Department of Medical Surgical Nursing, College of Nursing,
King Saud University, Riyadh, Saudi Arabia.
Corresponding author email: zhasan@ksu.edu.sa
Article Publishing History
Received: 11/09/2021
Accepted After Revision: 19/12/2021
The health effects of infectious diseases affecting school-aged children continue to be a source of concern in the majority of low- and middle-income nations, owing to poor personal hygiene habits and insufficient sanitary facilities in public primary schools. Schoolchildren and primary school pupils are at increased risk due to a lack of attention to a fundamental yet crucial aspect of personal hygiene, such as continually washing hands with soap under running water, and even due to a lack of information of correct hand washing with soap practice. In recent years, public health concerns about communicable diseases such as respiratory infection and pneumonia have increased. The majority of school students are more exposed to infectious risk factors as a result of their frequent engagement in unhealthy behaviors.
The purpose of this study is to determine the handwashing habits of Saudi Arabian secondary school students. The study employed a cross-sectional design in which an online survey was used to assess handwashing habits. Boys and girls from Saudi Arabia’s secondary schools were included in the population. Statistical software was used to synthesize and analyze the data collected. The findings indicate that there was a relatively high level of commitment to hand washing. Additionally, findings indicated that the primary reason for skipping hand washing was a lack of recall. When it comes to handwashing materials in schools, the majority of participants prefer water and soap.
The study discovered that the majority of secondary school students are unaware of the dangers associated with improper handwashing. Regression analysis revealed that there are significant predictors of handwashing commitment. Factors influencing secondary school students’ handwashing habits include their region, academic year, gender, age, and parent’s education. Thus, hygiene education programs in schools and communities should be implemented to raise awareness about the importance of hand hygiene.
Handwashing, Hygiene, Secondary School Students.
Noshili A. I, Hasan H. A. Z, Awaji N. Y. Assessment of Hand-Washing Habits Among Secondary School Students in Saudi Arabia. Biosc.Biotech.Res.Comm. 2021;14(4).
Noshili A.I, Hasan H.A.Z, Awaji N.Y. Assessment of Hand-Washing Habits Among Secondary School Students in Saudi Arabia. Biosc.Biotech.Res.Comm. 2021;14(4). Available from: <a href=”https://bit.ly/3lUffLP“>https://bit.ly/3lUffLP</a>
Copyright © Noshili et al., This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-BY) https://creativecommns.org/licenses/by/4.0/, which permits unrestricted use distribution and reproduction in any medium, provide the original author and source are credited.
INTRODUCTION
Due to poor personal hygiene practices and insufficient sanitary facilities in public primary schools, the health consequences of infectious diseases affecting school-aged children continue to be a source of concern in the majority of low- and middle-income countries. Due to a lack of attention to a fundamental but critical aspect of personal hygiene, such as constantly washing hands with soap under running water, and even due to a lack of knowledge about proper hand washing with soap practice, school children and primary school pupils are at a greater risk (Bolon 2011; Delea et al. 2020).
Inadequate awareness, practice, and attitudes toward personal hygiene, such as soap-washing, contribute significantly to the high prevalence of communicable diseases and can have long-term negative consequences for students as a whole (Bolon 2011; Delea et al. 2020). Many communicable diseases cause illness and death worldwide (Organization 2014). Infectious diseases are a major cause of morbidity and mortality among school-age children worldwide (Starke 2017).
Hand hygiene is a simple, effective, and inexpensive way to prevent the spread of infectious diseases (Cevizci et al. 2015). Schools are high-risk areas for infection because children work and play in close quarters. They may come across contaminated objects and surfaces. Infectious diseases can spread quickly in schools (Cutler 2010). Hand washing is the most cost-effective way to prevent infection spread from feces, body fluids, and inanimate objects (Besha et al. 2016; Ahmed et al. 2021).
Hand washing is especially important for children and adolescents, as unwashed hands can spread infections. Decreased absenteeism is another benefit of proper hand washing (Besha et al. 2016). Saudi students make up a significant portion of the total population, which was 31,742,308 in 2016, with 7277317 students. Only 1860116 (961888 males, 898228 females) are secondary school students (Cahyani 2017). Secondary students are regarded as an important cultural foundation due to their age, maturity, and knowledge. This section of society wants to be aware of and educated about hand-washing practices to improve their lives, families, and communities (Ahmed et al. 2021).
Overcrowding in a classroom increases the risk of infection and other health issues. Furthermore, the number of students in a classroom can affect the environment, resulting in poor ventilation and disease spread. The OECD estimated the normal range for students per class not to exceed 21.4 in public schools and 20.5 in public-private schools (Indicators 2009). However, in one region, Jizan city, the number of students per class exceeded the OECD recommendation by 24.6 at the intermediate level and 40.9 at the secondary level (JEC Report 2017; Ahmed et al. 2021).
As such, the purpose of this study was to ascertain the hand washing habits of secondary school students in Saudi Arabia. The specific objectives are as follows: (1) to ascertain the most frequently used substances for hand washing by secondary school students in the preceding month; (2) to ascertain the most frequently cited reasons for skipping handwashing in schools among secondary school students; and (3) to ascertain demographic variables as predictors of secondary school students’ handwashing habits (Ahmed et al. 2021).
MATERIAL AND METHODS
This study was employed as a descriptive correlational research design to examine secondary school students’ handwashing habits and the factors that influence them. We have looked for significant associations between the independent and dependent variables. This study was conducted at the secondary school level. The schools, which are either exclusively for boys or girls, are located throughout Saudi Arabia. By the end of the first half of this year, the Kingdom of Saudi Arabia will have a total population of 34.22 million people (Ahmed et al. 2021).
Participants were chosen based on inclusion criteria. The schools of the participants should be recognized as state-owned and located in Saudi Arabia. As secondary school students, they are between the ages of 15 and 18 and enrolled in schools for the 2019–2020 academic year. The primary and elementary schools were excluded. The total sample size required for the study was calculated using the 2018/2019 records at a 95% confidence level, a 5% margin of error, and a population size of 1,057,205 (Cahyani 2017). Using Rao soft software to calculate the sample size, the total sample size required for this study is 386 subjects with a response distribution of 25%.
However, 699 students were surveyed to ensure that the sample was representative and to reduce margin error. With this sample size, the level of confidence increased to 95% and the margin of error was 3.71% (Ahmed et al. 2021). Due to the current COVID-19 pandemic situation, data collection was conducted online. Restrictions on visiting schools were implemented, and the use of paper surveys is likely to contribute to the spread of infection. The researchers created an account on an online survey platform (such as surveysparrow.com) and then converted the tools to an online format. The first step was to validate the tool on a subset of students prior to conducting the final data collection via pilot study.
Changes were made to the questionnaire in response to the students’ responses and reactions. The time required for students to complete all sections of the survey was estimated to be between 3-5 minutes. Permission was obtained from the responsible authorities at the Faculty of Nursing College of King Saud University and the responsible persons at the Ministry of Education to conduct the study online. Prior to data collection, each school’s principal was consulted. The questionnaire included nine questions and was divided into three sections. The first section contained six questions requesting demographic information. This section included information about the participant’s gender, age, education level, place of residence, and parents’ educational level.
The second section contained two questions in which respondents were asked about the handwashing substances they used in the previous month and their personal reasons for not washing their hands. The third section contained a single question in which students were asked about their handwashing habits or frequency of handwashing in various situations. These components were quantified using a five-item Likert scale based on their frequency of occurrence: never, rarely, occasionally, mostly, and always. The instrument was adapted from previous research ( Pati et al. 2014; Adriaenssens et al. 2015). The author revised the content and validity as necessary, particularly to ensure easier comprehension in Arabic. Additionally, a pilot study with 62 students from various grades was conducted three days prior to the final data collection time to evaluate the reliability.
Permission to use this tool was obtained from the author, who generously granted it. The tool was originally written in English and then translated into Arabic. The tool was translated from English into Arabic because the respondents in this study spoke Arabic as their first language, and then it was translated back from Arabic to English to ensure conformity with the original.
To determine the content validity of each question, a panel of three expert professional staff members from a nursing college was selected. Each reviewer used a separate form provided for this purpose to record both criticism and suggestions for improvement. As a result, each reviewer provided both feedback and suggestions for improvement. Others were omitted and some were replaced based on the experts’ objective analysis of the items, primarily due to their clarity and consistency, particularly on items 3 and 2 (Waltz et al. 2010).
The major changes include response coding and question formulation to avoid leading questions and complex sentences, which had no effect on the questionnaire’s reliability. The content validity test was used to determine whether the Arabic version appears to be relevant to the study’s objective and the concept of handwashing among school students. The Arabic version received an overall rating of 0.83 from the judges, indicating that the content is valid (Waltz et al. 2010). A pilot test was conducted to assess reliability using ten students randomly selected from two schools that were not included in the main study subjects.
The primary objective of the pilot study was to assess the questionnaire’s internal consistency in light of the tool’s intended use among Saudi Arabian school children. The data from the pilot study were analyzed using SPSS version 22. The total average for all questions was calculated and added to the statistical analysis; the results indicated a Cronbach’s alpha of 0.71. This score indicates that the tool is suitable for use by secondary school students in Saudi Arabia. Due to pandemic restrictions, this study followed an online survey.
As a result, most young people in Saudi Arabia have access to it via WhatsApp, Snapchat, and Twitter. Second, because all schools were closed due to precautionary measures to control and limit the spread of COVID-19, most students were at home. They broadcasted at lunchtime and at night, when most people are at home. It was done to reduce sampling bias in the analysis.
As before, participants were not offered incentives, tokens, or payments as a way to eliminate false or hurried answers from those who answered study questions only for the token. Eventually, surveysparrow.com’s website included numerous steps to discourage repeat participation by one person. The IBM SPSS version 22 statistical package was used to synthesize and evaluate the data (IBM Corp., 2015). Outliers and missing data were identified using double data entry, testing of the frequencies and ranges in the descriptive statistics, and testing of the confidence intervals in the descriptive statistics.
In addition to descriptive statistics like mean and standard deviation, frequencies, minimum and maximum scores, and minimum and maximum scores were computed. Calculated for both the first and second study topics were descriptive statistics such as the mean (average), standard deviation (standard deviation), frequencies (frequency distribution), and the minimum and maximum scores. For the third research question, the mean and the sum of the scores for each item were determined for each question.
In order to answer the fourth research question, the independent variable (demographic data) was assessed at the nominal level, while the dependent variable (hand washing behaviors) was examined at the ordinal and interquartile range (Likert scale). Multiple Linear Regressions, or ML, were carried out with the overall score of the hand washing commitments as the dependent variables, with the significance threshold set at 0.05 (Khan et al. 2019). The independent factors were age groups, gender, school year level, parents’ education, and region of residence. The dependent variables were age groups, gender, and school year level.
RESULTS AND DISCUSSION
Six hundred and ninety-nine respondents were selected from the target population. Demographic variables collected from respondents include gender, age, parents’ education, region of residence, and school year level. In terms of gender, it was clear that males participated at a higher rate than females in this study. In terms of age groups and school years, the results indicate that the third year of secondary school is the most frequently represented, with students over the age of 16. However, the results of the parents’ education indicate that the majority of participants’ parents held bachelor’s degrees. The majority of students resided in the Janzen region.
Table 1. Demographics Characteristics of Subjects
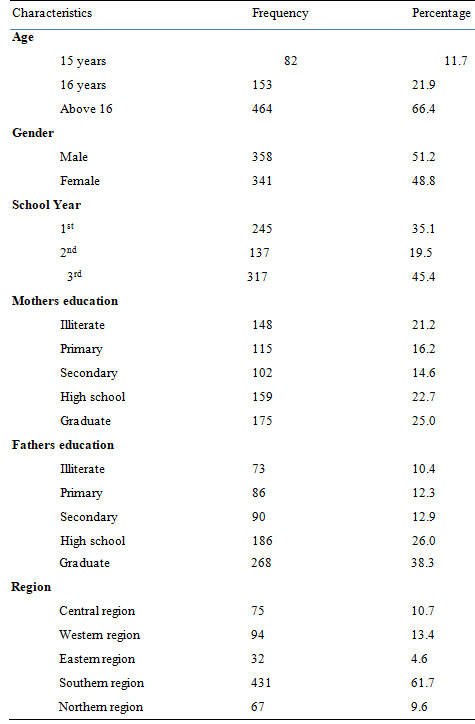
Table 1 contains detailed information. Students were given options for handwashing materials such as soap, water, disinfectant, and others. The majority of students chose water and soap. Additionally, the study’s findings indicated that the majority of participants forget to wash their hands. Others stated that they lack the time or opportunity to wash their hands and that the hand washing facilities were not clean (see Table 2).
Table 2. Reasons for not handwashing and common materials used
| Variables | Categories | Frequency | % | Mean (SD) |
| Material used to wash the hand in last previous months | Water | 112 | 16.0 | 3.78
(SD= 1.93) |
| Water and Soap | 401 | 57.4 | ||
| Disinfectant | 9 | 1.3 | ||
| Others | 11 | 1.6 | ||
| All | 166 | 23.7 | ||
|
Reasons for not washing the hands |
no time |
135 |
19.3 |
2.81 (SD= 1.29) |
| no need | 113 | 16.2 | ||
| Forgetting | 308 | 44.1 | ||
| Hand-washing facilities are not easily accessible | 38 | 5.4 | ||
| Hand-washing facilities are not clean | 105 | 15.0 |
Students consistently selected “wash your hands before eating,” “after eating,” “after touching an animal,” “after waking up in the morning,” “when my hands are dirty,” “before preparing meals,” “after touching the garbage,” “after combing my hair,” and “after playing.” Meanwhile, responses to the remaining ten statements were relatively consistent; respondents chose mostly, occasionally, or rarely. However, respondents almost always selected never for the statements “when I return from school”, “after exchanging money”, “after sneezing”, and “after picking up anything from the ground”, indicating that secondary school students are unaware of the dangers of not washing their hands (See Table 3).
Table 3 A. Reasons to Wash and Not Wash the Hands Response to Each Statement
of the Questionnaire” When You Wash Your Hands”,
| Variables | Never | Rarely | Sometimes | Mostly | Always | µ (SD) |
| Wash the hands before you eat | 93
(SD13.3) |
12
(SD1.7) |
42
(SD6.0) |
126
(SD18) |
426
(SD60.9) |
4.12
(1.387) |
| After eating | 30
(SD4.3) |
15
(SD2.1) |
14
(SD2.0) |
55
(SD7.9) |
565 (SD83.7) | 4.65
(.956) |
| Wash your hands before going to the toilet | 170
(SD24.3) |
100
(SD14.3) |
166
(SD23.7) |
117
(SD16.7) |
146
(SD2 0.9) |
2.96
(1.456) |
| Wash your hands after going to the toilet | 79
(SD22.3) |
11
(SD2.6) |
26
(SD3.7) |
103
(SD14.7 |
480
(SD68.7) |
4.28
(1.315) |
| When I come back from school | 184
(SD26.3) |
64
(SD9.2) |
99
(SD14.2) |
110
(SD15.7) |
242
(SD34.6) |
3.23
(1.624) |
| After shaking hands with people | 128
(SD18.3) |
180
(25.3) |
215
(SD30.8) |
96
(SD13.7) |
80
(SD11.4) |
2.74
(1.233) |
| After touching an animal | 73
(SD10.4) |
22
(SD3.1) |
39
(SD5.6) |
107
(SD15.4) |
458
(SD65.5) |
4.22 (1.315) |
| After waking up in the morning when my hands are dirty | 57
(SD8.2) |
24
(SD3.2) |
39
(SD5.6) |
104
(SD14.9) |
475
(SD68) |
4.31 (1.230) |
Table 3 B. Reasons to Wash and Not Wash the Hands Response to Each Statement
of the Questionnaire” When You Wash Your Hands”,
| Variables | Never | Rarely | Sometimes | Mostly | Always | µ (SD) |
| Before preparing meals | 82 (SD11.7) | 14(SD2.0) | 34(SD4.9) | 111(SD15.9) | 458(SD65.5) | 4.21 (1.340) |
| After exchange money | 133(SD19) | 216 (SD30.9) | 158(SD22.6) | 99(SD14.2) | 93(SD13.3) | 2.72 (1.291) |
| After cleaning my ear | 147(SD21) | 60(SD8.6) | 97(SD13.9) | 131(SD18.7) | 264(SD37.8) | 44 (1.561) |
| After cleaning my nose | 121(SD17.3) | 42(SD6) | 73(10.4) | 117(SD16.7) | 346(SD49.5) | 3.75 (1.529) |
| After sneezing | 175(SD25) | 58(SD8.3) | 99(SD14.2) | 162(SD23.2) | 205(SD29.3) | 3.23)1.561( |
| After rubbing my eyes | 167(SD23.9) | 142(SD20.3) | 156(SD22.3) | 107(SD15.3) | 127(SD18.2) | 2.84 )1.412) |
| After touching the garbage | 40(SD5.7) | 16(SD2.3) | 23(SD3.3) | 100(SD14.3) | 520(SD74,4) | 4.49(1.068) |
| After combing my hair | 40(SD5.7) | 16(SD2.3) | 23(SD3.3) | 100(SD14.3) | 520(SD74,4) | 2.91(1.450) |
Twenty statements were included in this study, ranging from always (5) to never (1) on a 5-likert scale. The maximum possible score is 100, and the minimum possible score is 20. The response’s mean score is 72.8 (SD 12.7). The minimum score was 36, and the maximum score was 100. However, the level of commitment is greater than 70, which is considered to be quite high. Additionally, the results indicate that the majority of respondents always, mostly, or occasionally agree with statements evaluating their commitments to hand washing. Further details about the study group’s response to specific situations involving hand washing are provided in the following sections. For example, Table 4 revealed that less than half (49.5 %) of respondents washed their hands after cleaning their nose and less than three-quarters (37.8 %) of respondents washed their hands after cleaning their ear.
Table 4. Study group according to hand-washing habits after cleaning ear, nose and rubbing eye)
| Variables | Never | Rarely | Sometimes | Mostly | Always | µ (SD) |
| After cleaning my ear | 147 (21%) | 60(8.6%) | 97(13.9%) | 131(18.7%) | 264(37.8%) | 3.44(1.56) |
| After cleaning my nose | 121(17.3%) | 42(6%) | 73(10.4%) | 117(16.7%) | 346(49.5%) | 3.75(1.1%) |
| After rubbing my eyes | 167(23.9%) | 142(20.3%) | 156(22.3%) | 107(15.3%) | 127(18.2%) | 2.84 (1.41%) |
Additionally, Table 5 revealed that over two-thirds (74.4%) of students always washed their hands after combing their hair.
Table 5. Study population hand-washing habits after combing the hair. n=699
| Items | Frequency | Percentage | µ (SD) |
| Never | 40 | 5.7% |
2.91(1.450) |
| Rarely | 16 | 2.3% | |
| Sometimes | 23 | 3.3% | |
| Mostly | 100 | 14.3% | |
| Always | 520 | 74.4% |
There is overwhelming evidence demonstrating the critical role of handwashing in disease prevention, particularly among vulnerable groups such as students. To this end, a variety of stakeholders contribute to the improvement of adolescents’ handwashing commitment. Handwashing is well-documented as a cost-effective method of reducing disease spread. Handwashing with running water and no soap is a better preventative measure than not washing at all (Luby et al. 2011; Mahmud et al. 2015).
For children, the practice is even more critical, as the demography is more susceptible to inhibiting infections and factors affecting personal hygiene. The findings in this study reflect a hot and cold state of affairs in adolescence’s commitment to handwashing. The circumstances are the result of a number of factors, as demonstrated by the investigation’s findings (Mahmud et al. 2015; Pogrebna and Kharlamov 2020).
Additionally, there is widespread recognition of the importance of handwashing and its practice among the study population. Adolescents are generally aware of the importance of proper handwashing. It’s unsurprising that approximately 50% of participants adhere to acceptable handwashing practices (Wilkinson et al. 2012). There is a high level of commitment to handwashing prior to eating, and more than 60% of respondents wash their hands after these activities. Surprisingly, students routinely washed their hands after sneezing or cleaning their noses. The phenomenon exemplifies the student’s awareness of the critical nature of handwashing.
Based on a previously published report a high rate of Middle East respiratory syndrome coronavirus (MERS-CoV) transmission via sneezing or nose cleaning. As such, handwashing after sneezing or washing one’s nose is critical for preventing the spread of MERS-CoV. Regrettably, a sizable portion of the population has a low commitment to handwashing. Nevertheless, the importance of consistent and continuous education cannot be overstated (Bolds et al. 2019). Besha et al. studies explain that adolescence’s low commitment to handwashing is a result of a number of factors that inhibit or disinterest the group in developing acceptable handwashing practices (Besha et al. 2016; Al-Hazmi et al. 2018; Pogrebna and Kharlamov 2020).
Additionally, this study discovered that students always wash their hands before eating, visiting the restroom, touching animals, or sneezing. Additionally, the results indicated a high level of commitment to hand washing among secondary school students. These findings suggest that in the Saudi Arabian student population, handwashing behavior improves with age and increased knowledge about the importance of exercise. Thus, these findings are consistent with the documented findings that healthy habits should be instilled in children at an early age, inspiring schoolchildren to continue practicing hand hygiene into adulthood (Pogrebna and Kharlamov 2020).
Adolescent students face unique challenges that reduce their commitment to and practices of handwashing. Adolescent handwashing is affected by environmental factors. Authors agree that access to handwashing infrastructure is critical to promoting handwashing during critical times (Bulled et al., 2017). According to the study, lack of handwashing facilities accounts for 20% of the reasons for not washing hands. For example, inaccessible handwashing facilities or unsanitary amenities. One reason for adolescents not washing their hands is a lack of handwashing infrastructure. However, when considering handwashing facilities, it is also important to consider their standard (Grimason et al. 2014; Pogrebna and Kharlamov 2020).
This study increases nursing students’ knowledge of the most effective strategies for improving care through infection prevention. The findings of this study will assist nursing administrators in hiring nurses who are knowledgeable about hand hygiene and management. This study provides an opportunity to initiate research into the care practices that nurses might adopt to assist patients with hand hygiene-related illnesses. Schools must ensure that students have adequate access to toilets with sinks and hand hygiene materials, and that there are no barriers to proper washroom use. Recommendations to schedule counseling sessions for students who are ill or at risk of illness, advising them to protect themselves and their peers from pathogen spread through the use of healthy behaviors such as social distance and hand hygiene (Pogrebna and Kharlamov 2020).
Because of the cross-sectional nature of the study and the use of a convenient sampling method in the online survey, the findings of this study cannot be generalized. The knowledge gained from this study indicates that effective handwashing among students can only be achieved through the combination of a number of different factors. Because of the lack of individual rapport between the participants in online questionnaires, the validity of the responses may be reduced as a result. A further external threat exists to the validity of history, given the study’s timing, which coincided with the pandemic, and in particular, its section on the importance of proper hand washing. A threat of this nature also has an impact on the generalization of results (Pogrebna and Kharlamov 2020).
Future research on this topic should examine the Saudi government’s role in raising civic awareness in schools and other sectors. Students’ understanding of hand hygiene must be improved. Students should learn how to wash their hands as a life lesson. To help students learn this vital life skill properly, schools and communities must promote increased knowledge of hand hygiene and infection prevention. Hand washing can be learned and practiced throughout the day. As a result, all secondary schools should have a hand hygiene education program run by school nurses. All secondary school students should be educated by school nurses. The content will cover the importance of handwashing, risk behavior, preventive control measures, and universal precautions (Pogrebna and Kharlamov 2020).
Schools and healthcare facilities can use self-learning, pamphlets, booklets, and exhibits to help students learn more. High school students must be motivated to learn about the most common habits and change their unhealthy attitudes into wellness behaviors. Teachers and school nurses should help students recognize when hand hygiene is required and teach them how to do it correctly. Hand washes with soap and water are preferred in some cases, but waterless hand sanitizers can be used in schools. Hand hygiene should be viewed as a lifestyle change for students. For example, during a pandemic, a better understanding of WASH and hygiene culture is critical (Pogrebna and Kharlamov 2020).
CONCLUSION: The findings of the present study confirm the majority of students prefer water and soap as their primary hand-washing materials at school. Additionally, it indicates that in the Saudi Arabian student population, handwashing behavior improves with age and increased knowledge about the importance of exercise. Additionally, it demonstrates that the Saudi Arabian education sector requires effective hygiene education programs in schools and various sectors of society to raise awareness about the importance of hand hygiene.
REFERENCES
Adriaenssens, N., Al Bashtawy, B. M. and Alcorn, J. J. (2015). journal homepage: www. elsevier. com/locate/ejon, European Journal of Oncology Nursing, 19, 748e749.
Ahmed, J., Wong, L. P., Chua, Y. P., et al. (2021). Drinking water, sanitation, and hygiene (WASH) situation in primary schools of Pakistan: the impact of WASH-related interventions and policy on children school performance, Environmental Science and Pollution Research, 1-19.
Al-Hazmi, A., Gosadi, I., Somily, A., et al. (2018). Knowledge, attitude and practice of secondary schools and university students toward Middle East Respiratory Syndrome epidemic in Saudi Arabia: A cross-sectional study, Saudi journal of biological sciences, 25(3), 572-577.
Besha, B., Guche, H., Chare, D., et al. (2016). Assessment of hand washing practice and it’s associated factors among first cycle primary school children in arba minch town, ethiopia, 2015, Epidemiology (Sunnyvale), 6(247), 2161.
Bolds, C., Education, S. A., Center, T., et al. (2019). The development of this plan would not have been possible without the participation and commitment made from approximately 120 people who attended Ending the Epidemic (EtE) Action Committee meetings from June through October 2018. Too long of a list to include here, they are identified by name in Appendix ii. Their role in and importance to this process cannot be overstated.
Bolon, M. (2011). Hand hygiene, Infectious Disease Clinics, 25(1), 21-43.
CAHYANI, H. (2017). A Job Training Report As A Tour Guide At Heroes Monument And Museum Of 10 November Surabaya From January 16th To February 20th 2017, unpublished thesis, Universitas Airlangga.
Cevizci, S., Uludag, A., Topaloglu, N., et al. (2015). Developing students hand hygiene behaviors in a primary school from Turkey: A school-based health education study, Int J Med Sci Public Health, 4(2), 155-61.
Cutler, R. (2010). Promoting hygiene in schools: Breaking the chain of infection, British Journal of School Nursing, 5(4), 187-190.
Delea, M. G., Snyder, J. S., Woreta, M., et al. (2020). Development and reliability of a quantitative personal hygiene assessment tool, International journal of hygiene and environmental health, 227, 113521.
Grimason, A. M., Masangwi, S. J., Morse, T. D., et al. (2014). Knowledge, awareness and practice of the importance of hand-washing amongst children attending state run primary schools in rural Malawi, International journal of environmental health research, 24(1), 31-43.
Indicators, O. (2009). Education at a Glance, Dosegljivo, 25(2011), 362-365.
Khan, I. A., Jahan, P., Hasan, Q. et al. (2019). Genetic confirmation of T2DM meta-analysis variants studied in gestational diabetes mellitus in an Indian population, Diabetes Metab Syndr, 13(1), 688-694.
Luby, S. P., Halder, A. K., Huda, T., et al. (2011). The effect of handwashing at recommended times with water alone and with soap on child diarrhea in rural Bangladesh: an observational study, PLoS medicine, 8(6), e1001052.
Mahmud, M. A., Spigt, M., Bezabih, A. M., et al. (2015). Efficacy of handwashing with soap and nail clipping on intestinal parasitic infections in school-aged children: a factorial cluster randomized controlled trial, PLoS medicine, 12(6), e1001837.
Organization, W. H. (2014). Global status report on noncommunicable diseases 2014, World Health Organization.
Pati, F., Jang, J., Ha, D.H., et al. (2014). Printing three-dimensional tissue analogues with decellularized extracellular matrix bioink, Nature communications, 5(1), 1-11.
Pogrebna, G. and Kharlamov, A. (2020). The impact of cross-cultural differences in handwashing patterns on the COVID-19 outbreak magnitude, Regulation and Governance.
Waltz, C. F., Strickland, O. L. and Lenz, E. R. (2010). Measurement in nursing and health research, Springer publishing company.
Wilkinson, M., Toit, A. and Mashimbye, D. (2012). Development of a Framework for Hand Hygiene Assessment.

