to produce a translatory distillation force devoid of any untoward movements (Greenspan 1970). Thus, it is essential to accurately determine the Cres of the maxillary complex and maxillary dentition.
No accurate and standard method has been established in literature to locate the Cres .Thus, the objective of this study was to formulate an indigenous simple method to locate the centre of resistance of maxillary dentition extraorally on the cheek and to determine whether the point marked extraorally on the cheek coincides with the centre of resistance of the maxillary dentition established previously between roots of premolars radiographically.
MATERIAL AND METHODS
This was a pilot study conducted on 14 patients in the age group of 14-40 years reporting to the Department of Orthodontics in a private hospital seeking treatment. The routine clinical examination and diagnosis was done for the patients. The methodology which was employed for this study was as follows: (Figure 1 and 2).The patients were seated on the dental chair and were asked to look straight at their eye levels.. The area near the roots of the 1st and 2nd maxillary premolars was isolated and a blue point was marked between them at distance of 10 mm from the Cementoename l junction i.e intraoral centre of resistance (iocres). This point was determined based on the known facts that the approximate root length of both premolars is 14 mm (Nelson and Ash, 2010) and the centre of resistance is generally 1/3rd to 1/4th the distance from the root apex (Bulcke et al., 1987).
Putty was placed on occlusal surfaces of the premolars and pushed apically upto the mark and the patient was asked to bite gently. The indigenous divider was then taken and the arm which was bent at right angles was passed through and through the putty prior to its set to make sure it coincided with the point marked between the two premolars. This arm was stabilized and the putty was allowed to set. Once the putty set (3.5 minutes; Zhermack Elite HD+ company), the soft tissues were relaxed and the other arm of the divider was closed and approximated extraorally on the cheek. This point was marked with blue marker and a small piece of the 6% gutta percha was cut and placed on the point and stabilized with transparent adhesive tape
.Orthopantomograms (OPG’s) were taken for each patient with the gutta percha point in place as routine diagnostic X-rays prior to treatment without exposing them to any additional radiation. Gutta percha was used specifically in an attempt to use a radiopaque material which would be distinguishable on the radiograph. Once the OPG’s were obtained, the point could be identified as a radiopaque point. The linear distances from the radiopaque point to the edges of roots of the premolars and molars, and the distance between the CEJ to the point was made and mean values were obtained by using FACAD software. (Figure 3).
Figure 1: Armamentarium : From left to right: An indigenous divider tool, marker, 6% gutta percha point, putty material.

Figure 2: Methodology to mark the centre of resistance

A) Point marked at 10mm distance from CEJ. B) Patient biting the putty placed on the occlusal surface, the marked point on gingiva is visible. C) The inner arm of the divider was placed on the exposed point. D) Once putty was set, the other arm of the divider closed on the cheek and a point was marked. E) Gutta percha stabilized with a transparent adhesive tape on the cheek on the point marked.
Figure 3: Measurements taken on the OPG
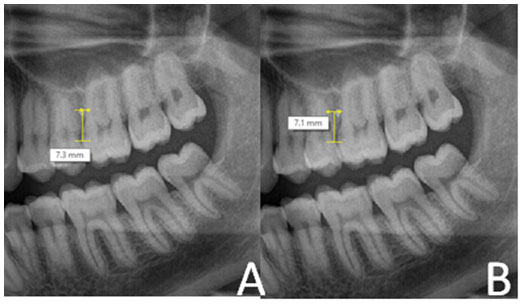
A) Distance from CEJ of the maxillary 1st molar. B) Distance from the CEJ of the maxillary 2nd premolar.
RESULTS AND DISCUSSION
The radiopaque point was located between the roots of the maxillary first molar and second premolar in the OPG of all the samples that were studied. (Figure 4). The means values of the distance of the radio opaque point (IOCres) to the maxillary 2nd premolar and 1st molar were calculated. The radio opaque point (IOCres) was located at a mean height of 6.8 mm from the CEJ of the 1st maxillary molar, 6.8 mm from the CEJ of the 2nd maxillary premolar (Table 1). This difference could be attributed to the angle of the radiation source to the radiopaque point on the cheek and the perpendicular distance between this point and the bone (thickness of the cheek).
Figure 4: represents the position of the radiopaque point between roots of the 2nd maxillary premolar and 1st maxillary molar.

Table 1. Mean values from CEJ of maxillary 1st premolar and molar to the IOCres , that is the radioopaque point on the OPG.
| DISTANCE FROM CEJ OF THE 2ND MAXILLARY PREMOLAR TO IOCres | DISTANCE FROM CEJ OF THE 1ST MAXILLARY MOLAR TO IOCres | |
| TOTAL NO OF PATIENTS | 7.50
7.40 6.80 6.40 7.30 6.00 6.10 6.80 7.10 7.50 6.40 6.10 6.80 6.90 |
6.80
7.40 7.30 6.50 7.40 6.90 7.10 6.20 7.50 7.00 6.10 6.50 6.40 6.30 |
| MEAN VALUE | 6.81 | 6.79 |
| STANDARD DEVIATION | 0.483 | 0.528 |
When force is applied to a tooth, tipping or bodily movement is expected to take place. It is mainly determined by the location of the Cres of the tooth and the distance from the force vector to this Cres. The knowledge of the accurate location of the Cres which is the point of the greatest resistance to tooth movement, helps in controlling the tooth movement by different moment to force ratios. Over the years, countless methods have been employed to determine the precise location of Cres of teeth, (Shroff et al., 1995). A force vector needs to pass the Cres of the maxillary dentition and through Cres of the maxilla to cause pure translation (Barton, 1972) and avoid any rotational effects(Roberts-Harry, 1996)(Teuscher, 1978). For a single tooth or a group of teeth, various experimental and analytical approaches have been researched by various authors. These studies reported the Cres of the single tooth to be half the root length as measured from the alveolar Crest, and an apical shift of Cres as more teeth were incorporated into the anterior segment, (Burstone and Pryputniewicz, 1980; Kusy and Tulloch, 1986; Tanne, Hiraga and Sakuda, 1989). However, it has been known that determining the position of Cres of the maxilla is tedious. Some cephalometric studies have attempted to determine Cres of maxilla by changes in craniofacial morphology (Bench, Gugino and Hilgers, 1978).
A Clinical method to determine the Cres of maxilla are given by Angle and Stanley Braun in 1999 was holding an amalgam plugger in maxillary vestibule when teeth were in occlusion and soft tissues relaxed. The amalgam plugger was palpated externally to determine the Cres of maxilla and marked on the cheek extraorally for the outer bow to pass through. Another clinical method known is to draw a line vertically 10 mm from the outer canthus of the eye and make a horizontal from that point to meet the pupil line in front of the face which denotes the Cres of the maxilla. But no clinical method has been known to mark the Cres of the maxillary dentition.
Tanne et al concluded that Cres of the nasomaxillary complex to be at the posterosuperior ridge of the pterygomaxillary fissure registered on a median plane by using a finite element analysis, (Tanne, Matsubara and Sakuda, 1995). Billet et al by using a holographic method on a human macerated skull showed that Cres of maxilla was underneath the zygomatic process but it couldn’t distinguish two different Cres i.e of the maxilla and maxillary dentition which are essential for application of accurate forces as suggested by Teuscher in 1986 and Stockli and Teuscher in 1994 (Billiet, 2001). Lee et al also conducted a similar study in a dry skull as Billet et al and concluded the Cres to be closer to the one as determined by Billet et al and couldn’t investigate the Cres of the Upper dentition (Lee et al., 1997). All the above literature has no study to determine the Cres of the maxillary dentition and all the above studies are sophisticated studies.
Thus the objective of this study was to establish a simple, easy, quick cost effective method to locate the Cres of the maxillary dentition extraorally which in turn helps swift maxillary Orthopaedic appliance therapy. Thus, this study was conducted in an attempt to determine whether the centre of resistance of the maxillary dentition established previously between roots of premolars coincides with the point marked extraorally on the cheek. The results revealed that the radiopaque point marked extraorally was reproduced constantly between the roots of the 1st maxillary molar and 2nd maxillary premolars. Miki in (1979) and Hirato in (1984) reported the location of Cres of the maxillary dentition is between the first and second premolars in the anteroposterior direction and between the lower orbital margin and the distal apex of the 1st molar vertically in the sagittal direction.(Zhang et al. 2016) This was distinguished by Teuscher in 1986, and Stockli and Teuscher in 1994 into Cres of the maxillary dentition to be situated between the roots of the two premolars and the Cres of the maxilla to be situated at the postero-superior area of the zygomaticomaxillary suture, (Teuscher 1986; Roberts-Harry 1996, Suzuki et al. 2019).
Our results are in contradiction to the results obtained by these authors. The reasons for this transposition can be explained by the fact that OPG is a two dimensional radiographic technique. While recording an OPG, the patient remains stationary but the x-ray source rotates in front of the patient from one side to the other side. The film rotates in the opposite direction to the x-ray source behind the patient, (Pandolfo and Mazziotti, 2013).Also while recording an OPG, the different angles of radiation causes magnification of posterior teeth and due to the negative angle of the ray tube in an OPG machine this magnification is known to be higher for maxillary teeth as compared to mandibular teeth (Yassaei, Ezoddini-Ardakani and Ostovar, 2010).
This magnification might cause some distortion. The x-ray source is directed at an angle to the Gutta percha point on the cheek and not directed perpendicularly, which caused the radiopaque point on the cheek (EOCres) to appear shifted distally on the OPG and not appear exactly on the IOCres in between the roots of the maxillary premolars. The distortion can also be attributed to the distance between the soft tissue cheek on which the point was marked and the bone. But this distortion was uniformly seen in all the study samples. The vertical measurements are more reliable in an OPG as compared to horizontal measurements as in the horizontal dimension, the functional focus is the rotation centre, whereas in the vertical dimension the focus is the X-ray source. Vertical measurements are reliable which still poses the point to be in between the molar and premolar (Thailavathy et al., 2017).
Thus, we can state that, if the mean values obtained are in this range and if the point is located between the maxillary 1st molar and 2nd premolar, the point has been accurately marked and is the Cres of the maxillary dentition. Thus, if the point is situated at any other position other than the one determined by this study, it could be due to some error while marking the point clinically. Cephalograms were not used in this study for confirming the position of the point keeping in mind the superimposition of structures making it less reliable for landmarks (Thailavathy et al., 2017), affecting clarity and accuracy.
CONCLUSION
Thus, this novel simple method is a clinical innovation and can be used to determine the centre of resistance of the maxillary dentition extraorally for Class II patients requiring headgears, or bodily distilization of maxillary arch or maxillary arch intrusion. This method could be used by orthodontists as a chair side method which is effective and less time consuming and simple. This was a pilot study and requires a study to be conducted with a larger sample size to confirm its results and its use in orthodontic practice.
Conflict of Interest: None.
REFERENCES
Alosman, Hala Sadek, Mohamed Bayome, and Levent Vahdettin. (2020). A 3D Finite Element Analysis of Maxillary Molar Distalization Using Unilateral Zygoma Gear and Asymmetric Headgear.Orthodontics & Craniofacial Research October. https://doi.org/10.1111/ocr.12430.
Barton, J. J. 1972. High-Pull Headgear versus Cervical Traction: A Cephalometric Comparison. American Journal of Orthodontics 62 (5): 517–29.
Bench, R. W., C. F. Gugino, and J. J. Hilgers. (1978). Bioprogressive Therapy. Part 6. Journal of Clinical Orthodontics: JCO 12 (2): 123–39.
Billiet, T. (2001). Location of the Centre of Resistance of the Upper Dentition and the Nasomaxillary Complex. An Experimental Study. The European Journal of Orthodontics. https://doi.org/10.1093/ejo/23.3.263.
Bulcke, Marc M. Vanden, Marc M. Vanden Bulcke, Charles J. Burstone, Rohit C. L. Sachdeva, and Luc R. Dermaut. (1987). Location of the Centers of Resistance for Anterior Teeth during Retraction Using the Laser Reflection Technique. American Journal of Orthodontics and Dentofacial Orthopedics. https://doi.org/10.1016/0889-5406(87)90390-8.
Burstone, Charles J. (2015). Physics and Clinical Orthodontics: 100 Years Ago and Today. American Journal of Orthodontics and Dentofacial Orthopedics. https://doi.org/10.1016/j.ajodo.2014.12.011.
Burstone, C. J and R. J. Pryputniewicz. (1980). Holographic Determination of Centers of Rotation Produced by Orthodontic Forces. American Journal of Orthodontics 77 (4): 396–409.
Deguchi, Toru, Takashi Murakami, Shingo Kuroda, Toshinori Yabuuchi, Hiroshi Kamioka, and Teruko Takano-Yamamoto. (2008). Comparison of the Intrusion Effects on the Maxillary Incisors between Implant Anchorage and J-Hook Headgear. American Journal of Orthodontics and Dentofacial Orthopedics: Official Publication of the American Association of Orthodontists, Its Constituent Societies, and the American Board of Orthodontics 133 (5): 654–60.
Duterloo, Herman S., Gerrit Kragt, and Annemiek M. Algra. (1985). Holographic and Cephalometric Study of the Relationship between Craniofacial Morphology and the Initial Reactions to High-Pull Headgear Traction. American Journal of Orthodontics. https://doi.org/10.1016/0002-9416(85)90128-9.
Eliades, T., T. G. Bradley, and W. Brantley. (2017). Material Properties and Effects on mechanotherapy∗∗Parts of This Chapter Appear by Permission of Elsevier in a Chapter Entitled Dental Materials Science and Orthodontics from the 6th Edition of Orthodontics: Current Principles and Techniques (Graber LW, Vanarsdall RL Jr, Vig KWL, Huang GJ, Editors), Elsevier, 2016. Orthodontic Applications of Biomaterials. https://doi.org/10.1016/b978-0-08-100383-1.00007-2.
Greenspan, Ronald A. (1970). Reference Charts for Controlled Extraoral Force Application to Maxillary Molars. American Journal of Orthodontics. https://doi.org/10.1016/0002-9416(70)90025-4.
Kragt, G., and H. S. Duterloo. (1983). The Initial Alterations in the Craniofacial Complex of Macaca Mulatta Skull Resulting from Forces with High-Pull Headgear. Journal of Dental Research. https://doi.org/10.1177/00220345830620031701.
Kusy, R. P., and J. F. Tulloch. (1986). Analysis of Moment/force Ratios in the Mechanics of Tooth Movement. American Journal of Orthodontics and Dentofacial Orthopedics: Official Publication of the American Association of Orthodontists, Its Constituent Societies, and the American Board of Orthodontics 90 (2): 127–31.
Lee, K. G., Y. K. Ryu, Y. C. Park and D. J. Rudolph. (1997). A Study of Holographic Interferometry on the Initial Reaction of Maxillofacial Complex during Protraction. American Journal of Orthodontics and Dentofacial Orthopedics: Official Publication of the American Association of Orthodontists, Its Constituent Societies, and the American Board of Orthodontics 111 (6): 623–32.
Namitha Ramesh PV, Namitha Ramesh P. V., and P. P. Biswas. 2008. Efficacy of High Pull Headgear in Restricting Maxillary Growth : A Clinical Study. Journal of Indian Orthodontic Society. https://doi.org/10.1177/0974909820080104.
Nelson, Stanley J and Major M. Ash. (2010). Wheeler’s Dental Anatomy, Physiology, and Occlusion. Saunders/Elsevier.
Pandolfo, Ignazio, and Silvio Mazziotti. (2013). Orthopantomography. https://doi.org/10.1007/978-88-470-5289-5.
Papageorgiou, Spyridon N., Eric Kutschera, Svenja Memmert, Lina Gölz, Andreas Jäger, Christoph Bourauel, and Theodore Eliades. (2017). Effectiveness of Early Orthopaedic Treatment with Headgear: A Systematic Review and Meta-Analysis. European Journal of Orthodontics. https://doi.org/10.1093/ejo/cjw041.
Roberts-Harry, D. (1996). Orthodontics: Current Principles and Techniques Thomas M. Gaber and Robert L. Vanarsdall Mosby Yearbook Inc., St. Louis, USA. Price: 132.00, ISBN: 0-8016-6590-6. The European Journal of Orthodontics. https://doi.org/10.1093/ejo/18.3.305.
Rosa, Anderson Jaña, Rizomar Ramos do Nascimento, José Nelson Mucha, and Oswaldo de Vasconcellos Vilella. (2020). Effects of the Cervical Headgear in Growing Angle Class II Malocclusion Patients: A Prospective Study. Dental Press Journal of Orthodontics. https://doi.org/10.1590/2177-6709.25.2.025-031.oar.
Sadeghi, Samaneh, Zohreh Hedayati, and Batoolalsadat Mousavi-Fard. (2019) Comparison of Two Asymmetric Headgear Force Systems: A Finite Element Analysis. Dental Press Journal of Orthodontics. https://doi.org/10.1590/2177-6709.24.2.41.e1-6.onl.
Shroff, Bhavna, Steven J. Lindauer, Charles J. Burstone, and Jeffrey B. Leiss. (1995). Segmented Approach to Simultaneous Intrusion and Space Closure: Biomechanics of the Three-Piece Base Arch Appliance. American Journal of Orthodontics and Dentofacial Orthopedics. https://doi.org/10.1016/s0889-5406(95)70128-1.
Stocker, Larissa Olivia, Raphael Patcas, and Marc Andreas Schätzle. (2020). Improving Headgear Wear: Why Force Level and Direction of Traction Matter. European Journal of Orthodontics 42 (2): 174–79.
Suzuki, Masayoshi, Kenji Sueishi, Hidenori Katada, and Satoshi Togo. (2019). Finite Element Analysis of Stress in Maxillary Dentition during En-Masse Retraction with Implant Anchorage. The Bulletin of Tokyo Dental College 60 (1): 39–52.
Tanne, Kazuo, Susumu Matsubara, and Mamoru Sakuda. (1995). Location of the Centre of Resistance for the Nasomaxillary Complex Studied in a Three-Dimensional Finite Element Model. British Journal of Orthodontics. https://doi.org/10.1179/bjo.22.3.227.
Tanne, K., J. Hiraga, and M. Sakuda. (1989). Effects of Directions of Maxillary Protraction Forces on Biomechanical Changes in Craniofacial Complex.”European Journal of Orthodontics 11 (4): 382–91.
Tanne, K., and M. Sakuda. (1991). Biomechanical and Clinical Changes of the Craniofacial Complex from Orthopedic Maxillary Protraction. The Angle Orthodontist 61 (2): 145–52.
Teuscher, U. (1986) An Appraisal of Growth and Reaction to Extraoral Anchorage. Simulation of Orthodontic-Orthopedic Results. American Journal of Orthodontics 89 (2): 113–21.
Teuscher, Ullrich. (1978). A Growth-Related Concept for Skeletal Class II Treatment. American Journal of Orthodontics. https://doi.org/10.1016/0002-9416(78)90202-6.
Thailavathy, V., Ssaravana Kumar, Daya Srinivasan, Divya Loganathan, and J. Yamini. (2017). Comparison of Orthopantomogram and Lateral Cephalogram for Mandibular Measurements. Journal of Pharmacy And Bioallied Sciences. https://doi.org/10.4103/jpbs.jpbs_98_17.
Yassaei, S.F. Ezoddini-Ardakani, and N. Ostovar. (2010). Predicting the Actual Length of Premolar Teeth on the Basis of Panoramic Radiology. Indian Journal of Dental Research. https://doi.org/10.4103/0970-9290.74207.
Zhang, Xiaobo, Hongmei Yao, Yanfei Yin, Li Tian, Peirong Li, Yuanqian Che, Menghan Wang, and Zhenlin Ge. (2016). Finite element analysis centre of resistance of maxillary dentition of different load mode in extraction space sliding closure. Biotechnology and Medical Science. https://doi.org/10.1142/9789813145870_0064.

