1Department of Biology and Microbiology, SSIT, Skyline University, Zaria Road, Kano, Nigeria and
2Huma Cancer Society, Ganj Plaza, 2nd Floor 42, Hazratganj, Lucknow – 226001, UP India
Corresponding author email: sanjoykpal@gmail.com
Article Publishing History
Received: 21/04/2020
Accepted After Revision: 15/06/2020
Due to lack of awareness about cancer, shortage of oncologists & infrastructure, and above all, financial crunch compels many Indian patients to avoid conventional treatment or report to a clinic with advanced malignant disease. As a result, curative treatment is not an option in most of the cases. Thus, many patients have to depend on some form of alternative therapy for the treatment of cancer. One of the most sought after therapy is polyherbal medicine. We follow-up two suspected cancer patients trying an alternative polyherbal therapy HUMA. This polyherbal therapy comprises of various important anti-cancer herbs described in Ayurvedic literature viz. Azadirachta indica, Curcuma longa, Embelica officinalis, Ocimum sanctum, Semecarpus anacardium, and Tinospora cordifolia, among others. Both the patients were immensely benefited by this polyherbal therapy. Complete regression of the disease/tumour was observed in both the patients. In the absence of any conventional therapy, the disease regression observed could be attributed to alternative polyherbal therapy. As a large number of terminal cancer patients try various herbal therapies all over the globe; hence, proper research attention should be given in this area.
Alternative cancer, HUMA, polyherbal therapy, CAM
Pal S. K, Fatima S. H. Adventurism in Herbal Medicine the Only Option for Economically Challenged Indian Cancer Patients: Perspective Based on Case Histories. Biosc.Biotech.Res.Comm. 2020;13(2).
Pal S. K, Fatima S. H. Adventurism in Herbal Medicine the Only Option for Economically Challenged Indian Cancer Patients: Perspective Based on Case Histories. Biosc.Biotech.Res.Comm. 2020;13(2). Available from: https://bit.ly/3cijRDA
Copyright © Pal and Fatima This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-BY) https://creativecommns.org/licenses/by/4.0/, which permits unrestricted use distribution and reproduction in any medium, provide the original author and source are credited.
INTRODUCTION
India faces a major disease burden from cancer (Dhillon et al., 2018). This non-communicable disease carries high levels of mortality and disability and requires expensive treatments. The cancer scenario in India is quite alarming. India has some of the highest cancer rates in the world (Mudur, 2005). Due to lack of awareness about cancer, shortage of oncologists & infrastructure (Khan, 2018), and above all, financial crunch (Mahal et al., 2013) compels many Indian patients either to avoid conventional treatment or report to a clinic with advanced malignant disease (Pal, 2002). As a result, curative treatment is not an option in most of the cases. Moreover, the expense of conventional treatment is not always within the reach of many patients compelling them to abandon it and venture elsewhere in search of treatment. The financial toxicity of cancer treatment is now a well-recognized problem in cancer (Gyawali, 2017).
Medicinal plants are considered to be one of the most popular alternative therapeutic modalities for cancer patients (Gratus et al., 2009). and may also be cost-effective (Chaudhary et al., 2015). India has a very long, safe, and continuous usage of many herbal drugs in the officially recognized alternative systems of health (Vaidya and Devasagayam, 2007).
Medicinal plants hold a special place in India. Herbal medicine in India has been refined by thousands of years of practical application and experience. In India, a substantial proportion of the population uses herbal drugs for their primary health care needs (WHO, 2003). After conventional treatment fails to cure chronic malignancy the biggest predicament of cancer patients and their caregivers is the acceptance of the grim reality of death. Most of the patients and their caregivers are not likely to give up easily and may end up trying some alternative herbal therapy. In some instances, the patients often do not disclose the use of alternative therapy (Sanford et al., 2019). However, for many Indian patients, conventional therapy is a luxury which they just cannot afford. In this article, the follow up of two suspected cancer patients who tried a polyherbal therapy ‘HUMA’ for treatment is described.
Huma Therapy
This polyherbal formulation for the treatment of cancer was first advocated by Dr. S M Atiq in Lucknow in the late 80s and now over 500 cancer patients try this therapy every year (Pal, 2013). The polyherbal formulation comprising of various anti-cancer herbs viz. Azadirachta indica, Curcuma longa, Embelica officinalis, Ocimum sanctum, Semecarpus anacardium, and Tinospora cordifolia, among others. This polyherbal medicine is orally administered and well tolerated by patients. Instances of adverse side effects are less due to individual dosing of the medicine. The dose of the medicine is not fixed; rather it is titrated according to the patient’s condition and maybe one of the main reasons for the lack of adverse effects. Though most of the patients try this polyherbal therapy mainly for palliation; however, there are some reports of complete regression of cancer/tumour, especially oral tumours with HUMA (Pal and Fatima, 2014; Pal and Fatima, 2017a).
Case 1: A 74 year old lady presented with allergic bronchitis on April 15, 2003. She had an earlier history of Chronic Obstructive Pulmonary Disease (COPD); however, her abdominal USG and chest X-ray were normal. She was advised and continued allopathic medication for the next 4 months. Two months later she started having difficulty swallowing solid as well as liquid food. The patient then underwent a barium swallow test on May 23, 2003. The report indicated irregularity in the lateral wall of thoracic esophagus with proximal dilation of cervical esophagus suggestive of esophageal carcinoma. In view of old age and financial problems the caregivers of the patient did not consent for any curative therapy. Hence, a biopsy was not done. She was on palliative therapy till October 2003, then her health condition deteriorated drastically and she became very sick. She was then admitted to Lucknow Cancer Institute on October 05, 2003, for supportive and palliative treatment. On October 10, 2003, the patient again underwent a barium swallow test.
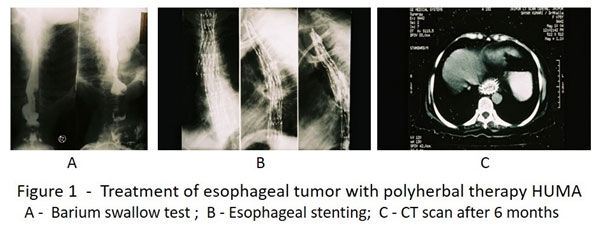
The study revealed a tracheoesophageal fistula at D1 vertebral level with the opacification of tracheo bronchial tree. Barium study also revealed the growth of tumor extended to the C6 vertebral level. Covered metallic stents were placed from C7 vertebral (Lower end) and extended below to cover the fistula. The patient was advised radiotherapy; however, the patient was not in a position to undergo any conventional therapy. She opted for the polyherbal therapy mainly for palliation from October 15, 2003. When the therapy started the patient was anorexic and cachexic. Remarkable clinical improvement was noticed in the patient after the start of therapy. Within 15 days the patient regained her normal appetite. The next 6 months were relative event free. In the first week of April 04 the patent started having breathing problems. She underwent a CT scan of the chest and upper abdomen on May 10, 2004. The study revealed no mass/lesion around the two metallic stents placed in the esophagus (Figure 1). Her problem was managed with allopathic medicines. Two months after this incidence the patient expired due to cardiorespiratory arrest.
Case 2: A 43 year old male who presented with acute epigastric pain radiating to his back on February 26, 1998. An abdominal ultrasound dated March 1, 1998 revealed marked dilatation of pancreatic duct and findings suggestive of an acute exacerbation of chronic pancreatitis. The patient was offered and received conventional therapy for 2 months; however, his condition did not improve. An abdominal ultrasound dated May 2, 1998 revealed a slightly bulky pancreas with an irregularly dilated pancreatic duct with bulky head of pancreas suggested of either chronic pancreatitis or carcinoma at the head of pancreas. He was advised to undergo an ERCP and was given an enzyme supplement for the treatment of chronic pancreatitis. Despite medication his upper abdominal pain continued to increase. An abdominal CT scan dated October 7, 1998 indicated a pancreatic head neoplasm with multiple cystic components, dense calcification, dilated pancreatic duct and atrophic pancreatic body and tail regions. A CT guided biopsy of the pancreatic tumor was suggested.
The suggested treatment plan involved surgery; however, the patient declined because of his financial constraints. He was a motorcycle repair mechanic and the money required for conventional treatment was beyond his reach. Instead he opted for the polyherbal HUMA therapy from November 10, 1998. A gradual improvement in his condition was noted after the start of polyherbal therapy. After about 3-4 months of therapy, his appetite improved, the abdominal pain was gone, and he resumed normal activities. He continued the herbal therapy for 11 months and then stopped the therapy. An abdominal ultrasound dated September 20, 2003 was reported as normal aside of some fatty changes in the liver (Figure 2). We followed the patient for the next 5 years and he was leading a normal life.
DISCUSSION
In the absence of any conventional therapy, the disease regression observed in both the patients could solely be attributed to the alternative polyherbal therapy. Though the biopsy of these patients could not be performed; however, complete regression of cancer was observed with HUMA in many other patients (Pal and Fatima, 2017a; Pal & Fatima, 2014; Pal, 2013; Pal et al., 2013). In few terminal cancer patients prolongation of survival time was also note with HUMA (Pal & Fatima 2017b).
In India, not all cancer patients have the luxury to undergo conventional therapy or allopathic follow-up. When cancer struck, many have to search for their own treatment options, be it herbal, traditional, local, or black magic. Many patients try all these therapies out of financial compulsion and in some when conventional therapy fails to cure their cancer. In the first case the caregivers of the patient did want conventional therapy due to the advanced age of the patient and in the second case finance was again the main constrain. Accessing good cancer care is a big issue for many living in the developing world (Jack, 2014). The cost of treatment for advanced cancer may cost millions of rupees a year. Only a few patients are able to bear the cost (Goyal, 2014). Government health schemes like Yashaswini, Arogyashri, and Vajpayee Arogya Yojana did not cover cancer (Anonymous, 2014). However, the recently introduced ‘Ayushman Bharat’ the National Health Protection Scheme (NHPS), will now cover the cancer treatment cost including radiation and chemotherapy which do not need hospitalization (Sharma, 2018).
People have used herbal medicines throughout our human history and they are currently the most commonly used medicines worldwide. Herbal medicines are in great demand in the developed world for primary health care due to their efficacy, safety, and lesser side effects. According to WHO about 70 – 80 % of the people in African and Asian countries are primarily dependent on the herbals of treatment of various diseases (Vijayaalakshmi, 2015). Medicinal plants maintain the health and vitality of individuals and also cure various diseases, including cancer without causing toxicity. These medicinal plants possess good immunomodulatory and antioxidant properties, leading to anticancer activities. The antioxidant phytochemicals protect the cells from oxidative damage (Patil et al., 2013).
The herbals that are presently used for treatment are also known for their anti-cancer activity viz Azadirachta indica (Al Saiqali et al., 2018), Curcuma longa (Willenbacher et al., 2019), Embelica officinali, (Baliga and Dsouza, 2011), Ocimum sanctum (Baruah & Kma, 2019) Semecarpus anacardium (Joseph et al., 2013), and Tinospora cordifolia (Ansari et al., 2017). As compared to conventional chemotherapy the polyherbal therapy HUMA is not only less expensive but also produced lesser side effects (Pal, 2013).
Cancer arises from various genetic defects, either in isolation or familial (Hannah-Shmouni and Stratakis, 2020). Increased levels of telomerase are found in the vast majority of human cancers (Roake and Artandi, 2020). For the successful treatment of cancer, there is a need for an altogether different approach that can target the individual cancer cells at a molecular level. Cell therapies present an entirely new paradigm in drug development. Within this class, immune cell therapies are among the most advanced, having already demonstrated definitive evidence of clinical benefits in cancer and infectious disease. Continued advances in fundamental immunology, genetic engineering, gene editing, and synthetic biology exponentially expand opportunities to enhance the sophistication of immune cell therapies, increasing potency and safety and broadening their potential for the treatment of disease (Weber et al., 2020).
However, these advances in molecular medicine will come at a price that is far from the reach of the common people of our country. Be it India or Africa (Omara et al., 2020) cancer patients across the globe depend on some form of herbal therapy. Two important commercial anti-cancer drugs vincristine and vinblastine are derived from a plant Catharanthus roseus (L.) G. Don (Nobili et al., 2009). Anti-cancer activity is reported in many plants; however, the proper clinical trial is lacking in herbal medicine due to a lack of standardization of the medicine. The anti-cancer herbals that are used by patients are often very toxic in nature. Hence, small doses and frequent titration of the medicines are required which makes them unsuitable for the clinical trial. Many herbal therapy created tremendous interest in the past. Essiac is one of the most popular herbal cancer alternatives in North America. PC-SPES is one of the most studied herbal therapies in prostate cancer. It is comprised of a combination of eight herbal compounds (Pal and Fatima, 2014). Mistletoe (Viscum album L.) still continues to be the medical herb prescribed most frequently for cancer patients in German-speaking countries (Rostock, 2020).
In India, Carctol an alternative herbal cancer therapy developed by Dr. Nandal Tiwari is quite popular. This herbal therapy is composed of 8 different herbs viz. Hemidesmus Indicus, Tribulus Terrestris, Piper Cubeba Linn, Ammani Vesicatoria, Lepidium Sativum Linn, Blepharis Edulis, Smilax China Linn and Rheumemodi Wall. (Pal, 2013). A dietary regimen ‘Sarvapasti’ developed by the scientist of D S Research, Varanasi has also become a very popular alternative therapy for cancer patients. Sarvapasti contains many important medicinal herbs (Ghosh, 2002). Maharishi Amrit Kalash [MAK] produced by the ‘Maharishi Ayurvedic Products’ is a polyherbal preparation of many important Ayurvedic herbs. This formulation was shown to be effective in patients undergoing chemotherapy (Maharishi AyurVeda).
CONCLUSION
Due to ignorance and lack of effective cancer screening process many treatable cancer patients land in the cancer clinics with advanced disease when virtually not curative treatment is possible (Broom et al., 2009). Waiting time for cancer treatment is more in India due to a lack of infrastructure and treatment facilities. Above all, financial problems will push many cancer patients to alternative practitioners with no allopathic qualifications and having limited knowledge about oncology. From the present observation, it can be concluded that not all alternative herbal cancer therapies may be evil. Some like HUMA may show some beneficial effect whereas others may be completely bogus. The need of the hour is a comprehensive dialogue between practitioners of different systems of medicine so that the good therapies are identified and the bad ones are weeded out. The overall aim should be to offer affordable evidence-based best cancer treatment and palliation to economically challenged patients in a developing country like India.
ACKNOWLEDGMENT
The fellowship offered to SKP from 2005 to 2006 for his postdoctoral study in the Department of Gastroenterology, Sanjay Gandhi Postgraduate of Medical Sciences, Lucknow from the Indian Council of Medical Research, New Delhi to study various complementary and alternative cancer medicines in north India is duly acknowledged. The clinical data present here was collected while working on this project.
Conflict of interest: Dr. S Hina Fatima is the practicing clinician and President of the Huma Cancer Society, Lucknow.
REFERENCES
Al-Saiqali, M., Tangutur, A. D., Banoth, C., & Bhukya, B. (2018) Antimicrobial and anticancer potential of low molecular weight polypeptides extracted and characterized from leaves of Azadirachta indica. Int J Biol Macromol Vol. 114: Pages 906-921.
Anonymous. (2014) Is India prepared for a cancer tsunami? September 19. Accessed from: http://qz.com/268716/is-india-prepared-for-a-cancer-tsunami/
Ansari, J. A., Rastogi, N., Ahmad, M. K., Mahdi, A. A., Khan, A. R., Thakur, R., Srivastava, V. K., Mishra, D. P., Fatima, N., Khan, H. J., & Waseem, M. (2017) ROS mediated pro-apoptotic effects of Tinospora cordifolia on breast cancer cells. Front Biosci (Elite Ed.). Vol. 9: Pages 89-100.
Baliga, M. S., & Dsouza, J. J. (2011) Amla (Emblica officinalis Gaertn), a wonder berry in the treatment and prevention of cancer. Eur J Cancer Prev Vol. 20 No 3: Pages 225-239.
Baruah, T. J., & Kma, L. (2019) Vicenin-2 acts as a radiosensitizer of the non-small cell lung cancer by lowering Akt expression. Biofactors Vol. 45 No 2: Pages 200-210.
Broom, A., Nayar, K., Tovey, P., Shirali, R., Thakur, R., Seth, T., Chhetri, P. (2009) Indian cancer patients’ use of Traditional, Complementary and Alternative Medicine (TCAM) and delays in presentation to hospital. Oman Med J Vol. 24 No 2: Pages 99-102.
Chaudhary, T., Chahar, A., Sharma, J. K., Kaur, K., & Dang, A. (2015) Phytomedicine in the treatment of cancer: A Health Technology Assessment. J Clin Diagn Res Vol 9 No 12: Pages XC04-XC09.
Dhillon, P. K., Mathur, P., Nandakumar, A., & Fitzmaurice C. (2018). The burden of cancers and their variations across the states of India: the global burden of disease study 1990–2016. The Lancet Oncology Vol. 19 No 10: Pages 1-18.
Ghosh A. (2002) Wonder drug up for expert scrutiny. The Times of India, Kolkata, May 16. Accessed from: https://tinyurl.com/y88z7qfe.
Goyal, D. (2014). Cancer patients plagued by long wait for little funds. The Indian Express, Ludhiana March 14. Accessed from: https://tinyurl.com/yb2b2vmh.
Gratus, C., Wilson, S., Greenfield, S. M., Damery, S. L., Warmington, S. A., Grieve, R., Steven, N. M., & Routledge, P. (2009) The use of herbal medicines by people with cancer: a qualitative study. BMC Complement Altern Med Vol. 9: 14.
Gyawali, B. (2017) Low-value practices in oncology contributing to financial toxicity. E cancer medical science Vol 11: 727. Accessed from: https://tinyurl.com/ya2j766e.
Hannah-Shmouni, F., & Stratakis, C. A. (2020) A gene-based classification of primary adrenocortical hyperplasias. Horm Metab Res Vol. 52 No 3: Pages133-141.
Jack A. (2014) Access to good therapy is big issue for cancer patients in poorer nations. Financial Times, September 26. Accessed from: https://tinyurl.com/y8dkqj37.
Joseph, J. P., Raval, S. K., Sadariya, K. A., Jhala, M., & Kumar, P. (2013) Anti cancerous efficacy of Ayurvedic milk extract of Semecarpus anacardium nuts on hepatocellular carcinoma in Wistar rats. Afr J Tradit Complement Altern Med. Vol. 10 No 5: Pages 299-304. eCollection 2013.
Khan, S.A. (2018) The cancer refugees. The Indian Express, July 23. Accessed from: https://tinyurl.com/y85paxx3.
Mahal, A., Karan, A., Fan, V.Y., & Engelgau, M. (2013) The economic burden of cancers on Indian households. PLoS One Vol. 8 No 8:e71853. doi: 10.1371/journal.pone.0071853.
Maharishi AyurVeda. Summary of research findings. Accessed from: https://www.imavf.org/wp-content/uploads/MAV_Summary_of_Research_Findings.pdf
Mudur, G. (2005) India has some of the highest cancer rates in the world. BMJ Vol. 30 No 7485: Page 215.
Nobili, S., Lippi, D., Witort, E. et al., (2009) Natural compounds for cancer treatment and prevention, Pharmacological Research Vol. 59 No 6: Pages 365–378.
Omara, T., Kiprop, A. K., Ramkat, R. C., Cherutoi, J., Kagoya, S., et al. (2020) Medicinal plants used in traditional management of cancer in Uganda: a review of ethnobotanical surveys, phytochemistry, and anticancer studies. Evid Based Complement Alternat Med. Article ID 2020:3529081. doi: 10.1155/2020/3529081. eCollection.
Pal, S. K. (2002) Use of alternative cancer medicines in India. Lancet Oncology Vol. 3 No 7: Pages 394 – 395.
Pal, S. K. (2013) Cancer alternative therapy HUMA: a clinical perspective. Annals of Ayurvedic Medicine Vol. 2 No 3: Pages 80-88.
Pal, S. K., Fatima, S. H., & Kalandar, A. (2013) Effect of poly herbal preparation HUMA on oral cancer: Two case reports. Translational Medicine & Biotechnology Vol. 1 No 1: Pages 65 – 69.
Pal, S. K., & Fatima, S. H. (2014) Cancer treatment with the alternative herbal medicine HUMA: Two case reports. Middle East J Cancer Vol. 5 No 1: Pages 41 – 46.
Pal, S. K., & Fatima, S. H. (2017a) Herbal cancer remedy: an alternative treatment option for cancer patients. Clinics in Oncology Vol. 2: Article 1299. May 17. Accessed from: http://www.clinicsinoncology.com/pdfs_folder/cio-v2-id1299.pdf
Pal, S. K., & Fatima, S. H. (2017b) Prolongation of survival time of incurable terminal cancer patients with herbal medicines. International Archives of Integrated Medicine. Vol. 4 No 6: Pages 149-156.
Patil, S. D., Chaudhari, M. A., Sapkale, P. V., & Chaudhari, R. B. (2013) A recent review on anticancer herbal drugs. J Drug Discov Therapeutics Vol. 1 No 6: Pages 77-84.
Roake, C. M., & Artandi, S. E. (2020) Regulation of human telomerase in homeostasis and disease. Nat Rev Mol Cell Biol. Published online on April 2. doi: 10.1038/s41580-020-0234-z.
Rostock, M. (2020) [Mistletoe in the treatment of cancer patients]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 63(5):535-540. doi: 10.1007/s00103-020-03122-x.
Sanford, N. N, Sher, D. J., Ahn, C., Aizer, A. A., & Mahal, B. A. (2019) Prevalence and nondisclosure of complementary and alternative medicine use in patients with cancer and cancer survivors in the United States. JAMA Oncol Vol. 5 No 5: Pages735-737.
Sharma, S. (2018) Fighting cancer with cheap treatment and screening. Sep 23. Hindustan Times, New Delhi. Assessed from: https://tinyurl.com/y2khj3hr.
Vaidya, A. D. B., & Devasagayam, T. P. A. (2007) Current status of herbal drugs in India: an overview. J Clin Biochem Nutr Vol. 41 No 1: Pages 1–11.
Vijayaalakshmi, L. G. (2015) Herbal remedy for liver cancer – Review. J Pharm Sci & Res. Vol. 7 No 1: Pages 21-24
Weber, E. W., Maus, M. V., & Mackall, C. L. (2020) The emerging landscape of immune cell therapies. Cell Vol. 181 No 1: Pages 46-62.
Willenbacher, E., Khan, S. Z., Mujica, S. C. A., Trapani, D., Hussain, S., Wolf, D., Willenbacher, W., Spizzo, G., & Seeber, A. (2019) Curcumin: New insights into an ancient ingredient against cancer. Int J Mol Sci. Vol. 20 No 8: Pages (pii) E1808.
World Health Organization (2003) Fifty-sixth world health assembly, A56/18 provisional agenda item 14.10. 2003. [Assessed from: http://apps.who.int/gb/archive/pdf_files/WHA56/ea5618.pdf].

