Department of Biotechnology, Adikavi Nannaya University, Rajahmundry
533 296, Andhra Pradesh, India.
Department of Microbiology, Rajiv Gandhi Institute of Management and
Science, Kakinada 533 005, Andhra Pradesh, India.
Corresponding author email:drdevaprakash@gmail.com
Article Publishing History
Received: 12/02/2025
Accepted After Revision: 24/03/2025
In the present study, an attempt has been made with regard to the bacteriological profile of the most commonly known infections found in the urinary tract. The 40 clinical samples were collected from patients of both sexes of all age groups. Out of 91 cases of the incidence of infections, there were 44% of the urinary tract infections. Gender wise incidence of UTIs in females is 59%, males is 42%, and UTIs in females is more than in males. The use of Amoxicillin has been recommended. The presence of detectable bacteria in the urine is named as the bacteriuria ecological zone of Amalapuram Mandal of Konaseema District of Andhra Pradesh.: Bacteriological study of urinary tract infection in Konaseema Institution of Medical Sciences and Research Foundation, Amalapuram revealed the route of various gram negative and gram-positive species of bacteria as the etiological agents.
Escherichia coli has been observed to be a predominant etiologic agent in cases of UTI closely followed by Klebsiella pneumonia. A large majority of cases occurred in the age group of 50 above years in males, (41-50) and 50 above years in females. The investigation reveals predominance of the disease in female patients (58%) than in male patients (42%). In vitro sensitivity tests reveal Gentamycin (75%) and Amoxycilin (100%), Nitrofurointoin (88%), Meropenum (74%) to be effective against the organisms causing urinary tract infections, followed by Cefoxitin (16%), CZA (16%) has been found to be the least. Escherichia coli was the most common pathogen incriminated in UTI, followed by Klebsiella pneumonia, and Staphylococcus species. In general, the emergence of the higher incidence of Gram-negative organism, especially Escherichia coli has occurred in this Konaseema region of Andhra Pradesh geographical area.
Bacteriological Profile, Urinary Tract Infections, Antibiotic Susceptibility Pattern,
Endogamous Populations, Konaseema Region, Andhra Pradesh.
Prakash D.S.R.S, Mohan S.M, Chandrakala B.P. Bacteriological Profile of Urinary Tract Infections and Antibiotic Susceptibility Pattern in Konaseema Region, Andhra Pradesh. Biosc.Biotech.Res.Comm. 2025;18(1).
rakash D.S.R.S, Mohan S.M, Chandrakala B.P. Bacteriological Profile of Urinary Tract Infections and Antibiotic Susceptibility Pattern in Konaseema Region, Andhra Pradesh. Biosc.Biotech.Res.Comm. 2024;18(1). Available from: <a href=”https://shorturl.at/R0jwA“>https://shorturl.at/R0jwA</a>
INTRODUCTION
Urinary tract infection is the second most common respiratory tract infection UTI is defined as an infection after disease caused by microbial invasion of the genitourinary tract, that extends from the renal cortex of the kidney to the urethral meatus. Urinary tract infections (UTIs) are counted among the most common infections in humans, exceeded in frequency among ambulatory patients only by respiratory and gastrointestinal infections. ( Shalini et al 2011, Levi et al 2005). The presence of detectable bacteria in the urine is known as bacteriuria. Presence of pus cells in urine denotes pyuria, which often accompanies UTI ( Hooton 2003, Baveja 2022 ).
The medical profession has known for a long time that urinary tract diseases of viral etiology. Infections of the urinary tract is commonly encountered in medical practice. The vast subject of urinary tract infection comprises many angles of study, namely bacteriological and clinical. The frequent occurrence of urinary tract infection among cases clinically diagnosed as “P U O “(Pyrexia of unknown origin) and the problem associated with their management are well appreciated. In trying to rid the urinary tract of the infection, the clinician is obliged to turn to bacteriology for it is the study of the nature of the invading bacteria that would lead to the proper treatment and Prevention of such infection ( Bhargava et al., 2022).
Acute urinary tract Infections are second only to respiratory tract infections in their frequency of occurrence. The problem of chronicity & recurrence of urinary tract infection is gaining paramount importance in recent years. Structural and congenital malformations and obstructive lesion are found to associate with urinary tract infections certain diseases such as diabetes mellitus and uremia are responsible for initiation or for their maintenance of urinary tract, urinary tract and catheterization infections instrumentation of are important predisposing factors for the development of urinary tract infections (Feinberg School of medicine, Chicago). A wide spectrum of gram positive & gram-negative organism have been incriminated as the ontological agents of urinary tract infections.
The extensive and inappropriate use of antimicrobial agents has invariably resulted in the development of antibiotic resistance, which, in recent years, has become a major problem worldwide (Goldstein FW, 2000). In patients with suspected UTI, antibiotic treatment is usually started empirically, before urine culture results are available. To ensure appropriate treatment, knowledge of the organisms that cause UTI and their antibiotic susceptibility is mandatory (Ashkenazi et al 1991). This study was planned to explore the common pathogens responsible for UTI and to determine the antibiotic susceptibility pattern of them.
MATERIAL AND METHODS
This was a cross-sectional analytical hospital-based study in which analysis of urinary culture results was done. This study was conducted in the department of Microbiology, Konaseema Institute of Medical Sciences & Research Foundation hospital in Amalapuram, Konaseema District, Andhra Pradesh, from March, 2024 to April, 2024. Both out and inpatients presenting or highly suspicious of having UTIs were recruited in the study. The details regarding the patient’s age, sex, literacy, socioeconomic status, and residential area (rural/urban) were recorded along with the sample. Both male and female patients having clinically suspected symptoms of UTI were included in the study.
Collection of Urine Samples: Early morning mid-stream urine samples were collected using
Sterile, wide mouthed container with screw cap tops. On the urine sample bottles were indicated name, age, sex, and time of collection along with requisition forms. The samples were analyzed bacteriological using the methods (Kass, 1957).
Sample processing:
Culture: A calibrated sterile micron wire loop for the semi-quantitative method was used for the plating and it has a 4.0 mm diameter designed to deliver 0.01 ml. A loopful of the well-mixed urine sample was inoculated into duplicate plates of Blood and Mac-Conkey agar. All plates were then incubated at 37ºC aerobically for 24 h. The plates were then examined macroscopically and microscopically for bacterial growth. The bacterial colonies were counted and multiplied by 100 to give an estimate of the number of bacteria present per millilitre of urine. A significant bacterial count was taken as any count equal to or in excess of 10,000 cfu /ml (National Committee for Clinical Lab Standards, 1993).
Antibiotic susceptibility test: Overall, 91 urine cultures were isolated from positive cultures and tested for their susceptibility to antibiotics. The anti- biogram was carried out by the disk diffusion method in Mueller Hinton agar medium according to the recommendations of the CLSI guidelines (Wayne PA, 2010). Several commercial antibiotic discs (Bio-Rad; Oxoid) used to treat UTIs were tested including: Amoxicillin. Azithromycin, Clindamycin, Cza, Cefoxitin, Doxycyclin, Gentamycin, Levofloxacin, Linezolid, Minocyclin, Norfloxacin, Nitrofurointoin and Vancomycin. Escherichia coli, Staphylococcus aureus, Pseudomonas aeruginosa, Klebsiella Pneumonia, Acinetobacter Baumanni and Proteus Mirabilis were used as quality control strains. The method used for standardization of the inoculums size was agar diffusion method. The standardized single-disc diffusion method was employed (Koneman’s Textbook, 2005). This study was ethically approved by institutional ethical committee of the institute.
RESULTS
In this study, urine sample total of 40 patients clinically diagnosed with urinary tract infection were collected and tested for microorganisms. There were 40 positive urine cultures (44%) and 51 (56%) negative. Escherichia coli represented 17 (42.5%.) of the positive urinary isolates. The resistance rate for Staphylococcus Species to CZA was found to be 83.83%.
Table 1. Incidence and Gender wise of Urinary Tract Infection
| Total No of Specimens Investigated | Culture Positive
|
Culture Negative | Gender wise | |||||
| Males | Females | |||||||
| 91 | Number | % | Number | % | Number | % | Number | % |
| 40 | 44% | 51 | 56% | 17 | 42% | 23 | 58% | |
The percentage incidence is more in females. The urinary tract infection in males and females is in the ratio 1:2
Table 2. Distribution of Uti Cultures and Types (Gram Positive and Gram Negative)
| GRAM POSITIVE | GRAM NEGATIVE | ||||
| ORGANISM | NUMBER | % | ORGANISM | NUMBER | % |
| STAPHYLOCOCCUS SPECIES | 07 | 17.5% | ESCHERICHIA COLI
KLEBSIELLA PNEUMONIA
PSEUDOMONAS AURUGINOSA
ACINETOBACTER BAUMANNI
PROTEUS MIRABILIS |
17
11
03
01
01 |
42.5%
27.5%
7.5%
2.5%
2.5% |
| 07 17.5% | 33. 82.5% | ||||
It is obvious from table that Escherichia coli is the most predominant organism encountered in this investigation with a percentage incidence of 42.5%. The incidence of gram-positive bacteria is 17.5% and gram-negative bacteria is 82.5%. The result revealed. The prevalence of gram negative as shown in Table 2.
Table 3.Organism In Relation to Gender and Age Groups
| ORGANISM | MALE GROUPS | FEMALE GROUPS | ||||||||||||
| 0-10 | 11-20 | 21-30 | 31-40 | 41-50 | ABOVE 50 | OVER ALL | 0-10 | 11-20 | 21-30 | 31-40 | 41-50 | ABOVE50 | OVER ALL | |
| STAPHYLOCOCCUS SPS
|
– | – | – | – | –
|
1
(5.88%) |
01 | – | 1
4.34% |
– | 1
4.34% |
2
8.69% |
2
8.69% |
06 |
| ESCHERICHIA COLI
|
1
5.88% |
– | – | – | – | 7
41.17% |
08 | 1
4.34% |
– | 2
8.69% |
2
8.69% |
1
4.34% |
3
13% |
09 |
| KLEBSIELLA PNEUMONIA | – | – | – | – | 1
5.88% |
3
17.64% |
04 | – | – | 1
4.34% |
– | 3
13% |
3
13% |
07 |
| PSEUDOMONAS AERUGINOSA
|
1
5.88% |
– | – | – | – | 1
5.88% |
02 | – | – | – | – | – | 1
4.34% |
01 |
| ACINETOBACTER BAUMANN | – | – | 1
5.88% |
– | – | – | 01
|
– | – | – | – | – | – | |
| PROTEUS MIRABILIS
|
– | – | 1
5.88% |
– | – | – | 01 | – | – | – | – | – | – | – |
| Table 4. Results of Sensitivity, Intermediate, Resistance of Drugs in Gram Positive Organism. | ||||
| Antibiotic | Organism | |||
| STAPHYLOCOCCUS SPECIES | ||||
| TOTAL | SENSITIVITY | INTERMEDIATE | RESISTANCE | |
| AMOXYCYCLINE | 07 | 7 (100%) | – | – |
| AZITHROMYCIN | 06 | 2 (33.33%) | – | 4 (66.66%) |
| CLINDAMYCIN | 07 | 5 (71.42%) | – | 2 (28.57%) |
| CZA | 06 | 1(16.66%) | – | 5 (83.83%) |
| CEFOXITIN | 06 | 1(16.66%) | – | 5(83.33%) |
| DOXYCYCLIN | 07 | 4 (57.14%) | 2 (28.57%) | 1(14.22%) |
| GENTAMYCIN | 07 | 6 (75%) | 1(13%) | – |
| LEVOFLOXACIN | 05 | 1(20%) | – | 4(80%) |
| LINEZOLID | 06 | 4 (66.66%) | – | 2 (33.33%) |
| MINOCYCLIN | 06 | 4 (66.66%) | – | 2 (33.33%) |
| NORFLOXACIN | 06 | 2 (33.33%) | 2 (33.33%) | 2 (33.33%) |
| NITROFUROINTOIN | 06 | 4 (16.16%) | – | 2 (33.33%) |
| VANCOMYCIN | 06 | 2 (33.33%) | – | 4 (66.66%) |
The overall antibiotic sensitivity pattern of urinary bacterial isolates. Staphylococcus Species was mostly sensitive to CZA (83.3%), CEFOXITIN (83.3 %), LEVOFLOXACIN in (80 %) followed by AMOXYCYCLINE (66.6 %), VANCOMYCIN (66.6 %).
Figure 1: Gram-positive Bacteria
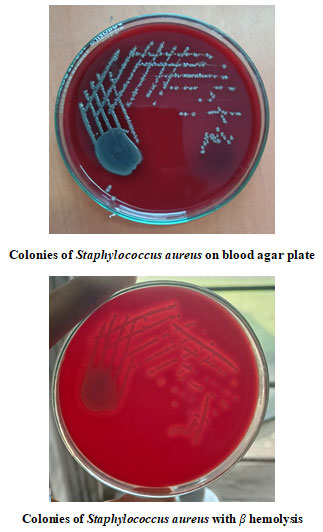
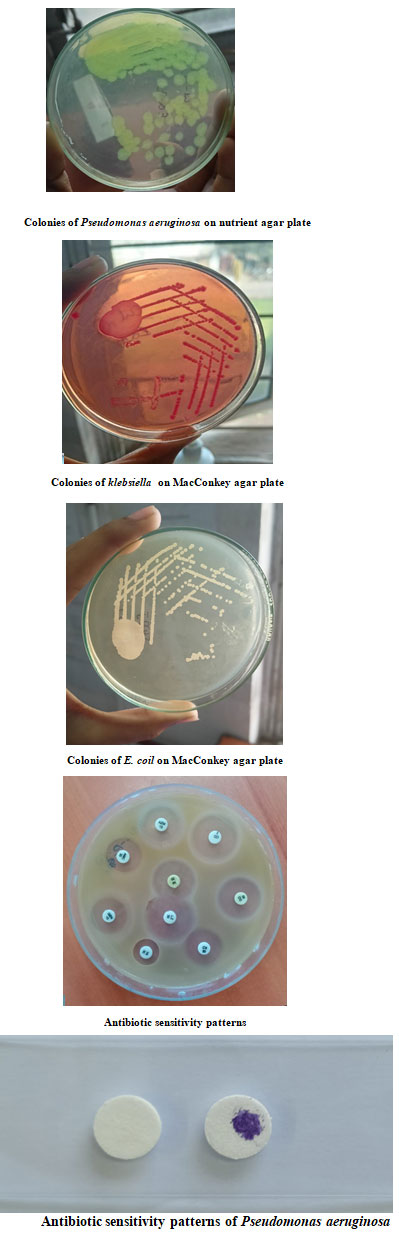
Figure 2: Gram Negative Bacteria
DISCUSSION
In community and hospital settings, the etiology of UTIs and the antimicrobial susceptibility of UTI causing bacteria’s have been changing over the years (New HC. 1996, Jones RN. 1996). A wide spectrum of gram-negative and gram-positive organisms has been incriminated for cases of UTI. In the present study of 91 cases, the incidence of infection was 44%. The prevalence nearly coincides with Panda et al (43.4%) (Panda et al, 2020). In a similar study by Das et al isolation rate was 71.6% (Das et al, 2006). The incidence of urinary tract infection in males 42% and females 58% is in the present study. Prevalence of UTIs was more in females when compared to males. This was in agreement with other studies by Bashir et al. (2008).
Women are more prone to UTIs then men because, in females, the urethra is much shorter and closer to the anus. ( Dielubanza and Schaeffer 2011, Gupta and Stamm 1990). The most commonly isolated organism in UTI among female outpatients in our study was E. coli. The proportion of bacterial species isolated was similar to those described in several previous studies. (Zhanel et al. 2005). Panda et al reported females 57%. and males 43%. The incidence of Escherichia coli isolated from UTI cases in the present study it is 42.5%.
The most commonly isolated organism in UTI among female outpatients in the present study was Escherichia coli. But nowadays Staphylococcus species, Klebsiella aerogenes, Pseudomonas aeruginosa, Proteus, Enterococcus, Acinetobacter and Candida have also been reported increasingly from UTI. The proportion of bacterial species isolated was similar to those described in several previous studies (Scottish Intercollegiate Guidelines Network. 2015) (Hertz et al 2016) (Akoachere 2012), These findings are consistent with those of Kader et al. The incidence of Escherichia coli isolated from UTI cases reported by Kader et al is 42.46%. (Kader et al. 2004 Panda et al 2024).
The incidence of Klebsiella aerogenes isolated from UTI cases in the present study is 27.5%, these findings are consistent with Latika et al reported the incidence of Klebsiella aerogenes is 13.5% (Latika J Shah et al, 2015). Shaki et al. (Shaki et al 2020) reported a predominance of E. coli and Klebsiella spp. in urine samples from Southern Israel. In Libya, Salem et al. (2018) indicated Klebsiella pneumoniae (43.6%) and E. coli (33%) as the two most isolated pathogens. The incidence of Staphylococcus species isolated from UTI cases in the present study is 17.5% with highest incidence in 51 and above year’s males, 41- 50 and females above 50 year’s. Sengupta et al reported 6.1% (Sengupta et al 2018), incidence was found to be equal in both sexes. Panda et al reported 7.2%, (Panda et al, 2020), the incidence in females is more in between the age group of 31-40. The incidence of Pseudomonas aeruginosa isolated from UTI cases in the present study is 7.5%, these findings are nearly coincides with Asifa Nazir et al 10.1 % (Asifa Nazir, Farhat Kanth, 2024).
The percentage of pseudomonas aeruginosa isolated from urinary tract from different parts of India is as follows: Bharati et al 5.7% (Bharti et al 2016). The incidence of proteus mirabilis reported in the present study is 2.5% nearly coincides with Asifa Nazir et al i.e., 1% (Nazir and Kanth, 2024) in males predominantly. Escherichia coli was the most common organism isolated (42.5%) among the gram negatives, followed by Klebsiella sp (27.5%), while other gram negatives isolated included Pseudomonas aeruginosa (7.5%), Proteus sp (2.5%).
In the present study, Most of the gram-positive organisms are sensitive to Amoxycyclin (100%), Gentamicin (75%), Clindamycin (71.42%), Doxycycline (57.14%), Nitrofurontoin (66.66%), Minocycline (66.66%), Linezolid (66.66%), Norfloxacin (33.33), Azithromycin (33.33%), Vancomycin (33.33%), Ceftazitdimeavivac (16.66%), Nitrofurontoin (66.66%), Cefoxitin (16.66%). And the Gram negative organism sensitive to Nitrofurointoin (88%), Meropenum (74%), Cefoperazone (53%), Norfloxacin (44%), Gentamycin (50%) Ceftazitdimeavivac (36%), Tetracycline (32%). gentamicin (92.3%) followed by imipenem (90.2%) and less sensitivity was shown to cefotaxime.
Das et al, (2015) in their study observed highest resistance to ampicillin, fluoroquinolones and ceftriaxone whereas gentamicin and nitrofurantoin were the antibiotics to which organisms were most sensitive. Most Escherichia coli from community infections investigated in this study were susceptible to oral drugs commonly used in general practice such as Amoxycyclin, Gentamicin, Clindamycin, nitrofurantoin, Minocycline and Norfloxacin.
CONCLUSION
Bacteriological study of urinary tract infection in Konaseema Institution of Medical Sciences and Research Foundation, Amalapuram revealed the route of various gram negative and gram-positive species of bacteria as the etiological agents. Escherichia coli has been observed to be a predominant etiologic agent in cases of UTI closely followed by Klebsiella pneumonia. A large majority of cases occurred in the age group of 50 above years in males, (41-50) and 50 above years in females. The investigation reveals predominance of the disease in female patients (58%) than in male patients (42%). In vitro sensitivity tests reveal Gentamycin (75%) and Amoxycilin (100%), Nitrofurointoin (88%), Meropenum (74%) to be effective against the organisms causing urinary tract infections, followed by Cefoxitin (16%), CZA (16%) has been found to be the least. Escherichia coli was the most common pathogen incriminated in UTI, followed by Klebsiella pneumonia, and Staphylococcus species. In general, the emergence of the higher incidence of Gram-negative organism, especially Escherichia coli has occurred in the Konaseema region of Andhra Pradesh geographical area.
Conflict of interest: Author declares no conflict of interest
Funding: Nil
Data Availability: Data will be available on request
Ethical statement: The study was a retrospective analysis of existing data and did not involve any direct patient contact or intervention. All patient data were anonymized and deidentified to protect patient confidentiality.
ACKNOWLEDGEMENTS
Authors express their sincere gratitude to Prof. S. Prasanna Sree, Vice Chancellor, Adikavi Nannaya University, Rajamahendravaram, East Godavari District, Andhra Pradesh, India for help and encouragement.
REFERENCES
Akoachere JF, Yvonne S, Akum NH, Seraphine EN. (2012). Etilogic profile and anti-microbial susceptibility of community acquired UTI in two Cameroonian towns. BMC Res Notes. 5; 219.
Ashkenazi S, EvenTov S, Samra Z, et al (1991). Uropathogens of various childhood populations and their antibiotic susceptibility. Paediatrics Infectious Diseases. Journal. 10: 742–6.
Bashir MF, Qazi JI, Ahmad Riaz S. (2008). Diversity of urinary tract pathogens and drug resistant isolates of Escherichia coli in different age and gender groups of Pakistanis. Tropical Journal of Pharmaceutical Research September; 7 (3):1025-1031
Baveja CP (2022). Textbook of Medical Microbiology, Arya Publishing Company.
Bharti AK, Farooq U, Singh S, Kaur N, Ahmed R, Singh K. (2016). Incidence of Enterococcal Urinary Tract Infection and its Sensitivity Pattern among Patients Attending Teerthanker Mahaveer Medical College and Research Centre, Moradabad, India. Int J Sci Stud;3 (12):115- 9
Das A and Banerjee T. (2015). Prevalence of Urinary Tract Infections and Susceptibility Pattern of Uropathogens in Women of Reproductive age Group from North India. J Adv Med;4 (1-2).
Das RN, Chandrashekhar TS, Joshi HS, Gurung M, Shrestha N, Shivananda PG. (2006). Frequency and susceptibility profile of pathogens causing urinary tract infections at a tertiary care hospital in western Nepal. Singapore Medical Journal; 47(4) : 281.
Dielubanza EJ, Schaeffer AJ (2011). Urinary tract infections in women. The Medical clinics of North America 95 (1): 27–41.
Goldstein FW (2000). Antibiotic susceptibility of bacterial strains isolated from patients with community acquired urinary tract infections in France. Multicentre Study Group. European Journal of Clinical Microbiology & Infectious Diseases. 19:112-7.
Gupta K, Stamm WE. (1990). Pathogenesis and management of recurrent urinary tract infections in women. World Journal of Urology.;17 (6)415-420
Hertz FB, Nielsen JB, Schønning K, Littauer P, Knudsen JD, Løbner-Olesen A, et al. (2016). Population structure of drug-susceptible, resistant and ESBL producing Escherichia coli from community-acquired urinary tract infections. BMC Microbiology. ; 16; 1-6.
Jones RN (1996). Impact of changing pathogens and antimicrobial susceptibility pattern in treatment of serious infections in hospitalized patients. American Journal of Medicine. 100 (Suppl.6A): S3-12.
Kader, Abdulrahman Abdulla; Kumar, A.; Dass, Selvarayan Mahimai. (2024). Antimicrobial Resistance Patterns of Gram-Negative Bacteria Isolated from Urine Cultures at a General Hospital. Saudi Journal of Kidney Diseases and Transplantation 15(2): 135-139.
Kass, E. H.(1957). Bacteriuria and diagnosis of infections of urinary tract. Archives of Internal Medicine, 100: 709-714.
Koneman’s Textbook (2005). Diagnostic Microbiology,6th Edition 2005.
Latika J Shah, Geeta M Vaghela, Hetvi Mahida (2015). Urinary Tract Infection: Bacteriological Profile And Its Antibiotic Susceptibility In Western India, National Journal Of Medical Research, (V,5) Issue.1.71-74.
Levi ME, Redington J, Barth L.( 2005). The Patient with Urinary Tract Infection. Manual of nephrology 6th Edition. Lippincott Williams & Wilkins.; 7: 91.
National Committee for Clinical Lab Standards (1993). Performance Standardization for antimicrobial Disc Susceptibility test. 4th ed. Villanona PA. CC, DC M2 AS.
Nazir A, Farhat Kanth (2024). Bacteriological Profile and Antimicrobial Susceptibility Pattern of Patients with Urinary Tract Infections In A Tertiary Care Hospital. Journal of Research in Applied and Basic Medical Sciences 10(2): 110-120
New HC. (1996). Urinary tract infections. American Journal of Medicine. 100 (Suppl.4A): S63-70.
Panda PK , Rakesh Kumar, Purnima Raj , Pragya Khusro et al (2020). Bacteriogical profile of antimicrobial susceptibility patterns of bacteria isolated from surgical site infections of patients attending a tertiary care Hospital. International journal of contemporary medical research. (V.7).Issue 2, B5-B9.
Salem MA, Ahmed FA.(2018). Bacterial profile of urinary tract infection and antimicrobial susceptibility pattern among patients attending at Bushra medical laborato- ry, Tripoli, Libya. J Gastroenterol Hepatol Res 2018; 7: 2671-2675
Scottish Intercollegiate Guidelines Network. (2015). Management of suspected bacterial urinary tract infection in adults- a national clinical guideline. Health improvement Scotland.
Sengupta, J. Rama.R. (2018). Phytochemical screening and antibacterial activities of Amaranthus viridis, Cynodon dactylon & Aerva sanguinolanta A preliminary investigation. Journal of the Indian Medical Association, (V.116), No 8, 116- 27.
Shaki D, Hodik G, Elamour S, Nassar R, Kristal E, Lei- bovitz R, et al. (2020). Urinary tract infections in children < 2 years of age hospitalized in a tertiary medical center in Southern Israel: epidemiologic, imaging, and microbiologic characteristics of first episode in life. European Journal of Clinical Microbiology & Infectious Diseases. 39: 955-963.
Shalini, Joshi MC, Rashid MK, Joshi HS. (2011). Study of Antibiotic Sensitivity Pattern in Urinary Tract Infection at A Tertiary Hospital. NJIRM Vol. 2(3): 43-46
Thomas M. Hooton. (2003). Fluoroquinolones and resistance in the treatment of uncomplicated urinary tract infection. International Journal of Antimicrobial Agents. (V.22) Supplement 2:65-72.
Wayne PA (2010). Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimi- crobial Susceptibility Testing. 20th ed Informational Supplement. CLSI document M100-S20. Clinical and Laboratory Standards Institute.
Zhanel GG Tamiko L Hisanaga, Nancy M Laing, Melanie R DeCorby, Kim A Nichol, Lorraine P Palatnik, Jack Johnson, Ayman Noreddin, Godfrey K M Harding, Lindsay E Nicolle, (2005). Antibiotic resistance in outpatient urinary isolates: results from the North American Urinary Tract Infection Collaborative Alliance (NAUTICA). International Journal of Antimicrobial Agents 26:380-388.

