1General Practitioner, Ministry of Health, Baish General Hospital, Jazan, Saudi Arabia
2General Practitioner, Ministry of Health, Alsahaleel Primary Health Care, Jazan, Saudi Arabia
3General Practitioner, Ministry of Health, Albadi and Algarafi Primary Health Care, Jazan, Saudi Arabia
4Intern Department, College of Dentistry, Jazan University, Jazan, Saudi Arabia
5Postgraduate Students, Sanaa University, Sana’a, Republic of Yemen
6General Practitioner, Ministry of Health, Samtah General Hospital, Samtah, Jazan, Saudi Arabia
6Department of Prosthetic Dental Science, College of Dentistry, Jazan University, Jazan, Saudi Arabia
Corresponding author email: drmoaleem2014@gmail.com
Article Publishing History
Received: 27/10/2020
Accepted After Revision: 15/12/2020
Here we summarize the original studies and case reports addressing the root and root canal morphology of permanent anterior teeth among the Saudi Arabian population, comparing findings to the international literature. The maxillary and mandibular central and lateral incisors are among the most likely teeth to require endodontic treatments, so their morphology should be considered for root canal treatment success. All related literature published between 1980 and 2020 in peer-reviewed journals were included in this review. A systematic literature exploration was carried-out using the PubMed, ScienceDirect, Scopus, Evidence-Based Dentistry Journal, and Dental Practice databases. The search terms used were: “root canal morphology”, “root morphology”, “case report for anterior maxillary and mandibular teeth”, and “Saudi Arabian population”. Twenty-nine original research articles were identified. Most of the studies used the cone beam computed tomography (CBCT) technique. A total of 29 original research studies were included in this review. In the Saudi-based original research, three studies addressed mandibular and one study maxillary teeth and were conducted in various cities. Twenty-nine clinical case reports are presented: among these, three were Saudi patients. When comparing Saudi data to data gathered in other populations, the findings were mostly consistent in canal and root configuration of maxillary and mandibular anterior teeth. New devices and technologies are clinically useful in the identification of morphological variations in permanent teeth. Greater attention should be given to detecting additional canals. Variation among canals of mandibular anterior and maxillary teeth should be considered for successful endodontic treatment.
Canal Configuration, Case Report, Mandibular Teeth, Maxillary Teeth, Root Canal System, Morphology, Saudi Arabia
Dallak A. E, Moafa W. M, Malhan S. M, Shami A. O, Alhaj W. S, Kariri M. A, Al-Moaleem M. M. Root and Canal Morphology of Permanent Maxillary and Mandibular Incisor Teeth: A Systematic Review and Comparison with Saudi Arabian Population. Biosc.Biotech.Res.Comm. 2020;13(4).
Dallak A. E, Moafa W. M, Malhan S. M, Shami A. O, Alhaj W. S, Kariri M. A, Al-Moaleem M. M. Root and Canal Morphology of Permanent Maxillary and Mandibular Incisor Teeth: A Systematic Review and Comparison with Saudi Arabian Population. Biosc.Biotech.Res.Comm. 2020;13(4). Available from: <a href=”https://bit.ly/3m4q9vI”>https://bit.ly/3m4q9vI</a>
Copyright © Dallak et al., This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-BY) https://creativecommns.org/licenses/by/4.0/, which permits unrestricted use distribution and reproduction in any medium, provide the original author and source are credited.
INTRODUCTION
All root canal treatments (RCTs) rely on knowledge of the tooth morphology, and three-dimensional imaging of root canal systems (Castellucci., 2015; Bansal et al., 2018). It has been reported that the shape and number of roots and canals differ among genders and populations (Al‑Fouzan et al., 2012; Mirhosseini et al., 2017; Saati et al., 2018; Mashyakhy., 2019; Valenti-Obino et al., 2019; Baxter et al., 2020; Ghabbani et al., 2020). Therefore, it is important to be familiar with differences in the tooth outlines and characteristic features among ethnicities. Such knowledge can aid in the location and negotiation of canals (Arslan et al., 2015; Zhengyan et al., 2016; Verma et al., 2017; Martins et al., 2018; Martínez et al., 2018; Popovic et al., 2018; Shemesh et al.,2018).
A study classified the cross‑sectional root canal configurations of mandibular teeth as round, oval, long oval, flattened, or irregular (Castellucci 2015). Whoever the majority of permanent of maxillary or mandibular incisors have one root and one canal; however, a small percentage may have a second canal, lateral canal, or apical deltas (Saati et al., 2018). The root canal systems of incisors do not consist of a single canal running uniformly from the orifice of the pulp champers to the apex. In fact, the root canal systems of incisors can be complex due to the splitting and reunion of the canals during its passage to the end of the roots (Vertucci., 1984; Saini et al., 1990; Altunsoy et al., 2014; Razumova et al., 2018; Mashyakhy and Gambarini., 2019; Pan et al., 2019). The root canal systems of incisors open apically into the periodontium through apical and lateral foramens. During its passage, the root canal presents a variety of configurations, differing among tooth types, genders, and populations (Mirhosseini et al., 2017; Martínez et al., 2018; Popovic et al., 2018; Mashyakhy and Gambarini., 2019). Recently, Neelakantan et al (2010) and Przesmycka and Tomczyk (2016) have compared the efficacy of various methods for visualizing the canal and root morphology. These authors concluded that CBCT is accurate, high-resolution, and can be useful for detailed quantitative and qualitative descriptions of the RC anatomy, (Neelakantan et al., 2010; Filpo–Perez et al., 2015; Przesmycka and Tomczyk., 2016; Martinsa et al., 2020).
Some reviews have noted high global rates of a second canal in the anterior central and lateral incisors (20.4% and 25.3%), respectively (Martinsa et al., 2020), while some studies have reported greatly varying numbers of canals and canal types among the same teeth (Ahmad., 2015; Ahmed and Hashem., 2016; Bansal et al., 2018; Martins et al., 2019). All the published reviews that we identified have noted that knowledge of these preoperative variables could help clinicians anticipate more complex RC anatomic configurations, thus minimizing the possibility of lost canals during treatment. Investigators use various morphological characteristics to classify root canal systems e.g., the number of canals from orifice to apex, the sum of roots and number of canals in each root, or the number of isthmuses (Vertucci., 1984; Bansal et al., 2018), but the most widely used is Vertucci’s classification, which classifies root canal systems into eight types.
Variations in the morphology of the canals and roots of maxillary and mandibular central or lateral incisor teeth have been noted in in vivo and in vitro studies (Vertucci., 1984; Saini et al., 1990; Caliskan et al., 1995; Al‑Quadah and Awawdeh; 2006; Weng et al., 2009; Al‑Fouzan et al., 2012; Aminsobhani et al., 2013; Altunsoy et al., 2014; Lin et al., 2014; Zhao et al., 2014; Arslan et al., 2015; Zhengyan et al., 2016; da Silva et al., 2016; Martins et al., 2017; Verma et al., 2017; Mirhosseini et al., 2017; Saati et al., 2018; Martins et al., 2018; Martínez et al., 2018; Popovic et al., 2018; Shemesh et al., 2018; Razumova et al., 2018; Mashyakhy M., 2019; Valenti-Obino et al., 2019; Mashyakhy and Gambarini., 2019; Pan et al., 2019; Bourzgui and Akarslan., 2020; Ghabbani et al., 2020; Baxter et al., 2020) (Table 1), and in case reports (Hwang and Min., 2005; Al-Madi., 2020) (Table 2).
However, only a few of those studies were original research by Saini et al., 1990; Al‑Fouzan et al., 2012; Mashyakhy M., 2019; Mashyakhy and Gambarini., 2019; Ghabbani et al., 2020, or case reports by Al-Nazhan., 1991; Alenazy et al., 2019; Al-Madi., 2020, conducted in Saudi Arabia. Here we summarize the published Saudi studies and investigate the number of canals and root morphology of maxillary and mandibular anterior teeth and making comparisons with the global data in relation to the original researches or case reports.
Search Methodology: All peer-reviewed original research articles or case reports for maxillary and/or mandibular central and lateral incisors from 1980 to 2020 addressing root or root canal morphology of permanent teeth were included in this review. A systematic literature review was carried out using the PubMed, Science Direct, Scopus, Evidence-Based Dentistry, and Journal of Evidence-Based Dental Practice databases. The search terms used were: “root canal morphology”, “root morphology”, “case report for anterior maxillary and mandibular teeth”, and “Saudi Arabian population”. All irrelevant or duplicate articles were excluded; the full texts of whole original researches or case reports were screened and saved in a single folder. In addition, all volumes or issues of the Saudi Dental Journal and Saudi Endodontic Journal were manually investigated for related topics. Lastly, the article reference lists were checked for further eligible articles.
Data Collections Original Researches: A total of 29 original research studies (18 mandibular teeth, seven maxillary teeth, four both teeth) were identified. Nineteen of the maxillary teeth studies were clinical studies that used CBCT, and three were laboratory studies using the clearing technique. Seven of the mandibular teeth studies used CBCT and a single study used radiograph, while the other three used the clearing technique. Three of the studies were original Saudi research involving mandibular teeth (Al‑Fouzan et al., 2012; Mashyakhy., 2019; Ghabbani et al., 2020), were done in Al Madinah Al Munawara, Jazan, and Riyadh, respectively.
Also, two Saudi studies, done in Riyadh and Jazan (Saini et al., 1990; Mashyakhy and Gambarini., 2019), involved maxillary teeth. The author names, the year the study was conducted, country, sample size, type of tooth, genders, and anatomical features and finding are given in Table 1. Also, significant differences were recorded when comparing genders, sides, types of teeth, bilateral symmetry, and techniques used. The anatomical features and finding in relation to Vertucci’s classification were investigated, including the number of roots, number of root canals and their configurations, and other radiographical or anatomical findings.
Few studies in the peer-reviewed literature have investigated the canal and root configuration of the maxillary arches (Table 1). A single Saudi study was carried-out by Mashyakhy and Gambarini., 2019 among a subpopulation in Jazan city, and they found that all maxillary central and lateral incisors were Vertucci’s classification Type I. Another earlier study, published earlier, investigated shovel-shaped and dens invaginates in maxillary central incisors (Saini et al., 1990). Other international studies (Russian, Chinese, and Portuguese participants) reported the same percentages (100%) for their maxillary central and lateral incisors samples, and most of them were Vertucci’s classification Type I (Martins et al., 2017; Razumova et al., 2018; Bourzgui and Akarslan., 2020). Other studies conducted in American, China, and Turkey (Vertucci., 1984; Caliskan et al., 1995; Weng et al., 2009 Altunsoy et al., 2014) reported Type I and Type III rates of 78.05% to 99.5%, respectively, for maxillary incisors. Vertucci’s classification Type V was recorded in 1–4.88% of patients from China, Turkey, and Brazil (Weng et al., 2009; Altunsoy et al., 2014; da Silva et al., 2016).
Table 1. Summary of clinical and laboratory morphological studies of roots and canals number, and canals’ configuration of mandibular and maxillary anterior teeth conducted on SA and worldwide countries
| Researcher (S), Year/Country | Tooth Type & Sample Size | Anatomical Features & %, general finding Tooth Type/ Vertucci Classification Type (N %) Two Gender I II III IV V VI VII Others canals | Sig ↔ Teeth, Gender & Bilateral symmetry, Male: Female % | Technique type |
| Mandibular teeth | ||||
| Ghabbani et al, 2020/KSA, Al‑Madinah Al‑Munawara3
|
812 MN
816 MN
406 Patient |
Central 24.6% 0.00% 21.5% 1.2% 2.4% 1.0%
Lateral 25.6% 0.00% 20.6% 1.2% 7.1% 1.6% Total 50.3% 0.00% 42.3% 0.2% 5.3%, 1.6% Males 45.2% 0.00% 46.9% 0.00% 6%, 1.7% Female 64.8% 0.00% 29.4%, 0.9%, 3.3% 1.4% Saudi 48.7%, 0.00% 44.1% 0.00% 5.3% 1.7% No-Saudi 52.8%, 0.00% 39.4% 0.6%, 5.4% 1.5% |
SD ↔ Type Teeth
SD ↔ Genders Low Symmetry
SD↔Saudi& Non-Saudi Male 300/ Females 106 |
CBCT |
| Mashyakhy M, 2019/ KSA, Jazan4 | 410 MN
412 MN |
Central 73.7% 0.00% 26.3% 26.3%
Lateral 69.2% 0.00% 29.8% 0.00% 1.0% 30.8% Male 67.3% 0.00% 32.7% 32.7% Female 79.4% 0.00% 20.6% 20.6% |
SD ↔ Canal, Side, Type
NSD- Gender Moderate Symmetry Male 48% Female 52% |
CBCT |
| Al‑Fouzan et al, 2012/KSA, Riyadh5 | 40 MN
40 MN |
Central 70% 0.00% 30%
Lateral 70% 0.00% 30% |
Very High symmetry | In-Vitro, clearing dye injection |
| Baxter et al, 2020/ Germany6 | MN
MN 302 Image 1,208 teeth |
Central 76.4% 22.3% 0.00% 0.7% 1.2% 22.6%
Lateral 76.3% 21.4% 0.00% 0.00% 1.0% 24.3% Total 76.4% 21.7% 0.00% 0.00% 1.1%, 0.8% |
NSD ↔ Teeth, Age
SD ↔ Genders High Symmetry Male 116 / Female 186 |
CBCT |
| Mirhosseini et al, 2019/ Iran7 | 330 MN
331 MN 180 Image |
Central 76.1% 0.00% 15.8% 0.6% 7.6% 23.9%
Lateral 65.0% 0.6% 15.7% 0.9%) 17.9% 35.0% |
SD ↔ Tooth Type
Low Symmetry |
CBCT |
| Pan et al, 2019/ Malaysia19 | 408 MN
400 MN 208 Image |
Central 94.9% 0.00% 1.0% 0.00% 4.2%
Lateral 87.8% 0.00% 3.8% 0.3% 8.3% |
NSD↔ Gender& Side
Low Symmetry Male43.3 /Female56.7 |
CBCT |
| Valenti-Obino et al, 2019/Italy8 | 487 MN
491 MN |
Central 55.0% 34.3% 9.3% 0.6% 0.8% 45%
Lateral 57.0% 35.7% 6.9% 0.0% 0.4% 43% |
NSD↔ Teeth Type
High Symmetry |
CBCT |
| Razumova et al, 2018/ Russia20 | 510 MN
510 MN |
Central 99.4% 0.00% 0.6%
Lateral 99.2% 0.8% 0.0% |
High Symmetry | CBCT |
| Saati et al, 2018/Iran9 | 207 MN
86 MN 270 Image |
Central 54.5% 0.00% 34.2% 0.00% 11.3%
Lateral 56.5% 0.00% 26.1% 0.00% 17.4% 1 root with 1 canal, CI; 84.5% and LI; 78.2% |
NSD ↔Teeth Type
NSD ↔ Gender High symmetry |
CPCT |
| Martins et al, 2018, China and Portugal10 | 240 MX Asian
White 937 MX Asian White |
Central 99.6% 0.00% 0.4% 0.00% 0.0%
Central 72.6% 2.40% 0.8% 0.00% 0.3% VII; 0.5% Lateral 95.0% 2.90% 0.8% 0.00% 1.3% Lateral 70.1% 6.10% 23.1% 0.00% 0.2% VII; 0.3% |
SD ↔Ethnics
Moderate Symmetry |
CBCT
|
| Martínez et al, 2018/ Belgium
& Chile11 |
MN Belgium
Chile MN Belgium Chile |
Central 60.50% 0.58% 32.18% 0.00% 4.02% VII; 0.58%, X; 1.15%
Central 59.65% 0.58% 37.44% 0.00% 1.75% VII; 000% X; 0.58% Lateral 77.8% 2.92% 19.3% 0.00% 0.00% Lateral 79.12% 1.10% 19.8% 0.00% 0.00% |
SD ↔ Ethnics
Moderate Symmetry
345 Belgium / 353 Chile |
CBCT |
| Popovic et al, 2018/ Serbia12 | 296MN/Male
Female 294MN /Male Female 902 Teeth |
Central 68.7% 7.2% 22.0% 0.00% 1.2%
Central 78.5% 1.5% 20.0% 0.00% 0.00% Lateral 72.0% 4.7% 22.0% 0.00% 1.2% Lateral 75.4% 4.9% 13.8% 1.5% 3.1% Total 73.3%, 5.1% 20.0% 0.4%, 0.00% Others 1.4% |
NSD↔ Tooth Type
SD ↔ Gender Moderate symmetry |
CBCT |
| Shemesh et al, 2018/ Israel13 | MN Male
Female MN Male Female
|
Central 51.2%, 5.77% 39.15% 1.24% 0.62% 1.87%
Central 65.8% 2.65% 29.6% 0.5% 0.5% 0.85% Lateral 56.96% 5.51% 35.83% 0.46% 0.00% 1.53% Lateral 66.5% 3.39% 29.24% 0.46% 0.11% 0.23% Bilateral incidence more than 1 root canal in C; 69.8% & L 68.7% |
NSD↔ Tooth Type
SD↔ Genders Moderate symmetry
Male 653/ Females 855 |
CBCT |
| Verma et al, 2017/ India14 | 400 MN
400 MN 200 Image 800 Teeth |
Central 68.3% 11.0% 15.3% 1.8% 3.8% Males 15.2%
Lateral 65.0% 13.3% 5.3% 3.0% 3.5% Females 20.4% One root with one canal in 66.5% of Man Two canals 33.5% both right C & L, 30% for left C & 36.5% for left L |
SD ↔ Side
SD ↔ Gender Moderate Symmetry 103 Male /97Females |
CBCT |
| Zhengyan et al., 2016/ China15 | MN
MN 9646 Image |
Central 96.3% 0.2% 2.7% 0.1% 0.75% 3.8%
Lateral 89.4% 1.1% 7.7% 0.3% 0.70% IX; 0.3% 10.8% |
SD↔ Tooth Type&Side
SD ↔ Gender & Age Low Symmetry Males 923 / Female 802 |
CBCT |
| Arslan et al, 2015/ Turkey16 | 184 MN/Male
190MN/Female
374 Image 101 Patient |
Central 51.9% 4.3% 41.6% 0.00% 0.5% 1.6%
Central 52.9% 2.6% 42.3% 0.00% 1.6% 0.5% Lateral 37.2% 5.2% 55.2% 0.00% 1.7% 0.6% Lateral 65.3% 2.0% 30.7% 0.00% 0.5% 1.5% Males more complex canal configuration than females. |
SD ↔ Gender
Low Symmetry
54 Females &47 Males |
CBCT
|
| Altunsoy et al, 2014/ Turkey21 | MN / Male Female
MN/ Male Female 1582 Central 1603 Lateral |
Central 80.7% 0.6% 1.3% 4.2% 13.1%
Central 88.2 0.3% 0.3% 4.3% 7.0% Lateral 76.7% 1.6% 1.4% 5.9% 14.4% Lateral 83.7% 1.0% 0.6% 4.9% 9.8% ↑in males
|
SD ↔ Gender
Moderate Symmetry
410 Male /417 Female |
CBCT |
| Lin et al, 2014/ China30 | 706 MN
706 MN
353 Image |
Central 89.1 % 2.4 % 6.2% 1.7 % 0.6 %
Lateral 74.5 % 3.7 % 19.3% 2.1 % 0.4
Type III incisors were most prevalent, followed by types II, IV & V |
SD↔ Tooth Type
SD ↔ Gender High Symmetry Male 163 / Females 190 |
CBCT |
| Zhao et al., 2014/ China31 | 866 Patients
4 674 MN |
All Centrals and Laterals were with a single root. Central 6.7%
Type III canal most prevalent Lateral 7.4% Two root canals 9.8% in 31-40 years in Cs, & 21.5% (31-40 years) in Ls |
SD↔ Tooth type
SD ↔Age Groups Moderate Symmetry |
CBCT |
| Aminsobhani et al, 2013/ Iran32 | 632 MN
614 MN 400 Image |
Central 72.7% 11.3% 4.7% 7.7% 3.6% 27.3%
Lateral 70.6% 7.10% 3.7% 15.4% 3.2% 29.4% Root Length; MANC (21.3±0.10) MANL (21. 9± 0.13 mm). |
NSD ↔ Gender
High Symmetry Males 620/Females 626 |
CBCT |
| AlOudah&Awadeh, 2006 / Jordan33 | 450 Extracted Teeth | 73.8% 26.2%
8.7% had two separate apical foramina. |
In-Vitro, staining & tooth‐clearing | |
| Vertucci FJ, 1984/ USA22 | 100 MN
100 MN |
Central 70% 5% 22% 0.00% 3%
Lateral 75% 5% 18% 0.00% 2% |
Moderate Symmetry | In-Vitro Clearing method |
| Maxillary teeth | ||||
| Mashyakhy & Gambarini, 2019 / KSA, Jazan17 | 184 MX
200 MX |
Central 100%
Lateral 100%
|
NSD ↔ Gender
Very High Symmetry Male 52.1/Females 47.9 |
CBCT |
| Saini et al, 1990/ KSA, Riyadh18 | 1980 MX
1980 MX
|
Teeth with Shovel-shaped incisors were
Central Cs- Type I;0.90%, II; 3.73%, III; 3.25%, IV; 7.8% Lateral Ls- Type I; 1.96%, II; 6.81%, III; 1.21%, IV:10% Teeth with Type II Dens invaginatus; Centrals 4.48% Laterals 11.11% |
NS ↔ Genders
Measured Shovel-shaped incisors Dens – invaginatus |
Radiograph |
| Martins et al, 2018/ China & Portugal10 | 240 MX
937 MX |
Central Asian 100% and White 100%
Lateral Asian 100% and White 100% |
SD ↔Ethnics | CBCT |
| Pan et al, 2019/ Malaysia19 | 347 MX
362 MX 208 Image |
Central 94.9% 5.1%
Lateral 87.85 12.3% |
NSD ↔ Gender
NSD ↔ Side High Symmetry |
CBCT |
| Razumova et al, 2018/Russia20 | 510 MX
510 MX |
Central 100%
Lateral 100% |
High Symmetry | CBCT |
| Martins et al, 2017/Portugal35 | 827 MX
902 MX |
Central 100%
Lateral 100% |
Very High Symmetry | CBCT |
| de Silva et al, 2016/ Brazil36 | 200 MX
200 MX |
Central 98% 1.0% 0.00% 0.00% 1.0%
Lateral 96% 3.5% 0.00% 0.00% 0.5% |
Moderate Symmetry | CBCT |
| Altunsoy et al, 2014/ Turkey21 | MX Male
MX Female
|
Central 99.5% 0.00% 0.4% 0.00% 0.1% Male Higher
Lateral 99.7% 0.00% 0.00% 0.00% 0.3% Central 96.7% 1.3% 0.7% 0.00% 1.3% Female/Lesser Lateral 98.3% 0.7% 0.00% 0.5% 0.5% |
SD ↔ Gender
Moderate Symmetry
Male 410 /Females 417 |
CBCT |
| Weng et al, 2009/ China37 | 71 MX
70 MX |
Central 95.8% 4.2% 0.00% 0.00% 0.00%
Lateral 91.4% 2.9% 1.40% 0.00% 4.3% |
Moderate Symmetry | Clearing method with dye |
| Caliskan et al, 1995/ Turkey38 | 100 MX
100 MX |
Central 100%
Lateral 78.05% 2.44% 14.63% 0.00% 4.88% |
Moderate Symmetry | Clearing technique |
| Vertucci FJ, 1984/ USA22 | 100 MX
100 MX |
Central 100%
Lateral 100% 24 lateral canals in MAXC; 1% cervical, 6% medial, 93% apical |
Very High Symmetry | In-Vitro Clearing |
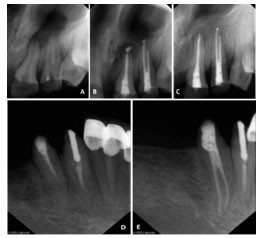
Case Reports: Twenty-nine clinical case reports are listed in Table 2: 25 cases involving maxillary teeth and four cases including mandibular teeth. Among these, three cases were related to Saudi patients (Al-Nazhan S., 1991; Alenazy et al., 2019; Al-Madi EM., 2020). Most of the maxillary case reports were central incisors teeth ‘’21 of 25 in the maxilla’’; nine cases were males and 14 females; and 14 cases were on the left side. Most canals were Vertucci’s classification Type IV in both arches, and most of the teeth had two roots. Relatively few cases relating to the mandibular arch have been published. The following information’s were gathered: the author(s) name, time of publication of the case report, place of documentations, gender, type and side of involved tooth/teeth, number of canals, roots or canal configuration according to Vertucci’s classification, and special finding associated with the treated case, if any. Figure 1 shows a radiograph of a treated case for male on the left lateral incisor maxillary tooth and other mandibular case for a female patient on the left central incisor tooth.
Table 2. Summary of previous case reports of Maxillary and Mandibular central and lateral incisors with variations as gender, tooth type, side, and canal morphology according to Vertucci’s Classification
| Maxillary Teeth | |||||||
| Author (s) & Year Publication | Country | Gender | Tooth type | Vertucci’s Classification | Canal (s) | Root (s) | Special findings |
| Present Case | Figure 1 (A-C) | Male | Lateral, left | V | 1 | 2 | Non – Vital |
| Al-Madi et al, 202039 | Saudi Arabia | Female | Central, left | IV | 2 | 2 | Re-treatment |
| Al-Nazhan S, 199140 | Saudi Arabia | Female | Central, left | IV | 2 | 2 | Enamel Hypoplasia |
| Buonvivere & Buonvivere, 201942 | Italy | Female | Lateral, left | VIII | 1 | 3 | Non-vital |
| Elbay et al, 201643 | Turkey | Female | Central, right
Lateral, right |
IV
IV |
2
2 |
2
2 |
Non-vital |
| Sharma et al, 201444 | India | Male | Central, right | V | 1 | 2 | Crown dilaceration |
| Krishnamurti et al,201245 | India | Female | Central, right | ———– | 2 | 1 | Root resorption |
| Kottoor & Murugesan, 201246 | India | Male | Lateral, left | ——- | 1 | 4 | Non-vital |
| Nabavizadeh et al,201047 | Iran | Male | Central, left | IV | 2 | 2 | Non-vital |
| Gondim et al, 200948 | Brazil | Male | Central, right | 2 | 3 | ——— | |
| Shokouhinejad et al, 200949 | Iran | Female | Central, left
Lateral, left |
V
V |
1
1 |
2
2 |
Non-vital |
| Rodrigues & Silva, 200950 | Brazil | Female | Central, right | IV | 2 | 2 | Non-vital |
| Sheikh-Nezami MM, 200751 | Iran | Male | Central, right | 1 | 3 | Non-vital | |
| Sponchiado et al, 200652 | Brazil | Female | Central, left | IV | 2 | 2 | ——— |
| Lin et al, 200653 | China | Female | Central, right | IV | 2 | 2 | ————- |
| Benenati FW, 200654 | ——– | —— | Central, left | IV | 2 | 2 | Non-vital |
| Khojastehpour & Khaya, 200555 | Iran | Female | Central, left | IV | 2 | 2 | Non-vital |
| Zaitoun &Mackie, 200456] | United Kingdom | Female | Central, right | VIII | 1 | 3 | Non-vital |
| Genovese & Marsico,200357 | Italy | Female | Central, right | IV | 2 | 2 | Non-vital |
| Cimilli & Kartal, 200258 | Turkey | Male | Central, left | IV | 2 | 2 | Fusion of roots |
| Cabo-Valle & Gonzalez-Gonzalez, 200159 | Spain | Female | Central, right | IV | 2 | 2 | Non-vital |
| Mangani & Ruddle, 199460 | Italy | Female | Central, right | 1 | 4 | Dens invaginatus | |
| Lambruschini & Camps, 199361 | France | Male | Central, right | IV | 2 | 2 | ——– |
| Hososmi et al, 198962 | Japan | Male | Central, right | 2 | 3 | Gemination | |
| Mader & Konzelman, 198063 | United States America | Male | Central, left | IV | 2 | 2 | —– |
| Sinai & Lustbader, 198064 | United States America | ——– | Central, right | IV | 2 | 2 | Incomplete apical formation |
| Mandibular Teeth | |||||||
| Present Case | Figure 1 (D-E) | Female | Central, left | V | 2 | 1 | Re-treatment |
| Al Enazay et al., 201941 | Saudi Arabia
|
Female | Central, left
Lateral, left Central, right Lateral, right |
V
III III IV |
1
1 1 2 |
2
1 1 2 |
Re-treatment |
| Hwang & Min, 200565 | South Korea | ——- | Central, right
Central, left Lateral, left |
IV
IV IV |
2
2 2 |
2
2 2 |
Re-treatments |
| Kabak & Abbott, 200766 | Belarusia | Male | Central, right
Lateral, right Lateral, left |
II
II V |
2
2 1 |
2
2 2 |
Non -vital |
| Guan et al., 200967 | China | ——– | Central, left
Lateral, left Central, right Lateral, right |
IV
IV IV IV |
2
2 2 2 |
2
2 2 2 |
———- |
Figure 1: Maxillary left lateral incisor with preapical pathosis (A), teeth after RCT for lateral with two canals (B), follow-up after
18 months (c). Mandibular left lateral incisor with incomplete RCT (D), tooth after RCT with two root canals (E).
DISCUSSION
Knowledge of tooth morphology is main basis for science of RCT. Today, root apex is not the only area in RCT science but the idea of three-dimensional RC filling implies that although working length and maintaining it is more important, access to all complications of canal inside is also crucial in order to RC filling (Castelucci., 2015; Bansal et al., 2018). Worldwide, the maxillary and mandibular central and lateral incisors are among the most likely teeth to require RCT (Castelucci., 2015; Filpo–Perez et al., 2015; Ahmed and Hashem., 2016; Martinsa et al., 2020; Baruwa et al., 2020).
Usually, there is just one canal in the anteriors incisors (Vertucci., 1984; Altunsoy et al., 2014; Razumova et al., 2018; Mashyakhy and Gambarini., 2019; Pan et al., 2019). However, a second canal or other variations do occur (Al‑Quadah and Awawdeh., 2006; Aminsobhani et al., 2013; Arslan et al., 2015; Zhengyan et al., 2016; Verma et al., 2017; Saati et al., 2018; Martins et al., 2018; Martínez et al., 2018; Popovic et al., 2018; Shemesh et al., 2018; Ghabbani et al., 2020). Anteriors incisors are the smallest human permanent teeth; incisors have complex roots and canals, especially mandibular incisors. Incisors can be single-rooted, have double roots or canals, a lateral branch of a root canal, apical ramification, or apical furcation; this variability can complicate RCT (Hwang and Min., 2005; Kabak and Abbott., 2007; Guan et al., 2009; Elbay et al., 2016; Alenazy et al., 2019; Buonvivere & Buonvivere., 2019).
Here we review local and international studies and describe the numbers of canals and root morphology of maxillary and mandibular anterior teeth.Starting in the 20th century, the outside and inner structure of the maxillary and mandibular anterior teeth have been evaluated using in vivo and in vitro techniques. The in vivo techniques include clinical evaluation during RCT, retrospective assessment of patients’ files, and radiographic analysis using conventional and advanced radiographic methods, such as CBCT. The in vitro techniques include root sectioning, canal staining, tooth clearing, microscopic and radiographic examinations using traditional or conventional x-rays, and 3-D techniques, such as micro-computed to be as high as 70% (Al‑Fouzan et al., 2012; Mashyakhy., 2019),and similar rates have been reported in the US, Turkey, Iran, Portugal, and Germany, (Vertucci., 1984; Altunsoy et al., 2014; Mirhosseini et al., 2017; Martins et al., 2018; Baxter et al., 2020). The frequency of Vertucci’s Type III in mandibular lateral incisors was recorded as 20–30% in Saudi studies by Al‑Fouzan et al., 2012; Mashyakhy., 2019; Ghabbani et al., 2020; and similar findings were reported by (Satti et al., 2018) in Iran, (Martins et al., 2018) among patients from China and Portugal, and Turkish patients by (Arslan et al., 2015), and less than 20% amongst patients from Iran, Belgium & Chile, and Germany (Mirhosseini et al., 2017; Martínez et al., 2018; Baxter et al., 2020).
Local studies in Saudi Arabia have reported that around 30% of mandibular teeth had two canals (Al‑Fouzan et al., 2012; Mashyakhy., 2019; Ghabbani et al., 2020). This is well supported by Ahmed et al., 2015. who reported that the two-canal configuration is the most common accessory anatomical variation in single-rooted mandibular anteriors (Ahmed and Hashem., 2016). This is in line with other studies conducted in, Iran, India, Serbia, and Germany (Mirhosseini et al., 2017; Verma et al., 2017; Popovic et al., 2018; Baxter et al., 2020) but a higher percentage was detected in Turkey, Israel, and Italy (Arslan et al., 2015; Shemesh et al., 2018; Valenti-Obino et al., 2019). Also, two canals were more common amongst females than males (Verma et al., 2017), but this trend was reversed in a Turkish population (Altunsoy et al., 2014). Finally, mandibular lateral incisors with two canals were more than central incisors among a Chinese population (Zhao et al., 2014). Vertucci’s classification Type IV was the least common in all studies, and Type V was present in small percentages within the screened patients in most of the studies (Table 1).
The root canal morphology can change over time. Changes due to normal physiological aging usually occur because of secondary dentine deposition (Johnstone and Parashos., 2015). A recent study has reported high variability in root canal morphology of mandibular anterior incisors. Vertucci’s classification Type VII was detected in a local study conducted in Al Madinah Al Munawara (Ghabbani et al., 2020). Also, a similar canal Type was reported in those studies that included participants from Turkey, China, Portugal, Belgium, Chile, and Israel (Arslan et al., 2015, Martins et al., 2018; Martínez et al., 2018; Shemesh et al., 2018;). Other variations were shown in the form of Types IX and X in China and Belgium (0.58–1.15%, respectively), and in China alone (10.8%) (Weng et al., 2009; Bourzgui and Akarslan., 2020).
Compared to the mandibular arch, relatively few studies have addressed maxillary anteriors (Vertucci., 1984; Caliskan et al., 1995; Weng et al., 2009; Altunsoy et al., 2014; da Silva et al., 2016; Martins et al., 2017; Razumova et al., 2018; Mashyakhy and Gambarini., 2019; Pan et al., 2019; Bourzgui and Akarslan., 2020). Both central and lateral maxillary teeth typically start with a single canal and end in a single root. Rates of up to 100% Vertucci’s Classification Type I have been reported, including in a single local Saudi study (Mashyakhy and Gambarini., 2019), and studies carried out in Russia, America, China, Portugal, and Turkey (Vertucci., 1984; Caliskan et al., 1995; Martins et al., 2017; Razumova et al., 2018; Bourzgui and Akarslan., 2020), but lower rates have been reported amongst central maxillary teeth in studies conducted in China, Brazil, and Malaysia (Weng et al., 2009; da Silva et al., 2016; Pan et al., 2019). On the other hand, a rate of 78–91%; Weng et al., 2009 was recorded for maxillary lateral incisors in Turkey, China, and Malaysia (Caliskan et al., 1995; Pan et al., 2019;). Few studies reported a moderate percentage of two canals in maxillary anteriors or incisors, with lower rates than in mandibular teeth. Vertucci’s classification Type III and IV were relatively rare. In a study conducted by Altunosy et al., 2014 among a Turkish population, the authors reported that two canals were more common in males than females; another study reported significant differences in canal number and configuration when comparing populations from China and Portugal (Bourzgui and Akarslan., 2020).
In this review, we conducted a gender comparison in relation to the number of canals, the number of root canals, and root canal configurations (according to Vertucci’s classification). Both studies among Jazanian publications showed no significant differences between gender (Mashyakhy., 2019; Mashyakhy and Gambarini., 2019), while a study conducted in Al Madinah Al Munawara by Ghabbani et al., 2020 showed a significant difference between genders. This could be explained by the uniform sample of the population in Jazan, and mixed populations in the study conducted by Ghabbani et al., 2020 and both studies conducted in Turkey by Altunsoy et al., 2014 and Arslan et al., 2015, while no significant differences were recorded in Malaysia in both arches Pan et al., 2019, or both Iranian studies by Aminsobhani et al., 2013; Saati et al., 2018).
The bilateral symmetry between sides in relation to the type of teeth and canals configurations as well as root numbers, Al-Fouzan et al., 2012 reported a high or typical symmetry between the extracted mandibular teeth in relation to the number of canals and canal configurations. This is consistent with studies conducted in Europe ‘Italy and Germany’’ (Valenti-Obino et al., 2019; Baxter et al., 2020), Asia ‘’China and Iran’’ (Lin et al., 2014; Saati et al., 2018), and the US (Vertucci., 1984), which have also reported high symmetry, which might be related to the racial type and uniform sample types. Mashyakhy M., 2019, Mashyakhy and Gambrini., 2019 reported moderate bilateral asymmetries in central and lateral maxillary and mandibular incisors in relation to some canals and canals configurations. This finding is similar to those from other countries, such as studies conducted in India, China, Portugal, Belgium, Serbia, and Israel (Verma et al., 2017; Martins et al., 2018; Martínez et al., 2018; Popovic et al., 2018; Shemesh et al., 2018). anteriors (Ahmed and Hashem., 2016). Due to the wide morphological variance of the root and root canal system in human anterior teeth, dental general practitioners and specialists should be aware of such anatomical variations, thereby decreasing the risk of failure because of inadequate debridement of inaccessible or undetected parts of the RCS. Recently developed diagnostic devices, the latest endodontic (and periodontal) techniques, and improvements in RCT biomaterials and machines are likely to improve RCT outcomes for patients (Ahmed and Hashem., 2016).
CONCLUSION
From this review the concluding remarks can be drown; The Saudi data and data gathered internationally in relation to canal number, root canal configuration was largely consistent. Type I Vertucci’s classification of canal configuration is the most common type in both arches, followed by Type III. Variations are frequent in the mandibular teeth. Other types of Vertucci’s classification were present in all populations, but at lower rates. The bilateral symmetry of canal and root numbers and configuration vary across populations and genders. All reported cases describing maxillary teeth included only a single tooth, while most of the cases involving mandibular anterior teeth described an unusual canal configuration or root canal number. Dentists should be familiar with the variations in canal numbers and configuration. Also, dentists should know how to use at least read the output of new technologies for visualizing root canal systems.
Conflicts of interest: The authors declare that there are no conflicts of interests.
Funding: We did not receive any fund for this project.
Ethical approval: Ethical approval was obtained from College of Dentistry, Jazan University, # CODJU-2007F date Septamber 15/ 2020.
REFERENCES
Ahmad IA (2015). Root and root canal morphology of Saudi Arabian permanent dentition. Saudi Endod J; 5: 99-106.
Ahmed HMA, Hashem AA (2016). Accessory roots and root canals in human anterior teeth: a review and clinical considerations. Inter Endo J; 49: 724–736.
Alenazy MS, Alrushoud SS, Almasoud A, Al-Dayel O (2019). Endodontic management of mandibular anterior teeth with two root canals. Saudi Endod J; 9: 140-
Al‑Fouzan KS, Al‑Manee A, Jan J, Al‑Rejaie M (2012). Incidence of two canals in extracted mandibular incisors teeth of Saudi Arabian samples. Saudi Endod J; 2: 65‑9.
Al-Madi EM. Maxillary Central Incisor with Two Roots (2020): A Case Report. Saudi Endo J; 10(2): 162-4.
Al-Nazhan S (1991). Two root canals in a maxillary central incisor with enamel hypoplasia. J Endod; 17(9): 469-71.
Altunsoy M, Ok E, Nur BG, Aglarci OS, Gungor E, Colak M (2014). A cone-beam computed tomography study of the root canal morphology of anterior teeth in a Turkish population. Eur J Dent; 8: 302-6.
Al‑Quadah AA, Awawdeh LA (2006). Root canal morphology of mandibular incisors in a Jordanian population. Int Endod J; 39: 8-12.
Aminsobhani M, Sadegh M, Meraji N, Razmi H, Kharazifard MJ (2013). Evaluation of the Root and Canal Morphology of Mandibular Permanent Anterior Teeth in an Iranian Population by Cone-Beam Computed Tomography. J Dent Tehran Univ Medi Scie; 10(4): 358-66.
Arslan H, Ertas H, Ertas ET, Kalabahk F, Saygih G, Capar ID (2015). Evaluating root canal configuration of mandibular incisors with cone-beam computed tomography in a Turkish population. J Dent Scie; 10: 359-36.
Bansal R, Hegde S, Astekar MS (2018). Classification of Root Canal Configurations: A Review and a New Proposal of Nomenclature System for Root Canal Configuration. J Clin Diag Rese;12(5): ZE01-ZE05.
Baruwa AO, Martins JNR, MeirinhosJ, Pereira P, et al (2020). The Influence of Missed Canals on the Prevalence of Periapical Lesions in Endodontically Treated Teeth: A Cross-sectional Study. J Endod; 46(1): 34-39.e1. doi: 10.1016/j.joen.2019.10.007.
Baxter S, Jablonski M, Hülsmann M (2020). Cone-beam-computed-tomography of the symmetry of root canal anatomy in mandibular incisors. J Oral Science; 62(2): 180-3.
Benenati FW (2006). Endodontic treatment of a maxillary central incisor with two separate roots: case report. Gen Dent; 54(4): 265-6.
Bourzgui F, Akarslan Z (2020). Extremal, and internal anatomy of mandibular permanent incisors. Human Teeth, Key Skills and Clinical Illustration, 1st ED, pp 845. DOI:10.5772/intechopen.81278, ISBN: 978-1-78923-840-2
Buonvivere M, Buonvivere M (2019). Maxillary Lateral Incisor with 3 Root Canals: A Case Report. J Adva Oral Research; 10 (2); 179-182.
Cabo-Valle M, Gonzalez-Gonzalez JM (2001). Maxillary central incisor with two root canals: an unusual presentation. J Oral Rehabil; 28(8): 797-8.
Caliskan MK, Pehlivan Y, Sepet~io~llu F, T~irk~in M, Tuncer S (1995). Root Canal Morphology of Human Permanent Teeth in a Turkish Population. J Endo; 21(4): 324-29
Castellucci A. Endodontics (2015); Access Cavity And Endodontic Anatomy. Volum I, Il Tridente Edizioni Odontoiatriche, Chapter 11, pp 244-329.
Cimilli H, Kartal N (2002). Endodontic treatment of unusual central incisors. J Endod; 28(6):480-1.
da Silva EJ, de Castro RW, Nejaim Y, et al (2016). Evaluation of root canal configuration of maxillary and mandibular anterior teeth using cone beam computed tomography: an in-vivo study. Quintessence Int; 47: 19–24.
Elbay M, Kaya E, Elbay ÜŞ, Sarıdağ S, Sinanoğlu A (2016). Management of two-rooted maxillary central and lateral incisors: A case report with a multidisciplinary approach involving CAD/CAM and CBCT technology. J Pediatr Dent; 4: 51-4.
Filpo–Perez C, Bramante CM, Villas-Boas MH, Duarte MAH, Versiani MA, Ordinola-Zapata R (20150. Micro-computed tomographic analysis of the root canal morphology of the distal root of mandibular first molars. J Endod; 41: 231- 36.
Genovese FR, Marsico EM (2003). Maxillary central incisor with two roots: a case report. J Endod; 29(3): 220-1.
Ghabbani HM, Marghalani AA, Alabiri HR (2020). Assessment of root canal morphology of mandibular incisors using cone beam computed tomography among residents of Al-Madinah Al-Munawara Region, Saudi Arabia. Eur J Gen Dent; 9: 40-4
Gondim E Jr SF, Zingg P, Karabucak B (2009). A maxillary central incisor with three root canals: a case report. J Endod; 35(10): 1445-7.
Grover C, Shetty N. Methods to study root canal morphology (2012): A review. ENDO (Lond Engl); 6:171‑82.
Guan QL, Yu XF, Deng J (2009). Double root canal of all mandibular incisors: report of one case and review of the literature. Shanghai Kou Qiang Yi Xue; 18(6): 669-72.
Hosomi T, Yoshikawa M, Yaoi M, Sakiyama Y, Toda T (1989). A maxillary central incisor having two root canals geminated with a supernumerary tooth. J Endod; 15(4): 161-3.
Hwang YH, Min KS (2005). Clinical Management of 3 Mandibular Incisors with 2 Separate Canals and Foramina: Case Report. J Can Dent Assoc; 71(6): 388–93.
Johnstone M, Parashos P (2015). Endodontics and the ageing patient. Australian Endo J; 60: 20-27.
Kabak YS, Abbott PV (2007). Endodontic treatment of mandibular incisors with two root canals: Report of two cases. Aust Endod J; 33: 27–31
Khojastehpour L, Khayat A (2005). Maxillary central incisor with two roots: A case report. J Dent; 2(2): 74-7.
Kottoor J, Murugesan R, Albuquerque DV (2012). A maxillary lateral incisor with four root canals. Int Endod J; 45: 393‑7.
Krishnamurti A, Velmurugan N, Nandin S (2012). Management of single-rooted maxillary central incisor with two canals: A case report. Iran Endo J; 7(1): 36-39.
Lambruschini GM, Camps J (1993). A two-rooted maxillary central incisor with a normal clinical crown. J Endod; 19(2): 95-6.
Lin WC, Yang SF, Pai SF (2006). Nonsurgical endodontic treatment of a two-rooted maxillary central incisor. J Endod; 32(5): 478-81.
Lin Z, Hu Q, Wang T, Ge J, Liu S, Zhu M, Wen S (2014). Use of CBCT to investigate the root canal morphology of mandibular incisors. Surg Radiol Anat; 36(9): 877-82.
Mader CL, Konzelman KJ (1980). Double-rooted maxillary central incisors. Oral Surg Oral Med Oral Pathol Oral Radiol Endod; 50: 99-101.
Mangani F, Ruddle CJ (1994). Endodontic Treatment of a “Very Particular” Maxillary Central Incisor. J Endod; 20(11): 560-1.
Martínez I, Torres A, Jacobs R, Lepe A, Jara D, Ramírez V, et al (2018). Root Canal Morphology of Mandibular Incisors Using Cone-Beam Computed Tomography in Two Population Samples: A Cross-Sectional Study. Austin J Radiol; 5(2): 1083-11.
Martins JH, Marques D, Silva EG, Carames K, et al (2019). Prevalence Studies on Root Canal Anatomy Using Cone-beam Computed Tomographic Imaging: A Systematic Review. J Endod; 45(4):372-386.
Martins JNR, Gu Y, Marques D, Francisco H, Carames J (2018). Differences on the Root and Root Canal Morphologies between Asian and White Ethnic Groups Analyzed by Cone-beam Computed Tomography. JOE; 44(7):1096–1104
Martins JNR, Marques D, Mata A, Carames J (2017). Root and root canal morphology of the permanent dentition in a Caucasian population: a cone-beam computed tomography study. Inter Endo J; 50: 1013–26.
Martins JNR, Marques D, Silvae EJN, Caramêsc J et al (2020). Influence of Demographic Factors on the Prevalence of a Second Root Canal in Mandibular Anterior Teeth – A Systematic Review and Meta-Analysis of Cross-Sectional Studies Using Cone Beam Computed Tomography. Archives of Oral Biology; 116: 104749.
Mashyakhy M (2019). Anatomical analysis of permanent mandibular incisors in a Saudi Arabian population: An in Vivo cone-beam computed tomography study. Niger J Clin Prac; 22: 1611-6.
Mashyakhy M, Gambarini G (2019). Root and Root Canal Morphology Differences Between Genders: A Comprehensive in-vivo CBCT Study in a Saudi Population. Acta stomatol Croat; 53(3):231-246.
Mirhosseini F, Tabrizizadeh M, Nateghi N., Shafiei Rad E., Derafshi A., Ahmadi B., Daneshvar M (2019). Evaluation of Root Canal Anatomy in Mandibular Incisors Using CBCT Imaging Technique in an Iranian Population. J Dent Shiraz Univ Med Sci; 20(1): 24-29.
Neelakantan P, Subbarao C, Subbarao CV (2010). Comparative evaluation of modified canal staining and clearing technique, cone-beam computed tomography, peripheral quantitative computed tomography, spiral computed tomography and plain and contrast medium-enhanced digital radiography in studying root canal morphology. J Endod; 36: 1547–51.
Nabavizadeh MR, Jouyandeh MR, Atbaee A, Shams MS (2010). Nonsurgical Endodontic Treatment of a Maxillary Central Incisor with Two Separate Roots: A Case Report. IEJ; 5(3): 212-5
Pan JYY, Parolia A, Chuah SR, Bhatia S, Mutalik S, Pau A (2019). Root canal morphology of permanent teeth in a Malaysian subpopulation using conebeam computed tomography. BMC Oral Health; 19: 14-29.
Popovic M, Papic M, Zivanovic S, Acovic A, et al (2018). Cone-Beam Computed Tomography Study Of The Root Canal Morphology Of Mandibular Anterior Teeth In Serbian Population. Ser J Exp Clin Res; 17(1): 27-34.
Przesmycka A, Tomczyk J (2016). Differentiation of root canal morphology – a review of the literature. Anthropological Review 2016; 79(3): 221–239.
Razumova S, Brago A, Khaskhanova L, Howijieh A, Barakat H, Manvelyan A (2018). A Cone-Beam Computed Tomography Scanning of the Root Canal System of Permanent Teeth among the Moscow Population. Inter J Dent, Article ID 2615746, 6 pages https://doi.org/10.1155/2018/2615746
Rodrigues EA, Silva SJ (2009). A Case of Unusual Anatomy: Maxillary Central Incisor with Two Root Canals: Case Report. Int J Morphol; 27: 827‑30.
Saati S, Shokri A, Foroozandeh M, Poorolajal J, Mosleh N (2018). Root Morphology and Number of Canals in Mandibular Central and Lateral Incisors Using Cone Beam Computed Tomography. Braz Dent J; 29(3): 239-244.
Saini TS, Kharat DU, Mokeem S (1990). Prevalence of shovel‑shaped incisors in Saudi Arabian dental patients. Oral Surg Oral Med Oral Pathol; 70: 540‑4.
Sharma s, Grover s, Sharma V, Srivastava D, Mittal M (2014). Endodontic and Esthetic Management of a Dilacerated Maxillary Central Incisor Having Two Root Canals Using Cone Beam Computed Tomography as a Diagnostic Aid. Case Rep Dent; doi: 10.1155/2014/8619422014, Article ID 861942, 7 pages.
Sheikh-Nezami M MN (2007). Endodontic treatment of a maxillary central incisor with three root canals. J Oral Sci; 49(3): 254-7.
Shemesh A, Kavalerchik E, Levin A, Ben Itzhak J, Levinson O, Lvovsky A, Solomonov M (2018). Root Canal Morphology Evaluation of Central and Lateral Mandibular Incisors Using Cone-beam Computed Tomography in an Israeli Population. J Endod; 44(1): 51-55.
Shokouhinejad N, Sheykhrezaee MS, Assadian H (2009). Endodontic treatment of two-canalled maxillary central and lateral incisors: a case report. IEJ: 4(2): 213-7
Sinal IH, Lustbader S (1984). A dual-rooted maxillary central incisor. J Endod; 10(3): 105-6.
Sponchiado EC, Jr., Ismail HA, Braga MR, de Carvalho FK, Simoes CA (2006). Maxillary central incisor with two root canals: a case report. J Endod; 32(10): 1002-4.
Valenti-Obino F, Di Nardo D, Quero L, Miccoli G, et al (2019). Symmetry of root and root canal morphology of mandibular incisors: A cone-beam computed tomography study in vivo. J Clin Exp Dent; 11(6): e527-33.
Verma GR, Bhadage C, Bhoosreddy RR, Vedpathak PR, Mehrotra GP, Nerkar AC, Bhandari A, Chaubey S (2017). Cone Beam Computed Tomography Study of Root Canal Morphology of Permanent Mandibular Incisors in Indian Subpopulation. Pol J Radiol; 82: 371-37.
Vertucci FJ (1984). Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol; 58: 589‑99.
Weng XY, Yu SB, Zhao SL, Wang HG, Mu T, Tang RY, Zhou XD (2009). Root Canal Morphology of Permanent Maxillary Teeth in the Han Nationality in Chinese Guanzhong Area: A New Modified Root Canal Staining Technique. JOE; 35(5): 432-38.
Zaitoun H, Mackie IC (2004). Management of a non‑vital central incisor tooth with three root canals. Dent Update; 31: 142‑4.
Zhao Y, Dong YT, Wang XY, Wang ZH, Li G, Liu MQ, Fu KY (2014). Cone-beam computed tomography analysis of root canal configuration of 4674 mandibular anterior teeth. Beijing Da Xue Xue Bao Yi Xue Ban; 46(1): 95-9.
Zhengyan Y, Keke L, Fei W, Yueheng L, Zhi Z (2016). Cone‑beam computed tomography study of the root and canal morphology of mandibular permanent anterior teeth in a Chongqing population. Ther Clin Risk Manag; 12: 19-25.

