1Orthodontist, Ministry of Health, Riyadh, Kingdom of Saudi Arabia.
2Sigal Private Clinics, Riyadh, Kingdom of Saudi Arabia.
3Consultant Dermatologist, King Saud University, Riyadh, Kingdom of Saudi Arabia.
Corresponding author email: ryshehri1@gmail.com
Article Publishing History
Received: 08/06/2021
Accepted After Revision: 25/09/2021
The present study was under taken to evaluate the effects of filler injections on lip morphology changes in three dimensions (vertical, transverse, and sagittal). The subjects included 14 volunteers aged between 23 and 48 years who visited a private dermal clinic for lip enhancement with dermal filler injections. Photographs and video records were captured before (T1) and immediately after filler injection (T2) in frontal rest, frontal smiling, and lateral rest views. After one to two weeks, another set of records was taken before retouch injections (T3). These images were collected and measured using a software program to determine changes in lip morphology over time.
In upper and lower lip vermilion heights at rest, lower lip vermilion protrusion, and upper and lower lip indices, there were significant differences between T1 and T2, T2 and T3, and T1 and T3. In upper lip length at rest and while smiling, upper lip vermilion height while smiling, upper incisor displays at rest and while smiling, gingival display while smiling, interlabial gap, smile index, nasolabial angle, upper and lower lip protrusion to the E-line, and upper lip vermilion protrusion, there were significant differences between T1 and T2 and between T1 and T3.
There were no significant differences in intercommissural width and buccal corridors between any time points. Most static changes were gained at T3. Filler injection in the lips leads to an increase in lip length at rest and while smiling, lip vermilion height at rest and while smiling, smile and lip indices, lip protrusion to the E-line, and lip vermilion protrusion. Similarly, filler injection in the lips leads to a decrease in upper incisor display at rest and while smiling, gingival display while smiling, interlabial gap while smiling, and nasolabial angle, but it may not alter the intercommissural width (smile width) or buccal corridors.
Lip Morphology; Filler Injection; Cosmetic; Orthodontics
Alshehri R, Alsanea J, Al-Haddab M. Esthetics of Lip Morphology Changes After Filler Injections: A Clinical Assessment. Biosc.Biotech.Res.Comm. 2021;14(3).
Alshehri R, Alsanea J, Al-Haddab M. Esthetics of Lip Morphology Changes After Filler Injections: A Clinical Assessment. Biosc.Biotech.Res.Comm. 2021;14(3). Available from: <a href=”https://bit.ly/3o0Ynoe“>https://bit.ly/3o0Ynoe</a>
Copyright © This is an Open Access Article distributed under the Terms of the Creative Commons Attribution License (CC-BY). https://creativecommons.org/licenses/by/4.0/, which permits unrestricted use distribution and reproduction in any medium, provided the original author and sources are credited.
INTRODUCTION
The demand for cosmetic procedures has risen over the years. As a result, orthodontic procedures involved in facial esthetics have been increasingly sought after by clients. Amongst them, the most requested procedures include dentition alignment and reconciliation of the patient’s profile. Moreover, procedures that attempt to improve smiles are also frequently sought (Polo, 2008).Orthodontists evaluate patient profiles in frontal and vertical planes and in static and dynamic states. Orthodontists are required to critically analyze two main aspects in their patients.
The first factor to be considered is soft tissue repose and animation, which is focused around particular details such as the way lips would animate while smiling, the degree of gingival display, crown length, and the quality of the smile. The second factor to be considered is facial amendment over the years throughout a patient’s life or the impact of aging on the facial skeletal and soft tissue structures, (Sarver and Ackerman, 2003, Lafaille and Benedetto, de Maio, 2020. Lipko-Godlewska et al., 2021).
Lip shape and fullness strikingly impact facial esthetics. As one of the main determining factors of physical appearance, facial esthetics have been associated with allure, self-love, and overall self-confidence (de Aquino et al., 2013, Litner et al., 2008). Over the past five decades, fuller lips have been considered to be a desirable facial feature in women. A significant number of young females have undergone lip augmentation procedures to achieve the famous sought-after look portrayed by celebrities and fashion magazines (Segall and Ellis, 2007).
Moreover, according to a study done by Bisson and Grobbelaar (Bisson and Grobbelaar, 2004), it has been reported that models seem to be more inclined towards following the fuller lip trend than women who are not involved in the fashion industry. Lip augmentation with fillers accentuates the overall look by making the lips look fuller and more defined by enhancing lip contours, and by making them look smooth as the procedure also reduces the appearance of fine lines (Lanigan, 2011, Fitzgerald et al 2019).
Furthermore, the use of dermal fillers for facial rejuvenation is trending. Such cosmetic procedures promise fascinating esthetic outcomes such as youthful, younger, and wrinkle-free skin without the need for any invasive surgical procedure, (Vlahova et al., 2014b, Dalati et al 2020 De Maio, 2020, Lipko-Godlewska et al 2021).
This study was aimed to evaluate the consequences of filler injections on lip morphology changes in three dimensions (vertical, transverse, and sagittal). Our null hypothesis stated that there would be no distinction in lip measurements before and after filler injection at all time points within the frontal rest view, frontal smile view, or the lateral view.
MATERIAL AND METHODS
Sample selection: All subjects signed an institutional review board-approved informed consent form which was explained to them by doctors, and all photographs were taken by the same doctors. A total of 14 volunteers aged between 23 and 48 years came to a private dermal clinic in the city of Riyadh, Saudi Arabia, for lip enhancement with dermal filler injections. A total of 114 photographs (38 frontal rest views, 38 frontal smiling views, and 38 lateral views) were collected and measured for this study.
Inclusion and exclusion criteria: The inclusion criteria were as follows: voluntary involvement in the study, individuals of both sexes, between 18-50 years of age, and seeking dermal fillers in the lips for lip enhancement for esthetic reasons. However, patients with a cleft lip and/or palate; inability to determine the natural head position (i.e. uncooperative patients, patients with neural conditions); presence of any craniofacial anomalies or alternative pathology; history of significant facial trauma after a permanent or semi-permanent hyaluronic acid (HA) filler or Botulinum toxin (BTX-A) within the previous 12 months; infection, disorder, or scar in the lip or mouth area that would prevent adequate study assessments; orthodontic braces or any other orthodontic appliances; active prosthodontic treatment; history of weight reduction surgery were excluded from this study.
Data collection: Photographs were standardized using a Canon EOS 750D (Canon; Tokyo, Japan) digital camera with a resolution of 1080p and frame rate of 60 frames per second. The camera was mounted on an adjustable LED-ring-lighted tripod and placed in front of the subject. The camera was adjusted in front of the patient’s lower face at a distance of 55 cm and continuously registered the face with the lens positioned parallel to the true perpendicular of the face in the natural head position.
While the subject was in the natural head position, they wore eyeglasses with a clipped-on reference standard to enable calibration in a digital measurement program (Cooke and Orth, 1990).Three video recordings were made for each subject at each time point using the “P video” setting at 60 frames per second (frontal view of a subject at rest while talking, frontal view of a posed social smile, and lateral right side profile at rest). These videos were recorded pre-injection (T1), post-injection (T2), and at a follow-up one to two weeks later (T3) before retouching.
Filler injection type and technique: In this study, 0.8 mL of HA filler were injected using a 30-gauge needle 12 mm in length. Topical anesthesia was applied before filler injection. The dermatologist used the multiple linear retrograde threading technique. The amount of filler delivered was 0.5 mL to the upper lip and 0.3 mL to the lower lip. The injection points were 0.5 cm away from the corners of each lip.
Image analysis:Using software (OnyxCeph³™ 3.2.100 Build 233; Tigris Chemnitz, Germany), 114 digital photographs were analyzed for changes in all three dimensions. A total of 950 points were traced on the T1, T2, and T3 images.
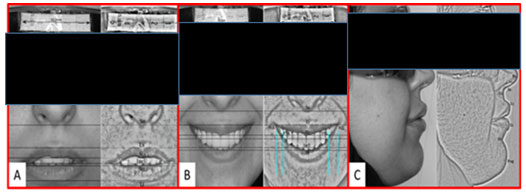
Measurements for the frontal view at rest (Figure 1A):Included upper lip length (Sn-Sts), upper lip vermilion height (Ls-Sts), upper incisor display (Sts-IncU), and lower lip vermilion height (Sti-Li).
Measurements for the frontal smiling view (Figure 1B):Vertical measurements included upper lip length (Sn-Sts), upper lip vermilion height (Ls-Sts), upper incisor display (Sts-IncU), gingival display (UIGM-Sts), and interlabial gap (ILG; Sts-Sti). Transverse measurements included intercommissural width (ICW; smile width; MCR-MCL), premolar width (PMR-PML), buccal corridors ((MCR to MCL) – (PMR to PML)), and smile index (ICW (MCR to MCL) / ILG (Sts to Sti)).
Measurements for the lateral right-side profile view (Figure 1C) included the nasolabial angle (angle between tangent Pn-Sn and tangent LS-Sn), the upper lip protrusion to the E-line of Ricketts (Ls to Pn-Pog’ line), lower lip protrusion to the E-line of Ricketts (Li to Pn-Pog’ line), upper lip vermilion protrusion (ULP; LS perpendicular to Sls-Ils line), lower lip vermilion protrusion (LLp; Li perpendicular to Sls-Ils line), upper lip index (ULH x ULP), and lower lip index (LLH x LLP).
Figure 1: Frontal view measurements (A) frontal view at rest, (B)
frontal smiling view and (C) lateral right-side profile view.
Examiner reliability: Reliability testing was carried out by having the examiner digitize the landmarks twice in a one-week interval for one randomly selected subject for each of the three different views. No significant differences were found between these examinations. The intra-class correlation coefficient was 1.00, which suggests 100% consistency across results.
Statistical analysis: The Statistical Package for Social Sciences (SPSS version 22.0; IBM, Armonk, NY) was used for statistical analysis. Sample size indicated a power value of 0.85, meaning that the chosen sample size allowed for statistical analysis. Friedman’s test was used to detect differences in measurements while the Wilcoxon signed-rank test with Bonferroni correction was applied to test differences between multiple time points for a specific measurement.
RESULTS AND DISCUSSION
Frontal rest measurements: Table 1 shows the lip changes after filler injection for the frontal rest measurements. 1. Upper lip length at rest :The upper lip length at rest was significantly increased between T1 and T2 by a mean value of 0.77 mm; between T2 and T3 also increased by a mean value of 0.39 mm (statistically insignificant). The net change between T1 and T3 was also statistically significant (1.17 mm).1, Upper lip vermilion height at rest.
The upper lip vermilion height at rest was increased between T1 and T2 by a mean value of 1.92 mm; between T2 and T3, decreased by a mean value of -0.12 mm. The net change between T1 and T3 was increased by 1.79 mm mean value.1 Upper incisor display at rest. The upper incisor display at rest was significantly decreased between T1 and T2 by a mean value of -0.84 mm; between T2 and T3 increased by a mean value of 0.04 mm (statistically insignificant).
The net change between T1 and T3 was significant and decreased by -0.8 mm mean value. 1 Lower lip vermilion height at rest.The lower lip vermilion height at rest was increased between T1 and T2 by a mean value of 1.2 mm; between T2 and T3 decreased by a mean value of -0.74 mm. The net change between T1 and T3 was increased by 0.45 mm mean value. The details are presented in Table 1.
Table 1. Lip changes after filler injection for the frontal rest measurements.
| Frontal at rest | T1 – T2 | T2 – T3 | T1 – T3 | |||
| Mean | P value | Mean | P value | Mean | P value | |
| upper lip length | 0.77857 | 0.001* | 0.39286 | 0.026 | 1.17143 | 0.005* |
| upper lip vermilion height | 1.92143 | 0.001* | -0.12857 | 0.011* | 1.79286 | 0.005* |
| Upper incisor show | -0.84286 | 0.001* | 0.04143 | 0.023 | -0.80143 | 0.005* |
| lower lip vermilion height | 1.20 | 0.001* | -0.74286 | 0.008* | 0.45714 | 0.005* |
* Statistical significance at p≤0.017
Frontal smiling measurements:
- Table 2 shows the lip changes after filler injection for the smiling measurements.1. Upper lip length: The upper lip length while smiling was significantly increased between T1 and T2 by a mean value of 1.04 mm; between T2 and T3 also increased by a mean value of 0.4 mm (statistically insignificant). The net change between T1 and T3 was significantly increased by 1.45 mm mean value.
- Upper lip vermilion height while smiling:The upper lip vermilion height while smiling was significantly increased between T1 and T2 by a mean value of 1.23 mm; between T2 and T3 also increased by a mean value of 0.49 mm (statistically insignificant). The net change between T1 and T3 was significant and increased by 1.73 mm mean value.
- Upper incisor display at a smile:The upper incisor display while smiling was statistically significant decreased between T1 and T2 by a mean value of -1.1 mm; between T2 and T3 increased by a mean value of 0.5 mm (statistically insignificant). The net change between T1 and T3 was also significant and decreased by -0.6 mm mean value.
- Gingival display while smiling :Gingival display while smiling was significantly decreased between T1 and T2 by a mean value of -0.78 mm; between T2 and T3 also decreased by a mean value of -0.12 mm (statistically insignificant). The net change between T1 and T3 was significant and decreased by -0.9 mm mean value.
- Interlabial gap while smiling: Interlabial gap while smiling was significantly decreased between T1 and T2 by a mean value of -1.6 mm. However, between T2 and T3 increased by a mean value of 0.49 mm (statistically insignificant). The net change between T1 and T3 was significant decreased by -1.11 mm mean value.
- Intercommissural width while smiling and Buccal corridors while smiling There was no statistically significant difference for the intercommissural width and buccal corridors at smile between T1 and T2; T1 and T3; and T2 and T3.
- Smile index:The smile index was significantly increased between T1 and T2 by a mean value of 1.97 mm. However, between T2 and T3 it was decreased by a mean value of -0.49 mm. (statistically insignificant). The net change between T1 and T3 was significant increased by 1.48 mm mean value. The details are presented in Table 2.
Table 2. Lip changes after filler injection for the smiling measurements
| Frontal smiling | T1 – T2 | T2 – T3 | T1 – T3 | |||
| Mean | P value | Mean | P value | Mean | P value | |
| Upper lip length | 1.04286 | 0.004* | 0.40714 | 0.646 | 1.45000 | 0.005* |
| Upper lip vermilion height | 1.23571 | 0.002* | 0.49429 | 0.645 | 1.73000 | 0.005* |
| Upper incisor show | -1.10714 | 0.005* | 0.50143 | 0.333 | -0.60571 | 0.011* |
| lower lip vermilion height | -0.78571 | 0.016* | -0.12143 | 0.838 | -0.90714 | 0.005* |
| Interlabial gap | -1.60714 | 0.001* | 0.49571 | 0.153 | -1.11143 | 0.005* |
| Intercommissural width | -0.65714 | 0.035 | 0.56857 | 0.314 | -0.08857 | 0.107 |
| Smile index | 1.97857 | 0.001* | -0.49571 | 0.202 | 1.48286 | 0.005* |
* Statistical significance at p≤0.017
Main lateral measurements: Table 3 presents lip changes after filler injection for the Lateral measurements.
- Nasolabial angle :The nasolabial angle was significantly decreased between T1 and T2 by a mean value of -5.87°; between T2 and T3 the angle increased by a mean value of 3.46° (statistically insignificant). The net change between T1 and T3 was statistically different by -2.4°.
- Upper lip protrusion to E-line:The upper lip protrusion to the E-line was significantly increased between T1 and T2 by a mean value of 1.32 mm; decreased between T2 and T3 by a mean value of -0.63 mm. The net change between T1 and T3 was statistically significant by 0.69 mm.
- Lower lip protrusion to E-line :The lower lip protrusion to the E-line was significantly increased between T1 and T2 by a mean value of 0.9 mm; decreased between T2 and T3 by a mean value of -0.54 mm. The net change between T1 and T3 was statistically significant 0.35 mm.
Table 3. Lip changes after filler injection for the Lateral measurements
| Lateral measurements | T1 – T2 | T2 – T3 | T1 – T3 | |||
| Mean | P value | Mean | P value | Mean | P value | |
| Nasolabial angle | -5.87143 | 0.001* | 3.46857 | 0.028 | -2.40286 | 0.005* |
| Upper lip protrusion to E-line | 1.32857 | 0.001* | -0.63857 | 0.052 | 0.69000 | 0.005* |
| Lower lip protrusion to E-line | 0.90714 | 0.001* | -0.54857 | 0.065 | 0.35857 | 0.005* |
* Statistical significance at p≤0.017
The present study was aimed to analyze the changes in lip morphology following lip filling injections. The changes were observed in the upper and lower lips of each individual in three dimensions including vertical, transverse, and sagittal planes. A total of 114 photographs were taken and evaluated for this study. The images were taken before and after the procedure.
The measurements show striking differences between images taken immediately after injection and those taken one to two weeks after the procedure. This suggests that the effect of lip fillers fades significantly over time; as a result of which, we considered a third measurement (T3) to determine the actual effect of HA fillers. One of the main reasons behind the changes noted over time following lip filling is the injection site reaction that follows immediately after HA filler injections.
According to Chiu et al, injection site reactions are fairly common after HA injections to the lip, despite being short-lived (Chiu et al., 2016). According to Lafaille and Benedetto, the most common side effects related to HA lip fillers are at the local injection site, including pain, redness, edema, ecchymosis, and itching (Lafaille and Benedetto, de Maio, 2020). However, these side effects are usually mild and short-lived , Abduljabbar and Basendwh, 2016, Lipko-Godlewska et al., 2021).
Upper lip length has a significant impact on the way lips equilibrate with one another. A shorter upper lip may decrease the lip seal and increase the interlabial gap at rest. Furthermore, the shorter the upper lip length, the greater the gingival exposure while smiling (Miron et al., 2012, Seixas et al., 2011).
Our study suggests that the upper lip can increase by roughly 1.2 mm, which is the length measured from the base of the nose (Sn) to the lowermost border of the upper lip (Sts) after lip filler injections. Subsequently, as a result, the visibility of the upper incisors decreased by only 0.8 mm.
Hence, it can be estimated that the reduction in incisor display is roughly around two-thirds of the amount of upper lip length gained. Furthermore, the remaining one-third could be due to a change in the Sn point position as a result of vermilion lip projection.
As per our observations, upper lip vermilion height grew by around 1.8 mm whereas the lower lip vermilion height increased by almost 0.45 mm. The difference between vermilion heights of the upper and lower lip can be attributed to different quantities of HA fillers injected.
The upper lip was injected with 0.5 mL of HA filler whereas the lower lip was injected with 0.3 mL. Concerning vertical smile measurements post-injection, the upper lip length and vermilion height increased by 1.45 mm and 1.73 mm, respectively. As a result, the upper incisor display and gingival display decreased by 0.6 mm and 0.9 mm, respectively. In contrast, BTX-A injections in subjects with large gingival displays (a “gummy smile”) resulted in gingival display reductions of 5.2 mm (Polo, 2008).
To evaluate the effect of dermal fillers on gingival display reduction, we required subjects with gummy smiles before filler injections. However, only 1 out of the total 14 subjects presented with a gummy smile before filler injection at T1, and they dropped out of the study after T2. Therefore, our findings of gingival display reduction relied on changes between T1 and T3 associated with the amount of upper lip length changes instead of actual gingival display changes.
The observations regarding the amount of reduction in gingival display achieved after lip filler injections are comparable to the report by Goldstein et al. (Goldstein et al., 2009). The use of dermal fillers for lip augmentation in cases with gummy smiles can be very helpful to improve the aesthetics of fixed prosthetic constructions for women with high or medium smile lines (Fitzgerald et al., 2019).
Vlahova et al. (2014a) showed pre- and post-procedure pictures that illustrated a decrease in smile line in two patients injected with HA fillers and they concluded that if a gummy smile is solely because of a thin upper lip, then lip-filling HA injections can give satisfactory results by improving the esthetics of a smile. Our suggested results are also in line with findings by Dalati, who stated that dermal fillers are used for lip augmentation and are used by dentists for cases of high lip lines, uneven lips, and to make the perioral area more esthetically pleasing (Dalati and Koussayer, 2020).
Even though all of the studies mentioned have results that can be compared to ours, they did not provide exact measurements. In contrast, our study showed that the mean gingival display reduction was almost 0.9 mm.The transverse dimension of the smile is a major characteristic of smile analysis.
The transverse dimension affects smile broadness and buccal corridors (more commonly referred by orthodontists as negative space) (Sarver, 2001).The effect of HA filler on intercommissural width and buccal corridors in our current study did not show a significant difference before and after injection. It can be suggested that the injection technique of terminating the filler injection 0.5 cm away from the corner of the mouth may contribute to these findings.
To visualize and quantify the frontal smile, Ackerman and Ackerman developed a ratio known as the smile index, which describes the area framed by the vermilion borders of the lips during a social smile (Ackerman and Ackerman, 2002). The smile index is determined by dividing the intercommissural width by the interlabial gap while smiling. This ratio helps compare smiles among different patients or over time in a single patient. It was suggested that the lower the smile index, the less youthful the smile appears.
Our results for the smile index increased after HA filler injection by almost 1.48 mm. As the intercommissural width did not change significantly in our study, it can be said that it did not affect the smile index, which was mainly affected by changes in the interlabial gap. As per our observations, the interlabial gap decreased by roughly 1.11 mm. Hence, it can be said that HA lip fillers can contribute negatively to the beauty of a smile due to a decrease in smile length, even if the smile index increases.
The nasolabial angle is influenced by the inclination of the columella of the nose and by the position of the upper lip. According to Sarver and Jacobson, one of the factors affecting the nasolabial angle is the soft tissue thickness of the maxillary lip, as a thin upper lip favors a flatter angle and a thicker lip favors an acute angle (Sarver and Jacobson, 2007). Our results showed that the nasolabial angle decreased after filler injection by almost 2.4°.
Therefore, the HA filler caused a narrowing of the nasolabial angle.The E-line, or the esthetic line of Ricketts, is drawn from the tip of the nose to the most anterior point on the soft tissue of the chin (Ricketts, 1957). This line is considered to be a very valuable diagnostic tool for an orthodontist to detect the amount of anterior-posterior soft tissue projection.
Our results showed that upper and lower lip protrusion to the E-line increased after filler injection by 0.69 mm and 0.35 mm, respectively.
Upper and lower lip vermilion protrusion were measured by perpendicular lines from the most anterior points of the vermilion of the lips to a line connecting the point of greatest concavity between the nose and upper lip and a point of greatest concavity between the chin and lower lip.22 Our results showed that the upper and lower lip vermilion protrusion increased after filler injection by almost 0.91 mm and 0.56 mm, respectively.
A simple lip index was proposed to evaluate the clinical effects and duration of dermal fillers (Lemperle et al., 2010). This index is calculated by multiplying the length of the vermilion lip by its protrusion. The upper and lower lip indices for our sample increased after filler injection by almost 15.94 mm2 and 8.31 mm2, respectively.
At the time of writing this manuscript, we could not find any study that measured the impact of dermal fillers on lips with such linear and angular measurements. Therefore, we could not objectively compare the results of this study with others.
In this study, we noticed differences in lip measurements before and after filler injection at all time points in the frontal rest view and the frontal smile view, and some differences in the lateral view, and so our null hypothesis was partially rejected.
CONCLUSION
Within the limitations of the present study, most static changes were gained at T3 (one to two weeks after filler injection), which we consider to be the actual effect of the HA filler. Injecting HA filler to the lips leads to an increase in the following parameters: lip length at rest and while smiling, lip vermilion height at rest and while smiling, smile index, lip protrusion to the E-line, lip vermilion protrusion, and lip index. Injecting HA filler to the lips also leads to a decrease in the following parameters: upper incisor display at rest and while smiling, gingival display while smiling, interlabial gap while smiling, and nasolabial angle. Injecting HA filler to the lips may not alter intercommissural width or buccal corridors.
Conflict of Interest: The author reports no conflicts of interest in this work.
Ethical Statement: The Board observed that you have complied with the Ethics Codes if the Scientific Research specified by the RCsDP has approved your proposal.The IRB approval number is RC/IRB/2016/586 which you may use as needed in future for conferences,poster presentation and publications. You are allowed to start your investigation starting 11-19-2017,please comply with the recommendations specified by the IRB.We wish you a successful project.
ACKNOWLEDGEMENTS
The authors are thankful to Alanoud Bin Muammar, Ghaida Alalshaykh and Lamyaa Altuwayjiri for providing assistance in clinical settings.
REFERENCES
Abduljabbar, M. H. & Basendwh, M. A. (2016). Complications Of Hyaluronic Acid Fillers And Their Managements. Journal Of Dermatology & Dermatologic Surgery, 20, 100-106.
Ackerman, M. B. & Ackerman, J. L. (2002). Smile Analysis And Design In The Digital Era. Journal Of Clinical Orthodontics, 36, 221-236.
Bisson, M. & Grobbelaar, A. (2004). The Esthetic Properties Of Lips: A Comparison Of Models And Nonmodels. The Angle Orthodontist, 74, 162-166.
Chiu, A., Fabi, S., Dayan, S. & Nogueira, A. (2016). Lip Injection Techniques Using Small-Particle Hyaluronic Acid Dermal Filler. Journal Of Drugs In Dermatology: Jdd, 15, 1076-1082.
Cooke, M. S. & Orth, D. (1990). Five-Year Reproducibility Of Natural Head Posture: A Longitudinal Study. American Journal Of Orthodontics And Dentofacial Orthopedics, 97, 489-494.
Dalati, M. H. N. & Koussayer, L. T. (2020). An Introduction To Botulinum Toxin And Dermal Fillers For Dentists: Part 1. Ec Dental Science, 19, 142-157.
De Aquino, M. S., Haddad, A. & Ferreira, L. M. (2013). Assessment Of Quality Of Life In Patients Who Underwent Minimally Invasive Cosmetic Procedures. Aesthetic Plastic Surgery, 37, 497-503.
De Maio, M. (2020) Myomodulation With Injectable Fillers: An Innovative Approach To Addressing Facial Muscle Movement. Aesthetic Plastic Surgery, 44, 1300-1316.
Fitzgerald, R., Carqueville, J. & Yang, P.( 2019.) An Approach To Structural Facial Rejuvenation With Fillers In Women. International Journal Of Women’s Dermatology, 5, 52-67.
Goldstein, R. E., Belinfante, L. & Nahai, F. (2009). Change Your Smile, Quintessence Pub.
Lafaille, P. & Benedetto, A. Fillers: Contraindications, Side Effects And Precautions. J Cutan Aesthet Surg. 2010; 3 (1): 16–19. Jcad.
Lanigan, S. (2011). An Observational Study Of A 24 Mg/Ml Hyaluronic Acid With Pre‐Incorporated Lidocaine For Lip Definition And Enhancement. Journal Of Cosmetic Dermatology, 10, 11-14.
Lemperle, G., Anderson, R. & Knapp, T. R.( 2010). An Index For Quantitative Assessment Of Lip Augmentation. Aesthetic Surgery Journal, 30, 301-310.
Lipko-Godlewska, S., Bolanča, Ž., Kalinová, L., Kermen, I., Onisak, B., Papp, I., Rebrov, M. & Valančienė, G. (2021). Whole-Face Approach With Hyaluronic Acid Fillers. Clinical, Cosmetic And Investigational Dermatology, 14, 169.
Litner, J. A., Rotenberg, B. W., Dennis, M. & Adamson, P. A. (2008). Impact Of Cosmetic Facial Surgery On Satisfaction With Appearance And Quality Of Life. Archives Of Facial Plastic Surgery, 10, 79-83.
Miron, H., Calderon, S. & Allon, D. (2012). Upper Lip Changes And Gingival Exposure On Smiling: Vertical Dimension Analysis. American Journal Of Orthodontics And Dentofacial Orthopedics, 141, 87-93
Polo, M.( 2008). Botulinum Toxin Type A (Botox) For The Neuromuscular Correction Of Excessive Gingival Display On Smiling (Gummy Smile). American Journal Of Orthodontics And Dentofacial Orthopedics, 133, 195-203.
Ricketts, R. M. (1957). Planning Treatment On The Basis Of The Facial Pattern And An Estimate Of Its Growth. The Angle Orthodontist, 27, 14-37.
Sarver, D. & Jacobson, R. S. (2007). The Aesthetic Dentofacial Analysis. Clinics In Plastic Surgery, 34, 369-394.
Sarver, D. M. (2001). The Importance Of Incisor Positioning In The Esthetic Smile: The Smile Arc. American Journal Of Orthodontics And Dentofacial Orthopedics, 120, 98-111.
Sarver, D. M. & Ackerman, M. B. (2003). Dynamic Smile Visualization And Quantification: Part 2. Smile Analysis And Treatment Strategies. American Journal Of Orthodontics And Dentofacial Orthopedics, 124, 116-127.
Segall, L. & Ellis, D. A. 2007. Therapeutic Options For Lip Augmentation. Facial Plastic Surgery Clinics Of North America, 15, 485-490.
Seixas, M. R., Costa-Pinto, R. A. & Araújo, T. M. D. (2011). Checklist Of Aesthetic Features To Consider In Diagnosing And Treating Excessive Gingival Display (Gummy Smile). Dental Press Journal Of Orthodontics, 16, 131-157.
Vlahova, Kazakova, Kissov, Popova & Todorov (2014a). Improving The Effect Of Aesthetic All-Ceramic Restorations With Hyaluronic Acid Fillers: Clinical Cases. J Interdiscipl Med Dent Sci Jbr Journal Of Interdisciplinary Medicine And Dental Science, 02.
Vlahova, A., Kazakova, R., Kissov, C., Popova, E. & Todorov, G. (2014b). Improving The Effect Of Aesthetic All-Ceramic Restorations With Hyaluronic Acid Fillers: Clinical Cases. J Interdiscipl Med Dent Sci 2: 134. Doi: 10.4172/2376-032x. 1000134 Page 2 Of 4 J Interdiscipl Med Dent Sci Issn: 2376-032x Jimds, An Open Access Journal Volume 2• Issue 4• 134. Figure, 4, 3.

