
Pharmaceutical
Communication
Biosci. Biotech. Res. Comm. 11(3): 356-362 (2018)
Clinical uses and toxicity of Ergot,
Claviceps purpurea
An evidence-based comprehensive retrospective review
(2003-2017)
Raghad Al-Omari
1
, Atheer Al-Enazi
1
, Rizwan Ahmad*
2
, Niyaz Ahmad
3
, Atta Abbas Naqvi
4
and Adeeb Shehzad
5
1
College of Clinical Pharmacy, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia
2
Natural Products and Alternative Medicines, College of Clinical Pharmacy, Imam Abdulrahman Bin Faisal
University, Dammam, Saudi Arabia
3
Department of Pharmaceutics, College of Clinical Pharmacy, Imam Abdulrahman Bin Faisal University,
Dammam, Saudi Arabia
4
Department of Pharmacy Practice, College of Clinical Pharmacy, Imam Abdulrahman Bin Faisal University,
Dammam, Saudi Arabia
5
Department of Biomedical Engineering and Sciences, School of Mechanical and Manufacturing Engineering,
National University of Sciences and Technology, Islamabad, Pakistan
ABSTRACT
Ergot alkaloids produced by the fungusClavicepsparasitizing on cereals presents a high toxicity risk for animals
and humans due to presence of its alkaloid content. Ergot-alkaloid toxicity occurs via their medicinal use however
human poisoning from ergot plant is rare. The aim of this review is to determine the toxicity of ergot plant or ergot-
amine derivatives in humans. Databases such as Google scholar, PubMed, Scopus, Web of Science alongwith related
books and theses as well as the library resources from Imam Abdulrahman Bin Faisal University were used whereas
the Key words searched included; Ergot, Egotism, Ergotamine poisoning, Ergotamine interaction with HIV therapy,
Ergotamine overdose, and report cases of ergotism. The relevant literature search suggests many toxicity cases and
side effects associated with the use of ergot-alkaloids. More commonly it develops a condition known as ergotism i.e.
a disease or toxic condition produced by eating ergot grains or rye or chronic use of ergot drug. The characteristic
356
ARTICLE INFORMATION:
*Corresponding Author: rizvistar_36@yahoo.com
Received 1
st
July, 2018
Accepted after revision 21
st
Sep, 2018
BBRC Print ISSN: 0974-6455
Online ISSN: 2321-4007 CODEN: USA BBRCBA
Thomson Reuters ISI ESC / Clarivate Analytics USA and
Crossref Indexed Journal
NAAS Journal Score 2018: 4.31 SJIF 2017: 4.196
© A Society of Science and Nature Publication, Bhopal India
2018. All rights reserved.
Online Contents Available at: http//www.bbrc.in/
DOI: 10.21786/bbrc/11.3/2
Raghad Al-Omari et al.
features of ergotism consist of painful and cold extremities. Furthermore, a notable and severe interaction of ergot-
alkaloids was found in HIV patients using ergotamine and antiretroviral drugs together. Ergotamine which is one of
ergot preparation has poisonous effect when taken in over dose and it interacts with antiretroviral drugs also.
KEY WORDS: EGOTISM; MIGRAINE HEADACHE; POSTPARTUM HEMORRHAGE; ARTERIAL SPASM; CYANOSIS
INTRODUCTION
The ergot fungus (Claviceps purpurea) is family of sec-
ondary metabolites and is a common seed pathogen
of grasses and cereals. Ergot is a parasitic fungus that
belongs to the genus Claviceps and forms dark sclerotia
on various grasses and grains. After maturing, the scle-
rotia fall to the ground and remain partially buried for
the resting stage of ergot formation. This period occurs
during cold or winter weather, (Ehrlich et al., 2013).
Ergot plant has medicinal uses to treat some diseases;
even though, Ergot contain alkaloids which can cause
severe toxicity in mammals when ingested and thus the
fungal infection might provide protection for the host
plant against mammalian herbivores, (Panaccione et al.,
2012). Ergot alkaloids are natural products having nitro-
gen indole alkaloids. There are three group of ergot; I.
peptides (ergopeptines), II. Clavines and III. Lysergic acid
amides, (Gerhards et al., 2014).
There are more than fourty known ergot and usu-
ally six of them may cause toxicity by interaction with
neurotransmitters. These are ergotamine, ergocornine,
ergocryptine, ergocristine, ergosine and ergometrine,
(Mulac et al., 2011). Ergot alkaloids have pharmacological
and toxicological effect on several receptor systems in the
human body. Ergot become activated in the body to some
receptors and show cytotoxic affects and induces apopto-
sis in human primary cells, (Mulac et al., 2013).
Ergotism occurs when either the fungus is ingested
via the contamination of grain, for example, rye or by
the medicinal use of drugs derived from ergotamine
compounds. Ergot toxicity called Ergotism previously
known as Holy Fire, in some cases may lead to death,
(Floss, 1976). There are two forms of Ergotism; gangre-
nous and convulsive and both can occur in the same
individual. Gangrenous named as Saint Anthony’s, usu-
ally characterized by pain in one limb particularly the
calf and leg, in amed, swollen, and violet hand and foot
whereas in severe cases the limb will separate from the
knee with hemorrhage and may need a knee amputa-
tion. The other form of ergotism i.e. convulsive form
is accompanied with heaviness and numbness in limbs
with paresthesia well as diarrhea without vomiting. In
humans, ergot is used pharmacologically to inhibit lac-
tation, postpartum hemorrhage, and induce labor, (Lee
and Coll, 2009). Previously ergot was used in the treat-
ment of Parkinsonism and other endocrine and neuro-
logicaldisorders, (Tesh, 2015).
In addition, ergot induces cytotoxic and apoptotic
effect shows anti-cancer effect and thus used as a can-
cer therapy. In a study on two cancer lines (Hep-G2
and HT-29) ergot showed a high grade apoptotic effect,
(Mulac et al., 2013). Furthermore, ergot alkaloids have
an important widespread use in migraine headaches and
5-hydroxytryptamine (5-HT) receptors acts as binding site
for these ergot derivatives such as Ergotamine, Dihydro-
ergotamine, and Methysergide. They work as agonist of
5-HT1B, 5-HT1D, and 5-HT1F receptors to treat for treat-
ment as well as prophylaxis for migraine headache with a
high ef cacy, (Dholf et al., 2012). Though in human, ergot
complications i.e. ergotism appears rarely with symptoms
such as tachycardia, hypertension and arterial spasm, still
it is important to be taken care as ergot acts as a strong
vasoconstrictor and may cause severe adverse effects at
cardiac and limbs level, (Adam et al., 2014).
Current review aims to highlight the more impor-
tant and recently reported cases regarding ergotism in
humans with major symptoms observed, as associated
with the use of ergot-alkaloids. The literature will be
searched to extract out the factors behind ergotism and
to report the possible measure in order to tackle such
reasons. The study owes importance as it will compare
the therapeutic and toxic pro le for ergot and to con-
clude an overall scenario of how to use ergot-alkaloids
for therapeutic purposes and to avoid ergotism.
MATERIAL AND METHODS
Various databases searched were: Google scholar, Sci-
ence direct, Research gate, Web of Science, PubMed,
Science Finder, Scopus and Journals such as; Journal
of Ethnopharmacology, Frontier in Ethnopharmacology,
Thieme journals, Clinical Toxicology journal, Journal of
Agricultural and Food Chemistry, Journals of Toxicol-
ogy, Canadian Medical Association Journal, JSM foot
and ankle journal, Toxicology and Industrial Health
(SAGE journals) and The Royal College of Physician of
Edinburgh were searched. In addition, books and the-
ses and online as well as hard resources from library of
Imam Abdulrahman Bin Faisal University Damam, Saudi
Arabia was also searched.
Key words were also searched:
Ergot, Ergot alkaloids, reported case of Ergot toxicity,
adverse effects of ergot; ergotism, ergotamine toxicity,
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS A COMPREHENSIVE REVIEW OF ERGOT 357

Raghad Al-Omari et al.
clinical cases observed for ergot alkaloids, uses of ergot
alkaloids, interactions of ergot alkaloids.
The literature was searched for retrospective fteen
years i.e. 2003-2017. All the clinical cases regarding ergot
toxicity or ergotism were gathered and ltered as per the
inclusion and exclusion criteria as mentioned below;
Inclusion criteria
The clinical cases reported in humans associated with
the use of ergot or ergot alkaloids in any of its form
used, were included. The toxicity resulted due to over-
dose, long term use as well as any adverse effect and
drug interaction of ergot and ergot derivatives with HIV
drugs were also included in the study.
Exclusion criteria
Clinical cases regarding ergot toxicity, reported in ani-
mals or in vivo studies (cell lines) as well as in vitro stud-
ies were excluded from the study. Any clinical report with
minor side effects or adverse effects was also excluded.
Similarly, any interaction with conventional medicine
other than ergotism was excluded from the study.
Search result
The number of clinical cases, after an in-depth and
extensive review as well as the cases which met the
inclusion/exclusion criteria was found to be ten. These
cases are reported in detail in the forthcoming section of
literature review;
LITERATURE REVIEW
The ten cases ltered as per eligibility criteria are
explained in detail as below. These cases are reported
here-in an ascending year wise order;
A. Clinical case reported in 2003
i. Overdose of Ergot preparation
A 36-years old man was diagnosed with HIV and lym-
phoma eight years ago and he was taking triple antivi-
ral therapy. He developed bilateral claudication and foot
cyanosis. History revealed that the patient was taking
2 mg of ergotamine tartrate due to migraine headache.
The overdose of ergot-alkaloid developed paresthesia,
and coolness in feet without pain. The left foot was
cyanotic and he was administered with heparin IV and
oral nifedipine. The symptoms resolved within one week
of the therapy, (Badwin and Ceraldi, 2003).
B. Clinical case reported in 2005
ii. Ergot toxicity in neonate
An infant born at 41 weeks gestation period was acci-
dentally administered with methylergonovine (I.M.)
instead of naloxone for respiratory depression. Soon
after administration he suffered from capillary re ll,
low oxygen saturation, his hand and feet became warm
and pink and after sometime his color became grey with
development of hypercarbia (partial pressure of carbon
dioxide). The infant was put on mechanical ventilation
and treated with nitroprusside infusion. The condition
recovered with 10 days of hospital treatment, (Bangh
et al., 2005).
C. Clinical case reported in 2009
iii. Ergotamine with caffeine
A 28-year old patient reported to hospital with pain in
both legs. Upon history it was revealed that the patient
used ergotamine tartrate (1 mg) with caffeine (100 mg)
for 3 days, due to a bi temporal headache a week ago.
Thus he developed the symptoms of severe leg pains,
especially below the ankle with cold and purple legs.
Hands were also cold but without any pain. The patient
was treated with I.V crystalline uids and nitroprus-
side as well as oral nifedipine (every 8 h). Papaverine
was also administered as the patient had arterial spasm
whereas Enoxaparine was administered in order to
inhibit any thrombus formation, (Musikatavorn et al.,
2009).
D. Clinical case reported in 2009
iv. Ergotamine with Anti-HIV
A 31-year female patient on anti-HIV therapy used
ergotamine for migraine headache. Soon after she start
to complain about pain in lower extremity and her both
legs were cold particularly the left leg. In addition, a
palpable popliteal artery with peripheral pulses was also
observed. This condition is termed as Ergotism. The sign
and symptoms resolved gradually with the use of Nifedi-
pine (30 mg) and Enoxiparine was used as treatment for
Ergotism, (Cagatay et al., 2009).
E. Clinical case reported in 2010
v. Ergotamine used with clarithromycin (Antibiotic)
An eighteen year ole female patient reported with a pain
in emergency which started 2 days ago. The symptoms
she presented were; cool cyanotic lower extremities,
tender on palpitation, pain at rest, a thin iliac to pop-
liteal region and blood ow with increased velocity. The
history revealed that the patient was using ergotamine
since 3 year for migraine whereas at the same time she
used clarithromycin for upper respiratory tract infection.
Heparin was administered in order to prevent possible
thrombotic complications and infusion of bupivacaine
was given. The symptoms resolved within a month,
(Demir et al., 2010).
358 A COMPREHENSIVE REVIEW OF ERGOT BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
Raghad Al-Omari et al.
F. Clinical case reported in 2010
vi. Ergotamine interaction with anti-HIV drugs produces
paresthesia
A 29-year old patient using antiretroviral therapy for
HIV traveled Egypt and developed a severe migraine. A
local physician prescribed him ergotamine tartrate for
two weeks. Soon after its use, he developed sever pain
in left upper extremities, pale and cool wooden hand
with paresthesia, absent arterial pulse and axillary artery
stenosis, and he was facing dif culty in writing. Heparin
was started as therapy to inhibit any coagulation. Pros-
tacyclin IV and topical Nitroglycerine was used as ther-
apy. The symptoms resolved within six days, (Frohlich
et al., 2010).
G. Clinical case reported in 2012
vii. Neonate and methylergonovine
A female neonate, 10 minutes after her delivery, was
given methylergonovine instead of vitamin-K. after 30
minutes, she developed respiratory depression with cya-
nosis in extremities. Naloxone IM was administered to
recover the symptoms, (Sullivan et al., 2012).
H. Clinical cases reported in 2014
viii. Ergotamine with azithromycin (Antibiotic)
A 35-year old women reported with severe pain and pal-
lor in left foot, into emergency room. She was using
ergotamine since long time due to migraine, and in
addition she used azithromycin for four days (as she
was heavy smoker). Upon examination, vasospasm and
acute arterial embolism was observed due to interac-
tion between azithromycin and ergotamine. For treat-
ment purpose, ergotamine was stopped and Heparin was
administered for a week. The symptoms resolved gradu-
ally,( Adam et al., 2014).
I. Clinical cases reported in 2016
ix. Ergotamine use with caffeine
A 33-year old women presented with critical limb
ischemia, foot camping pain and a decreased walking
distance for 36 hours. Two days ago she used ergot-
amine tartrate (1 mg) and caffeine (100 mg) for migraine
headache. She was treated with vasodilator (PG-E1 I.V.),
pentoxifylline, heparin and sildena l for every 8 hours.
The patient recovered partially within 4 days, however
for full recovery she was further prescribed with aspirin,
sildena l and cilostazol, (Eduardo et al., 2016). Ergot-
amine overdose develops cerebral ergotism
A 49-year old patient with a history of HIV infection
treated with ritonavir used ergotamine (3g) for migraine.
He developed cerebral ergotism with an ischemic attack
after 20 minutes. The Cervical Doppler ultrasound
revealed a narrowing in both internal carotid arteries.
The treatment plan consist of; stopping ergotamine, and
changing the antiretroviral regimen, aspirin (325 mg)
was administered and bed rest suggested. The patient
became asymptomatic after a week. (Gaye-Saavedra
et al., 2016) The cases reported for Ergot are presented in
detail in Table 1, as below;
DISCUSSION
Ergot, with the most prominent member in group i.e.
Claviceps purpurea, grows on rye and other grasses. It is
considered as a poisonous plant that produce ergotism
in humans and sever toxicity in mammals. The improper
use or overdose of ergot may lead to various severe
complications, discussed as below.
Ergot develops psychological effects;
convulsive,
spasmodic or nervous ergotism i.e. chronic serious stage
of ergotism called “convulsive stage”, can occur due to
patchy damage of mid brain and cerebral hemisphere
which leads to degeneration in the posterior column of
spinal cord. The patient in such cases suffers from opistho-
tonos strong muscle spasm, tonic or clonic spasm of limbs,
battened tongue, dilated pupils, mania, dementia, glau-
coma, and delirium. In addition, the patient may develop
status epilepticus/multiple convulsions with less or lack
of sleep and nally coma and death, (Lee and Coll, 2009).
Ergonovine evoke coronary artery spasm (CAS);
earlier, ergonovine (i.v.) was considered as a useful test
for CAD diagnosis however, recently it has been reported
that it may provoke variant angina in patients. It effects
vascular smooth muscles via alpha adrenergic agonist
activity and leads to vasoconstriction. Similarly, in CNS
it blocks the baroreceptors and prevents response of
re ex bradycardia. Thus it is considered an unsafe drug
in CAD patients because ergonovine may develop severe
hypertension, myocardial infarction, seizures, intracer-
ebral hemorrhage and death, (Curry and Pepine, 1977).
Acute coronary syndrome with myocardial bridg-
ing;
Ergotamine may induce vasoconstriction in coro-
nary, cerebral and pulmonary arteries and leads to
change in ECG pattern. A case of ergotamine overdose
was reported in 2003, for a 48-year aged women with
migraine headache, whereby she developed recurrent
chest pain with a complaint since last 10 days. The ECG
showed T-wave inversion and elevated ST-segment.
This shows that ergotamine may cause serious cardiac
adverse effects such as; arrhythmias, coronary vasos-
pasm and death, (Shimony et al., 2006).
Induces serotonin syndrome;
it can be a mild to
life-threatening syndrome. Dihydroergotamine, binds
to serotonin receptors in the dorsal horn of spinal
cord, result in serotonergic hyper-stimulation and may
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS A COMPREHENSIVE REVIEW OF ERGOT 359
Raghad Al-Omari et al.
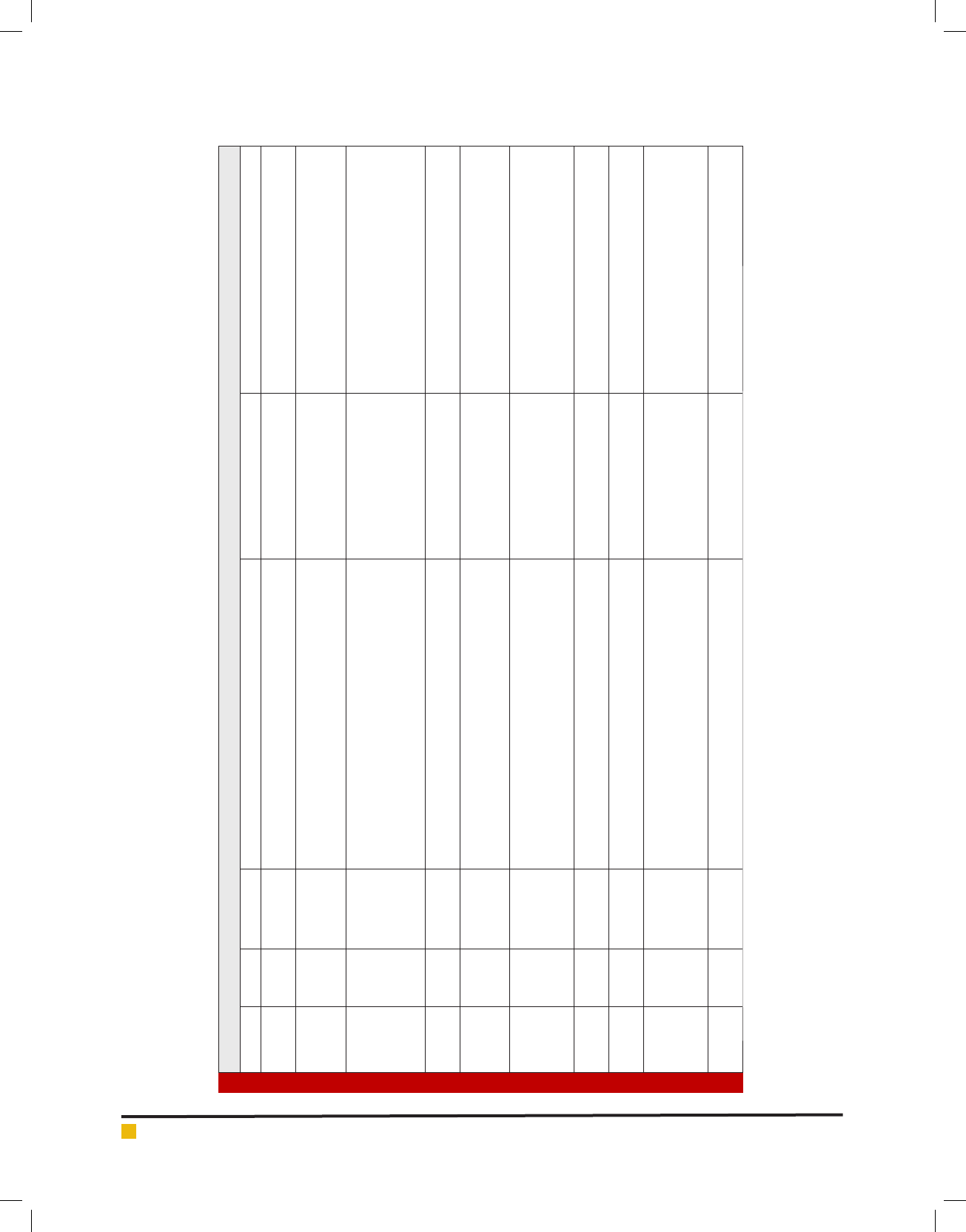
Table 1. Clinical cases reported for ergot
Case No. Age Gender Clinical manifestation Cause Treatment plan
1 36 Male
-Paresthesia and coldness of left foot
-Loss of sensation
Ergotamine tartrate for
migraine
-Heparin-IV
-Nifedipine orally
2 41 weeks Male infant
-Warm pink hands and feet
-Low oxygen saturation
-Hypercarbia-Oliguria
- Methylergonovine IM - Nitroprusside infusion
-Furosemide
3 28 Male
-Painful ,cold, and purple left legs especially below ankle
-Arteries spasm
-Ergotamine tartrate for bi
temporal headache
-Crystalloid uids(IV)
-Sodium nitroprusside (IV)
-Nifedipine orally
-Papaverine for arteries spasm
-Enoxaparin to prevent thrombus formation
4 31 Female
-Pain, cold lower left extremity
-Palpable popliteal artery
-Ergotamine for migraine +D-
DI with anti-HIV
-Nifedipine
-Enoxaparin
5 18 Female
-Cool cyanotic lower extremities
-Tender on palpitation
-Thin arteries with increased blood ow velocity
-Ergotamine for migraine
-Heparin
-Infusion of bupivacaine
6 29 Male
-Painful cold left upper extremities
-Pale wooden hands
Paresthesia
-Writing dif culties
Ergotamine tartrate for
migraine for 2 weeks + D-DI
with anti-HIV
-Heparin
-Prostacyclin IV
-Nitroglycerin(dermal application)
7 10 min Female
-Respiratory depression
-Cyanosis in her extremities
Unintentional use of
methylergonovine
Naloxone IM
8 35 Female
-Pain and pallor in the left foot
-Vasospasm and acute arterial embolism
Ergotamine for migraine Heparin for 7 days
9 33 Female
-Critical limbs ischemia
-Foot camping pain
-Decreased walking distance
Ergotamine tartrate for
migraine+
D-DI with ritonavir
- Prostaglandin E1(IV)
- Pentoxifylline
- heparin
- sildena l every(8h)
10 49 Male
-Cerebral ergotism
-Ischemia
Ergotamine overdose +D-DI
with ritonavir
325mg aspirin+ bed rest
360 A COMPREHENSIVE REVIEW OF ERGOT BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
Raghad Al-Omari et al.
develop “convulsive ergotism” characterized with symp-
toms of behavioral changes and mental disturbances,
agitation, sweating, fever, and hallucination etc. (Eadie,
2003).
Ergotamine and its interaction with macrolide anti-
biotics;
the combination of ergotamine with erythromycin
is considered and reported as a dangerous combination.
The reason behind is; macrolides have hepatic circula-
tion with ergotamine whereby it causes severe vascular
spasm and transient renal ischemia. And this is due to
macrolide inhibition of cytochrome P-450 metabolism
leading to an increase serum ergotamine concentration.
(Ghali et al., 1993) A clinical case reported in 2010 about
a woman with sore throat and migraine. She was pre-
scribed with erythromycin (500 mg) and ergotamine (100
mg) and soon after the combined use of these drugs she
developed pain and paresthesia in both feet as well as
numbness in hands. (Tseng et al., 2010) Though ergot may
have unwanted side effects or adverse effects as observed
above, however it is also a well-known fact that ergot
possess potential advantages as discussed below.
Bromocriptine as treatment of AML:
acute amyloid
leukemia is a type of cancer that affect the blood and
bone marrow. Bromocriptine is a hydrogenated ergot
derivatives with dopamine agonist activity, a novel
therapy as Anti-AML, induce apoptosis for AML cells.
(Lara-Castillo et al., 2016).
Bromocriptine as a treatment of breast cancer:
there
is a role of dopamine in development of cancer whereas
bromocriptine via down regulation of prolactin, result in
decrease and suppress the proliferation of MCT-7 cells
and induce apoptosis. It also shows effectiveness in idi-
opathic granulomatous mastitis (IGM) associated with
hyperprolactinemia. (Majid et al., 2015).
Ergot still the best as compared to triptans:
ergot
is still a drug of choice in migraine. It has more good
activity as compared to triptans as a powerful vaso-
constrictor because it works longer and better for pro-
long attacks than some triptans. Ergotamine is still very
useful and is used in many countries to relief migraine
headache. Rectal ergotamine reported higher ef cacy as
compared to triptans with rectal ergotamine activity of
(73%), while triptan rectally was (63%). (Marcelo et al.,
2003).
Reduce postpartum hemorrhage:
Ergotamine IM/IV,
as prophylactic agent, shows a good reduction in post-
partum hemorrhage when coadminstered with analgesic
to reduce the pain. An optimum result predicted with
intramuscular injection of ergotamine oxytocin combi-
nation called (Syntometrine) at the end of second stage
of labor. (Liabsuetrakul, 2007).
Ergot toxicity is due to cytochrome P-450:
Ergot-
amine is metabolized via CYP enzyme and interaction
with enzyme inhibitors drugs can increase its level in the
body which will lead to toxicity such as in the case of
antiviral and antibacterial drugs. Grapefruit also has been
reported to increase the level of ergotamine, thus it shows
that toxicity as resulted may not be due to ergotamine
itself, but due to interaction with drugs inhibiting the
enzymes. (Badwin and Ceraldi, 2003) Current review con-
sist of clinical cases reported due to use of ergot. It was
observed that the misuse or use without proper medical
guidance may result a condition known as ergotism. The
major symptoms for ergotism includes; vasospasm, arte-
rial embolism, pain and coldness in feet especially the left
one, respiratory depression particularly in neonates, par-
esthesia and decreased walking distance. The treatment
applied for these conditions mostly included vasodilators
and Heparin and almost all of the cases observed were
due to ergotamine overdose or drug-drug interaction
with protease inhibitors. In few of the cases an interac-
tion among ergot alkaloids and other drugs, especially
antivirals and azithromycin, was observed when they are
administered together. Furthermore, in most of the cases
it affected elder people i.e. age of 30 or likewise, however
it can affect infants when it’s given by medical mistake.
Regarding gender it effects both female and male equally
however it was observed that patients with HIV disease
are more prone to ergotism due to severe interaction. Two
cases were observed where toxicity of ergot resulted due
to overdose of ergotamine.
Plants remains the well-known sources of treating
many ailments mostly working as antioxidant, antidia-
betic and antiglycation, (Ahmad et al., 2013 & 2014) and
the people mostly possesses sound knowledge regard-
ing the use and treatment of most of the plants (Ahmad
et al., 2017).
However, in most of the cases the poisoning or toxicity
cases are not known to common peoples. Herein, we men-
tioned ten poisoning cases for ergot where the general
and common symptoms observed in elder patients, due to
toxicity were; painful and coldness lower extremity espe-
cially the left foot, ischemia and purple legs whereas, the
symptoms of affected infants were; respiratory depression
and pinkish skin. In some cases the lab tests showed nor-
mal hemoglobin, white blood cells with a normal temper-
ature (37-37.7C) measured orally. The common treatment
used in such toxicity cases was; aspirin, low molecular
heparin given IV, and nifedipine orally.
CONCLUSION
Finally, ergot plant has medicinal uses as well as toxic
effects. Current review has found poisoning cases which
were mostly due to overdose, mistakenly administered
or interaction with anti-HIV drugs for ergot alkaloids.
Any disease condition using ergot with proper dose,
time and under sound medical supervision whereby the
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS A COMPREHENSIVE REVIEW OF ERGOT 361

Raghad Al-Omari et al.
interaction with other drugs is taken under considera-
tion, may result a proper therapeutic outcome for ergot.
REFERENCES
Adam G, Kurt T, Çınar C, Sarıyıldırım A, Resorlu M, Uysal F,
Yener AU, Ozcan S. (2014). Ergotamine-induced vasospastic
ischemia mimicking arterial embolism. Ulus Travma Acil Cer-
rahi Derg. 20(4): 291-294.
Ahmad A, Upadhyay A, Ahmad M, Pieters L. (2013). Antioxidant,
antliglycation and antimicrobial activities of Ziziphus oxyphylla
and Cedrela serrata Extracts. Eur J med plants. 3(4): 520-529.
Ahmad R, Ahmad M, Jahan N, Mehjabeen. (2014). Phyto-
chemical screening and anti-oxidant activity of the two plants
Ziziphus oxyphylla Edgew and Cedrela Serrata Royle. Pak J
Pharm Sci. 27(5):1477-82.
Ahmad R, Naqvi AA, Ahmad N, Baraka M, Mastour M, Al
Sharedah S, Al Ghamdi S, Al Rabae G, Al Ghamdi MS. (2017).
Awareness, perception, attitude, and knowledge regarding
complementary and alternative medicines (cams) among the
pharmacy and medical students of a public university in Saudi
Arabia. Arch Pharm Prac. 8(2):51-63.
Baldwin ZK and Ceraldi CC. (2003). Ergotism associated with
HIV antiviral protease inhibitor therapy. Journal of Vascular
surgery. 37(3): 676-678.
Bangh SA, Hughes KA, Roberts DJ, Kovarik SM. (2005). Neo-
natal Ergot Poisoning: A Persistent Iatrogenic Illness. Ameri-
can Journal of Perinatology. 22(5): 239-243.
Belser-Ehrlich S, Harper A, Hussey J, Hallock R. (2013). Human
and cattle ergotism since 1900: symptoms, outbreaks, and reg-
ulations. Toxicol Ind Health. 29(4): 307-16.
Cagatay A, Guler O, Guven K. (2009). Ergotism Caused by Con-
current Use of Ritonavir and Ergot Alkaloids: A Case. Acta
chirurgica Belgica. 109(5): 639-640.
Curry JC and Pepine JR. (1977). Effects of Ergonovine in
Patients. Circulation journal. 56(5): 803-809.
Demir S, Akın S, Tercan F, Arıbog˘ an A, Og˘uzkurt L. (2010).
Ergotamine-induced lower extremity arterial vasospasm pre-
senting. Interventional radiology, Turkish Society of Radiol-
ogy. 16(2): 165-167.
Dhlof C, Maassen A, Brink VD. (2012). Dihydroergotamine,
Ergotamine, Methysergde, and sumatriptn-Basic science in
Relation to Migraine treatment. The journal of head and face
pain banner. 52(4). 707-714.
Eadie MJ. (2003). Convulsive ergotism: epidemics of the sero-
tonin syndrome?. The lancet neurology. 2(7): 429-434.
Eduardo J, Ayarragaray F, Panno M. (2016). Ergotism and Ret-
roviral Therapies: An Association not so Unusual. JSM Foot
And Ankle. 1(3): 1-2.
Floss GH. (1976). Biosynthesis of ergot alkaloids and related
compounds. Tetrahedran. 32.873- 912.
Fröhlich G, Kaplan G, Amann-Vesti B. (2010). Holy re in an
HIV-positive man: a case of 21st-century ergotism. CMAJ.
182(4): 378-380.
Gaye-Saavedra GA, et al., (2016). Transient ischemic attack
caused by cerebral ergotism. Arquivos de Neuro-Psiquiatria.
1603(1): 114-114.
Gerhards N, Neubauer L, Tudzynski P, Shu-Ming Li. (2014).
Biosynthetic Pathways of Ergot Alkaloids. Toxins. 6(12), 3281-
3295.
Ghali R, Léan JD, Douville Y, Noël HP. (1993). Raymond Labbé.
Erythromycin-associated ergotamine. Annals of Vascular sur-
gery. 7(3): 291-296.
Lara-Castillo MC, Cornet-Masana JM, Etxabe A et al., (2016).
Repositioning of bromocriptine for treatment of acute myeloid
leukemia. Journal of Translational Medicine. 14(1): 1-11.
Lee MR. (2009). The history of ergot of rye (Claviceps pur-
purea). Journal of Royal College of Physicians of Edinburgh.
39(2). 79-84.
Liabsuetrakul T, Choobun T, Peeyananjarassri K, Islam QM.
(2007). Prophylactic use of ergot alkaloids in the third stage of
labour. Cochrane Database Syst Rev. 18;(2).
Majid P, Ghasem A, Seyed HH, Abdolkhalegh D. (2015). New
Perspective Therapy of Breast Cancer Based on Selective Dopa-
mine Receptor D2 Agonist and Antagonist Effects on MCF-7
Cell Line. Bentham Science Publishers. 10(2): 214-223.
Marcelo E, Stewart JB, Tepper. (2003). Ergotamine and Dihy-
droergotamine. The New England Center for Headache Stan-
ford USA. 7(1): 55-62.
Mulac D, Humpf HU. (2011). Cytotoxicity and accumulation of
ergot alkaloids in human primary cells. Toxicology. 11;282(3):
112-21.
Mulac D, Lepski S, Ebert F, Schwerdtle T, Humpf HU. (2013).
Cytotoxicity and uorescence visualization of ergot alkaloids
in human cell lines. J Agric Food Chem. 16;61(2): 462-71.
Mulac D, Lepski S, Ebert F, Schwerdtle T, Humpf HU. (2013).
Cytotoxicity and Fluorescence Visualization of Ergot Alkaloids
in Human Cell Lines. Journal of agricultural and food chemis-
try. 61(2). 462-471.
Musikatavorn K and Suteparak S. (2009). Ergotism unrespon-
sive to multiple therapeutic modulities, including sodium
nitroprussside resulting in limb loss. Clinical toxicology. 46(2):
157-158.
Panaccione DG, Ryan KL, Schardl CL, Florea S. (2012) Analysis
and modi cation of ergot alkaloid pro les in fungi. Methods
in Enzymology, 515: 267-290.
Schardl CL. (2015). Introduction to the Toxins Special Issue on
Ergot Alkaloids. Toxins. 7(10). 4232–4237.
Shimony A, Romem A, Horowitz S, Boehm R, Horowitz J.
(2006). Acute coronary syndrome associated with myocardial
bridging due to ergotamine treatment for migraine. Interna-
tional journal of cardiology. 113(1): E7-E8.
Sullivan R, Nelsen J, Duggineni S, Holland M. (2012). Man-
agement of methylergonovine induced respiratory. Informa
healthcare Clinical Toxicology. 51(1): 47-49.
Tseng CW et al., (2010). Acute paresthesia in a patient with
migraine. Journal of Clinical Neuroscience. 1328(1): 20-20.
362 A COMPREHENSIVE REVIEW OF ERGOT BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS