Ebtesam A. Elsayed*1,2![]() , Hessa A. Almutairi3, Fahad M. Matashish4 and Hanan A. Abuhaimid3
, Hessa A. Almutairi3, Fahad M. Matashish4 and Hanan A. Abuhaimid3
1Community Health Nursing Department, Faculty of Nursing, Ain Shams University, Egypt.
2Public Health Department, College of Health Sciences, Saudi Electronic University, Saudi Arabia
3Msn., RN., Nursing Administration- General Directorate of Health Affairs- Riyadh.
4Msn., RN., Nursing Education Department, King Salman Hospital- Riyadh
Corresponding author email: e.elsayed@seu.edu.sa
Article Publishing History
Received: 19/04/2020
Accepted After Revision: 14/06/2020
Patient safety is an essential component of healthcare quality. It is clear that there is a need to analyze patient safety issues primary healthcare centers (PHCC) as an important part of the healthcare system, since most of the research that deals with patient safety issues in Saudi Arabia have been applied in hospitals rather than primary healthcare centers. The aim of this study is to assess the attitude of nurses regarding patient safety in Riyadh PHCCs of Saudi Arabia. A descriptive cross-section design was used. A sample of 314 nurses working in primary healthcare centers in Riyadh were participated in the study. A self-administered questionnaire was used for data collection which consisted of two parts covered socio-demographic data and nurses’ attitude regarding patients’ safety using the Safety Attitudes Questionnaire (SAQ). The study showed that the mean age of the participants was 34.3. The participants had a positive attitude regarding teamwork climate, job satisfaction, and safety climate dimensions with weighted mean 3.64, 3.78, and 3.61 respectively while they had a negative attitude regarding perceptions of management, working conditions, and stress recognition dimensions with weighted mean 3.19, 3.12, and 2.41 respectively. The study concluded that nurses working in PHCCs of Riyadh city had a negative attitude regarding patient safety with a statistically significant difference between nurses’ attitude and their years of experience and gender while there was no statistically significant difference between nurses’ attitude and age, educational qualification, and staff position.
Attitude; Nurses; Patient Safety; Primary Healthcare Center; Saudi Arabia
Elsayed E. A, Almutairi H. A, Matashish F. M, Abuhaimid H. A. Nurses’ Attitude Regarding Patient Safety in Primary Healthcare Centers of Saudi Arabia: A Cross-Sectional Study. Biosc.Biotech.Res.Comm. 2020;13(2).
Elsayed E. A, Almutairi H. A, Matashish F. M, Abuhaimid H. A. Nurses’ Attitude Regarding Patient Safety in Primary Healthcare Centers of Saudi Arabia: A Cross-Sectional Study. Biosc.Biotech.Res.Comm. 2020;13(2). Available from: https://bit.ly/2WIbv3z
Copyright © Elsayed et al., This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-BY) https://creativecommns.org/licenses/by/4.0/, which permits unrestricted use distribution and reproduction in any medium, provide the original author and source are credited.
INTRODUCTION
Patient safety is considered a global health concern which affecting patients whether in developed or developing countries, World health organization (WHO, 2016) has recognized the importance of patient safety and focused on as a public health concern. The simplest definition of patient safety as mentioned by (WHO, 2018) is “the prevention of errors and adverse effects to patients associated with healthcare”. According to the Saudi Patient Safety Taxonomy (S-PST), which is developed by Ministry of Health (MOH) to unify the conceptual framework related to patient safety in Saudi Arabia, has defined patient safety as “Freedom from accidental or preventable injuries produced by medical care” (MOH, 2017). The patient safety culture is the product of values, attitudes, skills, and standards of individuals and collective behaviors that determine the commitment, style, and proficiency of the administration of a safe organization (Fermo, et al., 2016). Thereby, a fulfilling culture of patient safety requires a grasp of these values and beliefs regarding what is important in an organization and which behavior and attitudes related to patient safety are supported and expected (Brasaite, et al., 2016).
Patient safety is the keystone of high-quality healthcare provided in all healthcare settings, and primary healthcare center is one of these settings which plays an important role in the healthcare system, as it is the first level of contact that individuals, families, and communities have with the healthcare system (Almalki, et al., 2011). So improving patient safety issues in primary healthcare centers (PHCCs) requires a new approach and thinking that including a greater emphasis on safety and prevention from harm. Because severe and complicated cases are treated in hospitals, most of the healthcare providers and the community underestimate the weight of primary healthcare services. This underestimation leads to errors in some fields as physician notification, communication, and staffing (Brotons, et al., 2012), add to that the most researches and activities concerned with patient safety issues are directed to hospitals, although it is well known that the majority of patients are examined first in primary healthcare centers by family doctors before they referred to hospitals (Webair, et al., 2015).
Community health nurse play a main role in maintaining and promoting patient safety in PHCCs, it not only just a part of what they do but it also committed through nurses’ code of ethics to provide “safe, competent and ethical care” (Canadian Nurses Association, 2002). Patient safety is fundamental part of nursing care, nurses play a significant role in improving patient safety alongside with the roles of inter-professional teams, health-care organizations and the health-care system (Canadian Nurses Association, 2019).
It is important that community health nurse working in PHCCs should be more knowledgeable about patient safety issues in order to minimize the incidence of adverse events that may lead to serious disabilities to the patients (Ghobashi, et al., 2014). Therefore, to ensure patient safety in PHCCs, it is essential to promote and improve safety attitudes among healthcare professionals especially nurses (Geevarghese, 2012). Patient safety research in PHCCs gives out that millions of people around the world are suffering from disabilities, injuries, or death due to unsafe medical practices, and there has been little research on patient safety published from Gulf Cooperation Council (GCC) countries regarding patient safety in PHCCs (Al Lawati et al., 2019).
More researches are needed to know about patient safety in PHCCs.It is important to mention that the data published by WHO showed that patient harm was the 14th leading cause of the global disease burden, comparable to diseases such as tuberculosis and malaria (WHO, 2018). Recent literature reviews have revealed that as many as four out of 10 patients are harmed while receiving healthcare in PHCCs, with up to 80% of the harm considered to have been preventable. The most detrimental errors are related to diagnosis, prescription and the use of medicines (WHO, 2019).
Administrative errors, those associated with the systems and processes of delivering care, were the most frequently reported type of errors in PHCCs (WHO, 2018). In the WHO Eastern Mediterranean Region, available data showed that healthcare-related harmful incidents affect 8 in 100 patients, and 4 out of 5 incidents were preventable (WHO, 2016).
In Saudi Arabia; patient safety is considered as a top priority for the healthcare services provided by the Ministry of Health (MOH), which has been obvious in the quality improvement projects and initiatives carried out through MOH facilities (MOH, 2017). The aim of this study was to analyze the attitude of nurses regarding patient safety in PHCCs of Saudi Arabia.
Research questions
The following research questions guided the study:
What is the attitude of nurses regarding patient safety in PHCCs of Riyadh city in Saudi Arabia?
Is there a statistical significant differences between nurses’ attitude and their age, gender, qualification, years of experience and staff position?
MATERIAL AND METHODS
In this study a descriptive cross-sectional design was used, the data collection was carried out from the last of November 2018 until May 2019 after permission letter No. 1440-544543 was obtained from the Ministry of Health to the managers of the primary healthcare centers in order to facilitate collecting the data. For data collection; an online self-administered structured questionnaire was used; all items of the questionnaire were obligatory to answer so no data are missed. The pilot study was carried out on 10% of the study sample in order to assess validity and reliability, detect any ambiguity in the tools, clarity of the items, as well as, to determine the time consumed for data collection. Necessary modifications were carried out and the final form was developed, the reliability of the study tool measured using Cronbach’s alpha; it was 0.896 for the 35 items. The nurses who participated in the pilot study were excluded from the study population. The tool of data collection consisted of the two parts first part; concerned with socio-demographic data of the nurses such as age, gender, qualification, and years of experience. Second part; concerned with nurses’ attitude regarding patient safety using the Safety Attitudes Questionnaire (SAQ), this questionnaire being one of the tools that most used to evaluate the safety attitudes among healthcare providers.
The SAQ instrument was developed by the Center for Healthcare Quality and Safety, University of Texas. In order to use this questionnaire, permission was obtained from the University of Texas to do the needed modification to be suited to PHCCs. This questionnaire consists of six dimensions: teamwork climate, safety climate, perceptions of management, job satisfaction, working conditions, and stress recognition. The 5-points Likert response scale of the agreement was used, this Likert-type scale rates answers from 5=strongly agree to 1=strongly disagree; negative phrases are encoded inversely. The score for means interpretation reference were strongly disagree 1 – 1.79; disagree 1.80 – 2.59; neutral 2.60 – 3.39; agree 3.40 – 4.19; strongly agree 4.20-5. The cut-off point is equal to 3.39, so a positive attitude was acknowledged if the weighted mean is more than 3.39. In contrast, a negative attitude was acknowledged if the weighted mean is less than 3.39.
Regarding sampling strategy and setting; the study was conducted in PHCCs of Riyadh city, Saudi Arabia. According to MOH in Saudi Arabia, the number of PHCCs are 2325 which covered 20 regions and consists of 19863 nurses. In Riyadh city there are 96 PHCCs including 1697 nurses; spread over the five health regions of the city (North, South, East, West, and Middle). The services offered by them include general practitioner services, childcare services, family medicine, maternity care, care for chronic diseases, dentistry, preventive medical care, nursing care, and pharmaceuticals (MOH, 2016). The Steven K. Thompson equation (Thompson, 2012) was used to calculate the required sample size from the total population, and a sample of 314 participants was obtained with a 95% confidence level and 5% margin errors. Multistage sampling was used which conducted through three stages; first stage Riyadh city was divided into 5 regions (East, West, Middle, North, and South); second stage simple random sample was used in order to select 35 PHCCs (7 centers from each region); third stage all nurses in each selected PHCC was included in the study.
The inclusion criteria for the study was registered nurses who work in PHCCs with one year and more experience, while the exclusion criteria were nurses less than one year of experience and the nurses who participated in the pilot study. The data were analyzed using SPSS Version 20. For descriptive statistical analysis, frequencies and percentages were used for all variables included in the study to describe the demographic data and explore the attitude of nurses. Weighted arithmetic means, arithmetic averages and standard deviations are also used. For inferential analysis, The Chi-Square test was used to examine the association between variables. The statistical test of significance or p-value in this study was set at <0.05. The internal consistency of the tool was measured by calculating the Cronbach’s alpha.
The ethical approval for this study was obtained from the King Fahad Medical City IRB committee with log number 18-597E. The explanatory covering letter was attached at the beginning of the survey indicating the aim of the study. Participating in the study is considered voluntary and participants have the right to refuse to participate in the study. They informed that ‟ feedback would not affect their evaluation at work, work status, position or salary”. Confidentiality and anonymity were maintained to protect the identity and position of the participants.
RESULTS
Table 1. Demographic characteristics of nurses participated in the study (n=314)
| Parameters | Frequency (%) | |
| Age in years : | ||
| 24 – 30 | 99 | 31.5 |
| 31 – 35 | 103 | 32.8 |
| 36 – 40 | 65 | 20.7 |
| > 40 | 47 | 15 |
| Mean (SD) | 34.3 (6.14) | |
| Gender: | ||
| Male | 83 | 26.4 |
| Female | 231 | 73.6 |
| Educational qualification: | ||
| Diploma | 183 | 58.3 |
| Bachelor | 131 | 41.7 |
| Master | 0 | 0 |
| Staff position: | ||
| Supervisor | 44 | 14 |
| Nurse practitioner | 253 | 80.6 |
| Assistant nurse | 17 | 5.4 |
| Direct contact with patients: | ||
| Yes | 294 | 93.6 |
| No | 20 | 6.4 |
| Years of experience: | ||
| 1-5 years | 66 | 21 |
| 6-10 years | 101 | 32.2 |
| > 10 years | 147 | 46.8 |
Table 1 showed a demographic overview of the respondents. The mean age of the participants was 34.3 years. Regarding gender, about (73.6%) of the participants were females while only (26.4%) were males. In terms of educational qualification, around half of the participants (58.3%) had a diploma and (41.7%) had a bachelor’s degree while no one neither had a master degree nor a doctorate. Turning to a staff position, most of the participants were nurse practitioners (80.6%) and the majority of them (93.3%) had direct contact with patients, and about (46.8%) their years of experience were more than 10 years.
Figure 1: Percentage of nurses receiving training program regarding patient safety
Figure 1: Presented that (54%) of participants received training program on patients’ safety.
Figure 2: Nurses’ source of information regarding patient safety
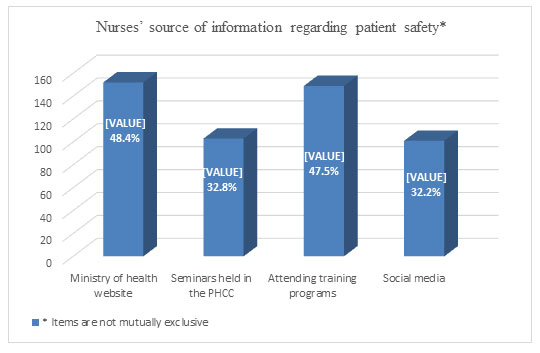
Figure 2: Clarified that about (48.4%) received their information regarding patient safety from the website of Ministry of Health and about (47.5%) from attending training programs while (32.8%) and (32.2%) from seminars held in their PHCCs and social media respectively.
Table 2. Attitude of nurses regarding patient safety in primary healthcare centers
| Parameter | Mean | *SD | Attitude | Rank |
| Teamwork climate | 3.64 | 1.15 | Positive | 2 |
| Job satisfaction | 3.78 | 1.02 | Positive | 1 |
| Perceptions of management | 3.19 | .87 | Negative | 4 |
| Safety climate | 3.61 | .83 | Positive | 3 |
| Working conditions | 3.12 | .87 | Negative | 5 |
| Stress recognition | 2.41 | .72 | Negative | 6 |
| Overall attitude | 3.29 | .76 | Negative | |
*SD= standard deviation
Table (2) Showed that the participants had a positive attitude regarding teamwork climate, job satisfaction, and safety climate dimensions with weighted mean 3.64, 3.78, and 3.61 respectively while they had a negative attitude regarding perceptions of management, working conditions, and stress recognition dimensions with weighted mean 3.19, 3.12, and 2.41 respectively. The overall attitude was negative with a weighted mean (3.29) which was less than the cut-off point (3.39).
Table 3. Relationship between nurses’ attitude regarding patient safety in PHCCs and years of experience, age, gender, qualification, and staff position
| Overall attitude | Years of experience (%) | X2 | df | P | |||||
| 1-5 years | 6-10 years | > 10 years | 6.21 | 2 | 0.04* | ||||
| Positive | 41 (13.1) | 54 (17.2) | 65 (20.7) | ||||||
| Negative | 25 (7.9) | 47 (14.9) | 82 (26.1) | ||||||
| Age (%) | |||||||||
| 24 – 30 | 31 – 35 | 36 – 40 | > 40 | 6.62 | 3 | 0.85 | |||
| Positive | 61 (19.4) | 48 (15.3) | 30 (9.6) | 21 (6.9) | |||||
| Negative | 38 (12.1) | 55 (17.5) | 35 (11.1) | 26 (8.3) | |||||
| Gender (%) | |||||||||
| Male | Female | 13.3 | 1 | 0.000* | |||||
| Positive | 28 (8.9) | 132 (42.1) | |||||||
| Negative | 55 (17.5) | 99 (31.5) | |||||||
| Education qualification (%) | |||||||||
| Diploma | Bachelor | 1.73 | 1 | 0.18 | |||||
| Positive | 99 (31.5) | 61 (19.4) | |||||||
| Negative | 84 (26.8) | 70 (22.3) | |||||||
| Staff position (%) | |||||||||
| Supervisor | Nurse practitioner | Assistant nurse | 5.84 | 2 | 0.05 | ||||
| Positive | 29 (9.2) | 125 (39.8) | 6 (1.9) | ||||||
| Negative | 15 (4.8) | 128 (40.8) | 11 (3.5) | ||||||
*P value is statistically significant < 0.05 level
Table (3) Clarified the statistical association between nurses’ attitude and their demographic data, the table showed that there was a statistically significant difference between nurses’ attitude and gender, also there was a statistically significant difference between nurses’ attitude and years of experience. Meanwhile, there was no statistically significant difference between nurses’ attitude and their age, educational qualifications, and staff position.
DISCUSSION:
This study analyzed the attitude of nurses regarding patient safety in PHCCs using the SAQ questionnaire which is a useful tool for evaluating safety attitudes, some studies showed that the validity and reliability measures of the SAQ were acceptable and others showed that it has good internal consistency reliability (Gabrani, et al., 2015; Li, et al., 2017). This was evident in this study where the results showed that more than half of the nurses attended training programs on patient safety, which is beyond any doubt that receiving patient safety training programs considered one of the important factors influencing safety attitudes for nurses and other healthcare providers. Several studies proved the importance of providing patient safety training programs for healthcare professionals to create and maintain a culture concerning patient safety issues which are thought to have an important effect on ensuring positive safety attitudes (Onler, 2010; Amarapathy, et al., 2013; Sevdalis, 2012). Also nearly half of nurses got their information regarding patient safety from the website of the Ministry of Health which means that the Ministry of Health in Saudi Arabia doing its best to provide healthcare workers with all information related to patient safety. However, the results of this study found that nurses working in PHCCs generally had a negative attitude towards patient safety, this result may be attributed to the fact that more attention to patient safety measures are directed more to hospitals than to PHCCs. This result comes contrary to what was mentioned with (Brasaite, et al., 2016; Durgun & Kaya, 2018) who reported that attitudes related to patient safety issues were positive among healthcare professionals, furthermore it was reported also by (Al-Khaldi, 2013) that attitude of the physician in PHCCs of Asser region in Saudi Arabia was positive. While (Alzahrani, et al., 2018), on the other hand, found that nurses had a negative attitude toward patient safety which come in the line with the present study. Also other studies (Ongun & Intepeler, 2017; Saberi, et al., 2017) showed a moderate level of professional attitude regarding patient safety which is lower than the international standards attitude regarding patients’ safety.
The results of the present study have reported that the nurses had a positive attitude in teamwork climate and job satisfaction which take the high rank between other dimensions; patient safety can be maintained if the relationship between healthcare workers relate well with each other, as this is the only way to create a conducive working atmosphere where although errors are not condoned if they occur, measures are put in place to ensure that they do not recur in the future.
A recently carried out study by (Al Lawati et al., 2019) has described about patient safety culture in primary health care in Muscat, Oman, and has identified that the teamwork was one of the core areas of strength in PHCCS. Another study by (Ongun and Intepeler, 2017) asserted that high scores in teamwork and job satisfaction among nurses play an important role in ensuring patient safety and creating a positive atmosphere for patients. Moreover, job satisfaction enhances the development of nurse’s collaboration with other healthcare professionals in order to achieve the goals of the healthcare organization. Thus, it is likely that nurses’ satisfaction influences their level of engagement in patient safety activities as well as patient safety outcomes. This result comes in concurrence with (Alzahrani, et al., 2018; Almutairi, et al., 2013; Algahtani, 2015) who found that more positive scores on job satisfaction are found between nurses. The results for this study also revealed that nurses had a positive attitude as regards to safety climate. It is important to ensure the safety climate in healthcare organizations to allow negotiation and mutual learning, as well as providing appropriate feedback in order to get rid of errors (Algahtani, 2015). A positive safety climate improves nurses’ production and decreases exposure to environmental hazards which reduces the number of accidents.
For perceptions of management, the results showed that nurses had a negative attitude regarding this dimension, and maybe this one of the important factors that affected the nurses’ overall attitude. There is no doubt that healthcare managers play an important role in forming nurses’ attitude toward patient safety, when managers openly display a positive attitude toward patient safety or manage the patient safety issues effectively, the general culture of patient safety within their organization is increased. Also, nurses tend to be more productive in the environment that stimulates a positive attitude, they feel more self-sufficient when their opinions heard and taken by their leaders in the context of improving patient safety and reduce the medical error, these are the main role of the managers. According to (Institute for Healthcare Improvement, 2017) top management need to show commitment to patient safety through providing required resources, ensuring transparency; understanding and applying quality improvement science, reliability, safety and continuous learning, creating an inspiring environment for innovation and risk mitigation, fostering environment of mutual respect and trust were people feel their opinions are valued and trustworthy. The result reported by this study was quite different from what was mentioned by (Saberi, et al., 2017) who found that the highest rate of positive attitude toward patient safety belonged to the dimension of ‘management perception’, also the study was done by (Mahfoozpour, et al., 2012) who reported the highest percentage of the positive attitudes among healthcare providers was toward the perception of management.
Regarding the safety climate, the nurses were had a positive attitude regarding this dimension. It is worth mentioning that regularly reviewing safety climate processes lead to improve the nurses level of thinking, therefore bring new ideas and hypotheses, as well as enhancing team collaboration which, in the end, will improve overall nurses’ performance resulting in improving the patient safety. Reporting systems which is one of the important part in assuring safety climate can be only effective when a strong feedback loops and evidence of action following reported harm is established. Feedback from incident reporting can optimize the learning from mistake, finding improvement opportunity, reduce the reoccurrence of errors, and enhance of overall patient safety (Panesar, et al., 2014)
Regarding the working conditions, the nurses were had a negative attitude, this maybe because of when nurses live in perpetual fear of retaliation from the immediate managers or supervisors, In the long run, patient safety further deteriorates since even opportunities that have been used to rectify the errors are squandered. This result was conflicting the results obtained by (Tabibi, et al., 2010) who demonstrated that the nurses’ attitude was positive in the work conditions dimension. Moreover, this finding was in concurrence with the results obtained by (Gutiérrez-Cía, et al., 2010; Lee, et al., 2010; Marinho, et al., 2014) which indicated the lowest score to be in the SAQ dimension was in work conditions, also it congruence with (Saberi, et al., 2017) who found that the lowest mean score of attitude toward the patient safety culture belonged to the same dimension. Regarding the stress recognition, the study showed that nurses had a negative attitude, this result in agreement with (Ongun and Intepeler, 2017) who asserted that stress recognition had the lowest score among the sub-scales of the operating room professionals’ SAQ. However, there are some studies in which the stress recognition score was found to be high (Onler, 2010; Kaya, et al., 2010).
Stress can trigger illness among healthcare workers especially nurses, in order to improve stress management, the healthcare professionals must acknowledge that stress caused by high work demands limits their activities and affects their health (Kogienl and Cedaro, 2014) which can lead to unsafe and low-quality of care. Moreover, the adequacy of the nurse-to-patient ratio and availability of the necessary information during the decision-making process affect positively on this dimension (Lee, et al., 2010). Many professionals encounter errors due to their heavy workload, which exhausts them and lowers their precision in the provision of care (Saberi, et al., 2017) all of these issues should be discussed with managers when addressing improvements to patient safety
Furthermore, the present study reported that about one-third of participants their age were ranged between 24 -30 years, more than half of them had a diploma as an educational qualification. Most of participants were nurse practitioners and less than half of them had more than 10 years’ experience. It should be noted that the present study found that there was statistically significant difference between gender and nurses’ overall attitude; also there was statistically significant difference between years of experience and nurses’ overall attitude. These came in the same line with the study done by (Durgun & Kaya, 2018) who stated that years of experience and patients’ safety issues were correlated, and nurses with experience showed expected results, used evidence more efficiently and developed critical thinking skills. These results showed that nursing experience had a positive impression on patient safety.
The present study also showed that there was no statistically significant difference between age and nurses’ overall attitude, meanwhile, the study done by (Brasaite, et al., 2016) recognized that age seemed to be associated with many safety attitudes scales, which were found to be higher in older age groups. Also, the current study showed that there was no statistically significant difference between educational qualification and nurses’ overall attitude, this may be because all participants had either diploma or bachelor no one had master or doctorate in nursing. The study was done by (Durgun & Kaya, 2018) also found that no noticeable difference between educational level and attitudes toward patient safety which supports the results of the current study.
CONCLUSION
As any healthcare organization; PHCCs continue to embrace the improvement of patient safety and quality, they must recognize the importance of nurturing a patient safety culture as well as the attitude of their healthcare providers regarding it. To achieve this, PHCCs’ management must understand how healthcare providers perceive their teamwork climate, safety climate, perceptions of management, job satisfaction, and working conditions. This study contributed to analyze nurses’ attitude regarding patients’ safety in primary healthcare centers of Saudi Arabia, which were found to be negative with a statistically significant difference between attitude and years of experience and gender while there was no statistically significant difference between nurses’ attitude and age, educational qualification, and staff position.
The evidence-based about the nature of patient safety risks and patient safety solutions in primary healthcare centers still weak, so it’s important to focus on patient safety and its adverse events in PHCCs, investigating attitude of all healthcare professionals working in PHCCs in relation to patient safety, in order to obtain a deeper understanding of the present situation. Attitude regarding patient safety in PHCCs is not only should be positive but also it should be effective. MOH can help shed light on the direction of the PHCCs as done in hospitals to instill a culture of patient safety within its workforce.
Funding sources: no external funding
Conflict of interests: none
REFERENCES
Algahtani FD., (2015). The culture in safety culture: exploration of patient safety culture in Saudi Arabian operating theatres, University of Adelaide; Ph.D. Thesis
Al-Khaldi YM., (2013). Attitude of primary care physicians toward patient safety in Aseer region, Saudi Arabia. Journal of family & community medicine, 20:153.
Al- Lawati, M., Short, S., Abdulhadi, N., Panchatcharam, S., Dennis, S. (2019). Assessment of patient safety culture in primary health care in Muscat, Oman: a questionnaire -based survey. BMC Family Practice 20:50. https://doi.org/10.1186/s12875-019-0937-4
Almalki M, Gerald G, Clark M., (2011). Healthcare system in Saudi Arabia: an overview. Eastern Mediterranean health journal, 17:784.
Almutairi A, Gardner G, McCarthy A., (2013). Perceptions of clinical safety climate of the multicultural nursing workforce in Saudi Arabia. Collegian, 20:187–94.
Alzahrani N, Jones R, Abdel-Latif ME., (2018). Attitudes of doctors and nurses toward patient safety within emergency departments of two Saudi Arabian hospitals. BMC health services research, 18:736.
Amarapathy M, Sridharan S, Perera R, Handa, Y., (2013). Factors Affecting Patient Safety Culture in a Tertiary Care Hospital in Sri Lanka. Int J Sci Technol Res, 2(3):173-80.
Brasaite I, Kaunonen M, Martinkenas A, Suominen T., (2016). Healthcare professionals’ attitudes regarding patient safety: cross‑sectional survey. BMC Res Notes, 9:177
Brotons C, Soriano N, Moral I, Rodriguez F, Banegas J., (2012). Prevention in primary care: the example of the program for prevention and health promotion. SESPAS report. Gac. Sanit, 26:151–57.
Canadian Nurses Association, (2002). Code of ethics for registered nurses. Ottawa Available from: http://www.cnanurses.ca/cna/documents/pdf/publications/CodeofEthics2002_e.pdf
Canadian Nurses Association, (2019). Patient safety: Joint position statement. Available from: https://www.cna-aiic.ca/-/media/cna/page-content/pdf-en/2019-joint-position-statement-_patientsafety.pdf?la=en&hash=4688BDFCF9B9D3FC6D0B210C89DBB5C757D6F7AC
Durgun H, & Kaya H., (2018). The attitudes of emergency department nurses towards patient safety. International emergency nursing, 40:29-32.
Fermo VC, Radünz V, Rosa LM, Marinho MM. (2016). Professional attitudes toward patient safety culture in a bone marrow transplant unit. Revista gaucha de enfermagem, 37(1).
Gabrani A, Hoxha A, Simaku A, Gabrani J., (2015). Application of the Safety Attitudes Questionnaire (SAQ) in Albanian hospitals: a cross-sectional study. Bmj Open., 5:775–80
Geevarghese F., (2012). Knowledge and attitude of nursing personnel regarding patient safety and rights in hospitals of Delhi. Nursing Journal of India,103:276.
Ghobashi MM, El-ragehy HA, Ibrahim HM, Al-Doseri FA., (2014). Assessment of patient safety culture in primary healthcare settings in Kuwait. Epidemiology, Biostatistics and Public Health, 11(3).
Gutiérrez-Cía I, de Cos P, Juan A, Obón-Azuara B, Alonso-Ovies Á, Martin-Delgado M., (2010). Perception of safety culture in Spanish intensive care units. Medicina clinica, 135:37-44.
Institute for Healthcare Improvement (IHI), (2017). A Frame work for safe, reliable, and effective care. Retrieve from: http://www.ihi.org/resources/Pages/IHIWhitePapers/Framework-Safe-Reliable-Effective-Care.aspx
Kaya S, Barsbay S, Karabulut E., (2010). The Turkish Version of the Safety Attitudes Questionnaire: Psychometric Properties and Baseline Data. Qual. Saf. Healthcare, 19:572-77.
Kogienl M, Cedaro JJ., (2014). Public emergency room: psychosocial impacts in the physical domain of the quality of life of nursing professionals. Rev Latino-Am Nursing, 22:51-8.
Lee WC, Wung HY, Liao HH, Lo CM, Chang FL, Wang PC., (2010). Hospital safety culture in Taiwan: a nationwide survey using Chinese version safety attitude questionnaire. BMC health services research, 10:234.
Li Y, Zhao X, Zhang X, Zhang C, Ma H, Jiao M., (2017). Validation study of the safety attitudes questionnaire (SAQ) in public hospitals of Heilongjiang province. China. PLoS ONE, 12(6): e0179486. https://doi.org/10.1371/journal. pone.0179486
Mahfoozpour S, Ainy E, Mobasheri F, Faramarzi A., (2012). Patients’ safety culture status among educational hospitals of Shahid Beheshti University of Medical Sciences. Pajoohandeh Journal, 17:134-41.
Marinho MM, Radünz V, Barbosa FF., (2014). Assessment of safety culture by surgical unit nursing teams. Texto & Contexto-Enfermagem 23:581-90.
Ministry of Health. Saudi Arabia, (2016). Statistical Year Book, Total Utilities in MOH by Region.
Ministry of Health. Saudi Arabia: Saudi Patient Safety Taxonomy, (2017). Available from:
https://www.moh.gov.sa/endepts/Nutrition/News/Documents/Saudi-Patient-Safety Taxonomy.
Ongun P, & Intepeler SS., (2017). Operating room professionals’ attitudes towards patient safety and the influencing factors. Pakistan journal of medical sciences, 33:1210.
Onler E., (2010). Patient Safety in the Operating Room Determination of Attitudes [dissertation]. Istanbul (Turkey): Istanbul University Health Sciences Institute, p.136.
Panesar, S., Carson-Stevens, A., Salvilla, S., & Sheikh, A., (2014). Patient safety and healthcare improvement at a glance, John Wiley& Sons.
Saberi M, Jamshidi E, Rajabi F, Seydali E, Bairami F., (2017). Attitude of Nurses toward the Patient Safety Culture: A Cross-Sectional Study of the Hospitals in Tehran, Iran. Journal of Patient Safety & Quality Improvement, 5:554-60.
Sevdalis N, Hull L, Birnbach JL., (2012). Improving Patient Safety in the Operating Theatre and Perioperative Care: Obstacles, Interventions and Priorities for Accelerating Progress. Br J Anaesth, 109:3-16. doi: 10.1093/bja/aes391.
Tabibi J, Nasiripour A, Maleki M, Raessi P, Mahmmoudi M, Azimi L., (2011). Survey of employees’ safety attitude in a teaching hospital Tehran 2010. Iran Occupational Health, 7:5-10.
Thompson S., (2012). Sampling, 3rd ed., Wiley Co., ISBN: 978-0-470-40231-3 Pp 59-60.
Webair HH, Al-ssani SS, Al-haddad RH, Al-Shaeeb WH, Bin Selm MA., (2015). Assessment of patient safety culture in primary care setting, Al-Mukala, Yemen. BMC Family Practice, 16:136.
World Health Organization, (2016). Regional Office for the Eastern Mediterranean. Patient safety assessment manual, 2nd ed. Available from: https://apps.who.int/iris/handle/10665/249569
World Health Organization, (2018). Patient safety Features: stories from countries, Q&As, Fact files, 10 facts on patient safety. Available from:
https://www.who.int/features/factfiles/patient_safety/en/
World Health Organization, (2019). Patient Safety and Risk Management Service Delivery and Safety. Patient Safety Fact files.

