
Medical
Communication
Biosci. Biotech. Res. Comm. 9(4): 878-883 (2016)
Application of WHOQOL-BREF for the evaluation of
the quality of life in elderly patients with heart failure
Mahshid Borumandpour* Medical Student, Medical School, Fasa University of Medical Sciences, Fasa, Iran,
Gholamabbas Valizadeh Cardiologist, Medical School, Fasa University of Medical Sciences, Fasa, Iran,
Azizallah Dehghan Ph.D Epidemiology, Noncommunicable Diseases Research Center, Fasa University
of Medical Sciences, Fasa, Iran, Alireza Pourmarjani, Research Center for Health Sciences, Department
Epidemiology, Shiraz University of Medical Sciences, Shiraz, Iran and Maryam Ahmadifar Medical Student,
Medical School, Fasa University of Medical Sciences, Fasa, Iran
ABSTRACT
Heart failure is the most common cardiovascular disease and its prevalence and incidence increase as the age goes up.
This chronic situation affects the quality of life of patients and their family. The main objective of this study was to
determine quality of life of elderly patients with heart failure. A cross-sectional study conducted among 150 patients
with heart failure aged 50 and above who entered cardiovascular clinic and Coronary Care Unit (CCU) ward of Vali-
Asr hospital of Fasa, Iran, from March to August 2013. Patients with a left ventricular ejection fraction below 50%
entered. WHOQOL-BREF questionnaire was used to evaluate the quality of life of patients. All the statistical analyses
were performed using the statistical package for social sciences version 16.0. Overall we enrolled 147 patients includ-
ing 77 (52.3 %) males and 70 (47.7 %) females with the mean age ± standard deviation of 63±27 years. There was
not any signi cant relationship between NYHA class, ejection fraction, past medical history of hypertension, diabetes
mellitus, chronic obstructive pulmonary disease, renal failure, pulmonary hypertension in patients and variables of
our questionnaire. Social and environmental aspects were the highest and lowest scores of this questionnaire, respec-
tively (53.85 ±21.28 and 45.74 ±17.67). There was not any correlation between job of patients and any aspect of
their quality of life (p-value = 0.49 for total).Our results indicated that the majority of heart failure patients had poor
and undesirable quality of life and the women have weaker scores of quality of life variations than men. Therefore,
controlling some available variables among these patients is suggested.
KEY WORDS: HEART FAILURE, QUALITY OF LIFE, WHOQOL-BREF
878
ARTICLE INFORMATION:
*Corresponding Author: mahshid.boroomand@yahoo.com
Received 19
th
Sept, 2016
Accepted after revision 21
st
Dec, 2016
BBRC Print ISSN: 0974-6455
Online ISSN: 2321-4007
Thomson Reuters ISI ESC and Crossref Indexed Journal
NAAS Journal Score 2015: 3.48 Cosmos IF : 4.006
© A Society of Science and Nature Publication, 2016. All rights
reserved.
Online Contents Available at: http//www.bbrc.in/
Mahshid Borumandpour
INTRODUCTION
Heart failure is the most common cardiovascular dis-
ease as a chronic, progressive, and disabling disease,
worldwide. Its prevalence and incidence increase as the
age goes up; that approximately one percent of more
than 50 years old people and 10 percent of people older
than 80 years old suffer from heart failure in the United
States. In addition, with the progression in medical care
and surgery, patients who survive myocardial infarction
subsequently develop with heart failure (Jaarsma et al.,
2000).Increase in the prevalence of heart failure results
from complications of infections, in ammation, vascu-
lar, and valvular heart disease. Therefore, it has become
a major health problem and an epidemic disorder in the
United States. Five million people suffer from heart fail-
ure in this state which approximately 500,000 new cases
add to this number annually and are expected to be dou-
bled in the next 30 years (Zambroski, Moser, Bhat, &
Ziegler, 2005).According to the Center of Disease Control
and Prevention (CDC) a study published in the year 1380
and showed that the number of patients with heart fail-
ure that have been reported in 18 provinces was 3337
per 100,000 populations. In an epidemiological survey
in the year 1377 in Iran, 25% of patients hospitalized
in different wards of hospital were cases of heart failure
(Rahnavard et al 2006).
Heart failure symptoms are something shortness of
breath and blood ow, dizziness, angina, edema, and
ascites. These symptoms predispose the patients to expe-
rience exercise intolerance and changes in their lifestyle
that nally affect their life satisfaction and quality.
Patients will be restricted in job tasks, family interac-
tions, and social life that will nally lead to social isola-
tion and depression (Dunderdale et al 2005).Based on
who organization, the quality of life is people’s de ni-
tion of their selves in life from many aspects such as cul-
ture, their goals in their life, value of their living system,
expectations, their standard beliefs and their priorities.
Therefore, it has been a subjective issue which is not
visible for anyone. Moreover, it is based on people’s per-
ceptions of the different aspects of their lives (Dehghan
et al 2011). In health care system, control and giving
good care to chronic diseases is very important these
days, these diseases healing is almost impossible but
their fatality is not imminent. So, improving the quality
of life should be considered as a consequent of clinical
and medical researcher (Kash et al 2015).
Martensson et al.(2003) have also suggested that the
primary source of depression and decrease in the quality
of life in these patients is due to the adverse physical
symptoms of the disease.Exercise intolerance disable the
patients to perform activities of daily living, it creates
dependency and help resulting in decrease in their qual-
ity of life (Molloy et al 2005). Mc Murray et al. carried
out a study on heart failure patients in the year 2004
and concluded that the total years of potential life lost
in heart failure patients is 6.7 years per 1,000 men and
5.1 years per 1000 women in Australia (McMurray &
Stewart, 2002).
Shojaie (2008) studied the quality of life of 250
patients with heart failure in Tehran, which revealed that
76.4% of patients had undesirable and relatively desira-
ble quality of life. According to this study, increase in the
age and the frequency of hospitalization and prolonged
disease will make much poorer quality of life for these
patients.Another similar study was done in Zahedan Iran
by Ebrahimi et al. (2007) They concluded that there is a
relationship between the quality of life and job, marital
status, age, disease duration and the frequency of hos-
pitalization. In addition, there is a signi cant relation-
ship between being male and experiencing a better life
quality. This study showed the negative impact of heart
disease on the quality of life .According to aging popu-
lation in Iran and increase in cardiovascular diseases in
developing countries, we conducted this study to assay
the quality of life of elderly patients with heart failure.
MATERIAL AND METHODS
In this prospective cross-sectional study, 150 patients
with heart failure entered cardiovascular clinic and
Coronary Care Unit (CCU) ward of Vali-Asr hospital, a
tertiary health care center af liated with Fasa University
of Medical Sciences, Fasa, Iran, from March to August
2013. Patients were included according to the American
Heart Association criteria of diagnosing cardiovascular
disease (Lloyd-Jones et al., 2009). Patients with stable
congestive heart failure, (NYHA class I–III) who referred
to the hospital and clinics of cardiovascular disease
enrolled the study. Inclusion criterion was a left ven-
tricular ejection fraction below 50%, as determined by
transthoracic echocardiography. Patients in NYHA func-
tional class IV were excluded, as were those who had
neurological, orthopedic, peripheral vascular, or severe
pulmonary diseases. Furthermore, patients were divided
into four groups according to the stage of heart failure
as follows: stage one: risk factor only, stage two: symp-
toms without signs, stage three: existences of signs but
improved by drugs, and stage four: existences of signs
without any improvement with drugs.
Demographic information was recorded by a
researcher checklist. The quality of life of the patients
were assessed with World Health Organization (WHO)
quality of life questionnaire. This questionnaire included
demographic information and ve dimensions of heart
failure patients` quality of life. Trained people helped
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS APPLICATION OF WHOQOL-BREF FOR THE EVALUATION OF HEART FAILURE 879
Mahshid Borumandpour
the illiterate patients to ll out the questionnaire.
(WHOQOL-BREF), this instrument is one of the known
instruments that has been developed for cross-cultural
comparisons of QOL and is available in many languages
(Gholami et al 2013).
Whoqol-BREF questionnaire evaluates QOL in four
aspects, physical, psychological, social and environmen-
tal health, with 24 questions (7-6-3 and 8 questions for
each dimension). The rst two questions are not related
to any aspect and evaluate the patient’s health and the
quality of life generally. Therefore, this questionnaire
has 26 questions overall. Scores for each aspect would
be between four and 20 that score four shows the worst
and 20 shows the best condition. These scores are con-
vertible to another score with the domain of 0-100 (Deh-
ghan et al., 2016).Persian version of this questionnaire
was prepared by Nedjat et al. and it has good validity
and reliability for evaluating QOL in the Persian speak-
ers (Nedjat et al 2008).To ll out the questionnaire for
illiterate patients trained people was used. The
study was
approved by the Ethics Committee of Fasa University of
Medical Sciences and all the participants signed a writ-
ten informed consent (Approval number: 26492/A/28).
The protocol of the study was approved by the Institu-
tional Review Board of the University.
STATISTICAL ANALYSIS
All the statistical analyses were performed using the sta-
tistical package for social sciences version 16.0 (SPSS
16). Descriptive results were expressed as mean value
± standard deviation. Qualitative data were expressed
by frequency and relative frequency. One way ANOVA
and Mann Whitney test were used for comparing the
scores of quality of life dimensions between the differ-
ent groups.
RESULTS
Overall, we enrolled 147 patients (3 of 150 excluded
during the study) including 77 (52.3 %) males and 70
(47.7 %) females referring to internal clinic and CCU
ward of Vali-Asr hospital (Fasa, Iran). The mean age of
patients was 63± 27 years. Demographic data is availa-
ble in Table.1.Also the quality of life dimensions of heart
failure patients has been shown in Table 2. Physical,
psychological, social, and environmental are all aspects
of WHO quality of life questionnaire that is scored in
this table.
Past medical history of hypertension, diabetes mel-
litus, chronic obstructive pulmonary disease, renal
failure, and pulmonary hypertension of patients
were extracted and each questionnaire variables were
assessed with them, but there was not any signi cant
relationship. (P-value = 0.40, 0.14, 0.50, 0.77, and 0.91,
respectively).
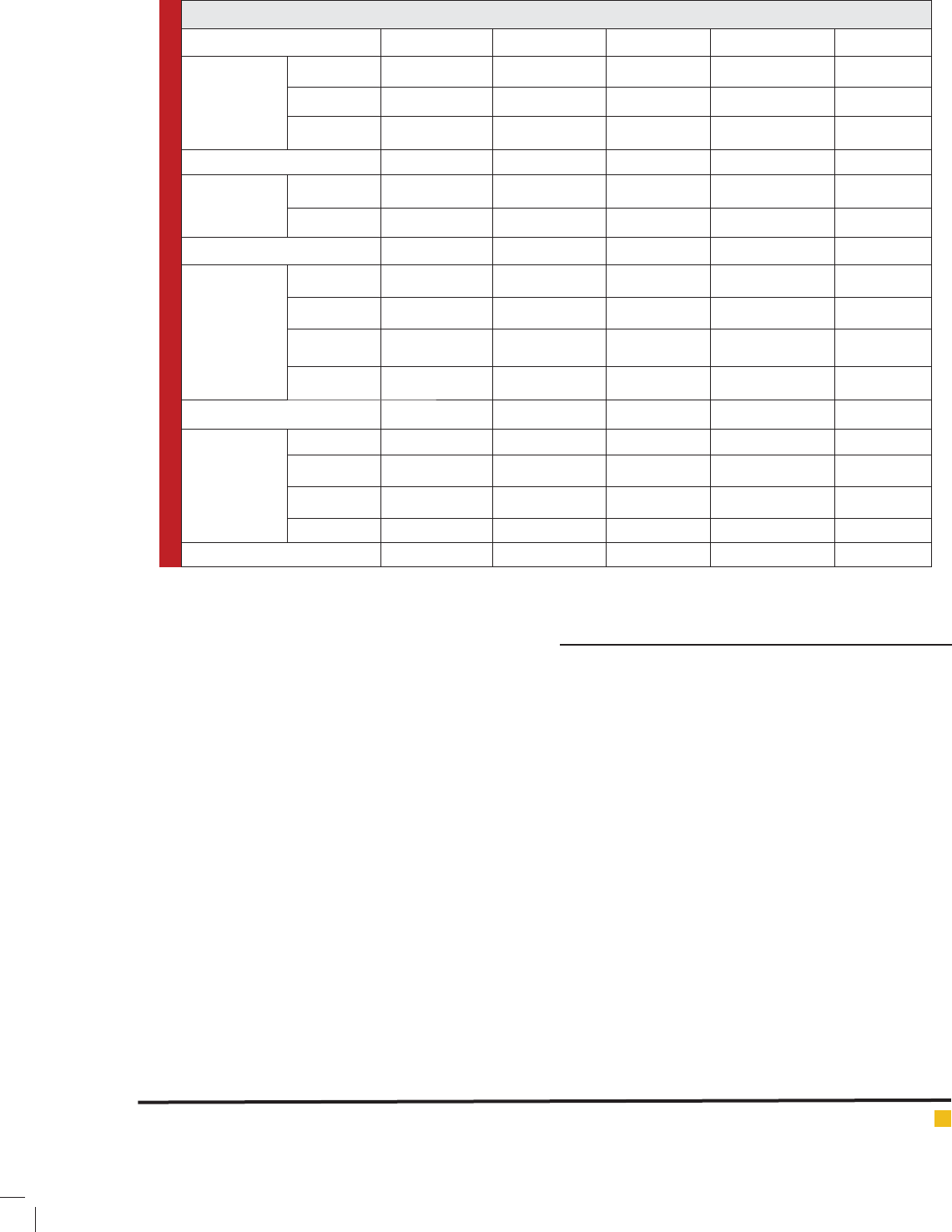
The scores of the questionnaire dimensions and their
correlation with age, sex, education, and stage of heart
failure is summarized in Table 3.3. Ejection fraction of
the patients didn`t have any relationship with these vari-
ations (p-value = 0.61).There was not any correlation
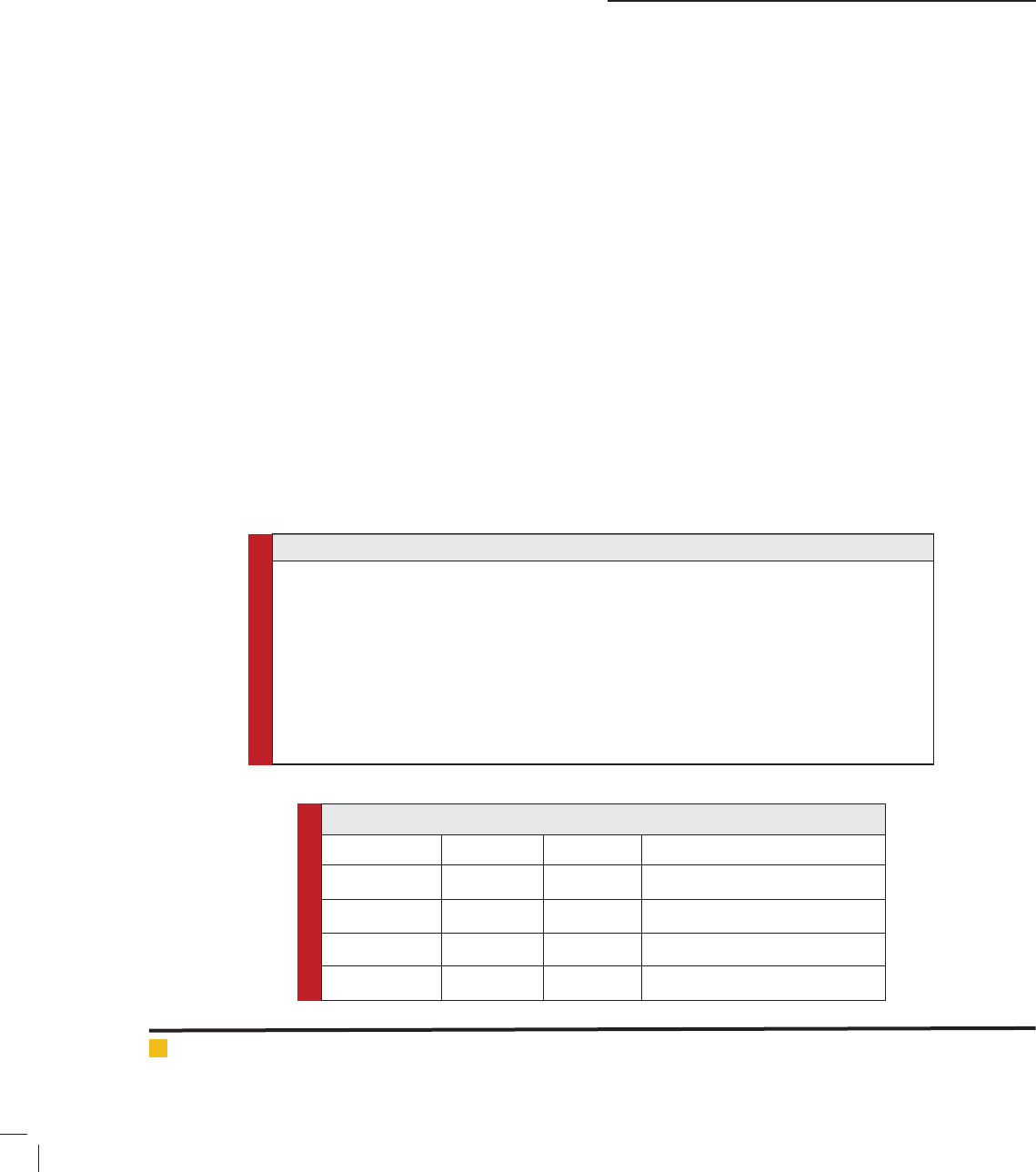
Table 1: Demographic data of heart failure patients
Variable Under 60
Frequency (%)
Between 60 and 70
Frequency (%)
More than 70
Frequency (%)
Age 45 (30.6) 37 (25.1) 65 (44.3)
Male
Frequency (%)
Female
Frequency (%)
Sex 77 (52.3) 70 (47.7)
Illiterate
Frequency (%)
Elementary 1
Frequency (%)
Elementary 2
Frequency (%)
Collegiate
Frequency (%)
Education 84 (57.1) 34 (23.1) 23 (15.6) 6 (4.2)
Table 2: Quality of life dimensions of patients with heart failure
Variable Minimum Maximum Mean ± Standard deviation
Physical 3.57 96.43 48.42±20.09
Psychological 12.50 83.33 49.97±14.99
Social 0.00 100.00 53.85 ±21.28
Environmental 6.25 90.63 45.74 ±17.67
880 FISH DIVERSITY OF WULAR LAKE KASHMIR INDIA BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
Mahshid Borumandpour
Table 3: Scores of questionnaire variations and their correlation with age, sex, education, and stage of heart failure
Variable Physical Psychological Social Environmental Total
Age < 60 49.76±18.51 48.98±15.96 54.62±20.37 46.73±15.91 51.38±27.72
60-70 50.09±19.73 49.77±14.59 54.95±16.71 43.15±16.48 37.16±26.59
> 70 46.53±21.44 50.76±14.71 52.69±24.25 46.53±19.50 46.53±27.99
P value 0.70 0.78 0.83 0.56 0.06
Sex Male 47.72±20.71 49.89±15.33 53.57±21.22 45.21±18.50 48.21±27.92
Female 49.18±19.50 50.05±14.71 54.16±21.50 46.33±16.83 42.85±27.79
P value 0.59 0.90 0.84 0.83 0.25
Education Illiterate 48.25±19.88 49.50±14.78 52.97±22.09 45.34±16.98 45.53±28.56
Elementary 1 45.90±22.41 50.61±14.61 54.41±22.95 44.76±20.10 44.85±24.25
Elementary 2 52.63±19.89 50.00±17.45 56.52±17.39 49.59±15.20 46.19±28.56
Collegiate 48.80±6.64 52.77±13.08 52.77±16.38 42.18±23.61 50.00±41.07
P value 0.69 0.89 0.86 0.67 0.98
Stage of heart
failure
Stage 1 30.35±19.45 50.00±10.20 37.50±27.63 37.50±22.24 50.00±20.41
Stage 2 49.72±17.58 49.35±14.27 53.52±21.10 47.71±18.44 45.19±28.95
Stage 3 47.46±19.39 50.29±15.53 53.75±20.11 45.40±16.83 47.25±28.01
Stage 4 56.30±25.45 49.01±14.77 58.82±26.42 46.69±21.17 36.02±27.20
P value 0.18 0.96 0.52 0.77 0.50
between NYHA class of patients and their quality of life
aspects, neither (p-value = 0.34)
Moreover, there was not any correlation between the
job of patients and any aspect of their quality of life
(p-value = 0.49 for total). Number of hospital admis-
sion days of patients and variations of questionnaire
were also compared with each other. None of them had
correlation with hospital staying days of the patients.
(P-value = 0.06 for physical, p-value = 0.17 for psy-
chological, p-value = 0.07 for social, p-value = 0.87
for environmental, and P-value = 0.69 for total). It is
obvious that if our sample size was much more, scores
of physical and social aspect of heart failure quality of
life might be signi cantly correlated with hospital stay-
ing days of the patients. Patients who underwent selec-
tive coronary angiography and coronary artery bypass
graft operation did not have any signi cant correlation
with any dimensions of quality of life questionnaire
(p-value= 0.49 and 0.85, respectively). In patients who
underwent percutaneous intervention environmental
aspect and total score of questionnaire were correlated
with this intervention. (P-value= 0.014 for environmen-
tal and p-value= 0.023 for total)
DISCUSSION
Access to the information about the quality of life,
moreover to treatment, promote supportive programs
and rehabilitation proceedings in many societies. Today,
people are demanding improved quality of life that
is why the governments are increasingly focusing on
improving the quality of life of their people and are try-
ing to reduce disease; they also secure health services,
physical, mental, and social welfare for their popula-
tion (Park, Sands, & Marek, 1995).We found in our study
that the score of all the aspects of patients’ quality of
life are in relatively desirable spectrum. Maximum score
belonged to social dimension of the heart failure quality
of life questionnaire. According to many researchers, the
majority of heart failure patients have an undesirable
life quality (Jaarsma et al., 2000) (Juenger et al., 2002)
(Wielenga et al., 1998). Also it has been declared that
congestive heart failure occurs more than other chronic
diseases, which disturb patients` quality of life (Cline
et al 1999).
In our study, we reached to this theory that the qual-
ity of life of younger patients is much better than elderly
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS APPLICATION OF WHOQOL-BREF FOR THE EVALUATION OF HEART FAILURE 881
Mahshid Borumandpour
patients. In other words, patients under 60 years old had
better life quality. Shojaie (2008) also stated that patients
between 40 to 60 years old have much desirable quality
of life than other age spectrums especially elderly peo-
ple. Moreover Stewart et al. 2008) stated that males have
a better quality of life but we didn`t see any signi cant
difference between males and females quality of life in
our study. In another study the comparison of the qual-
ity of life dimensions in women and men showed that
physical function (P=0.005) and mental health (P=0.01)
were signi cantly higher in men than women (Abedi
et al 2011).
Perhaps the main cause of these ndings is as follows:
Men are very active people in the period before being
retired; but they af icted to heart failure in the years
after this section of life. While majority of women in
this survey are homemakers and notwithstanding suffer-
ing from chronic diseases. This task dramatically reduces
their quality of life. Riedinger et al (2006) performed a
cross-sectional study and found that women do much
less exercise than men that this leads to a decrease in
functional capacity and deterioration of their physical
condition and nally affects their quality of life (Ried-
inger et al 2002).
In the present study, the quality of life of the patients
older than 70 years old are so low and this quality
became worsen with the increasing age. Johansson et
al. ( 2006) and Shojaie ( (2008) concluded similar conse-
quences but Rahnavard et al., (2006) did not found any
signi cant correlation between the age and the qual-
ity of life of heart failure patients. Level of education
by establishing fundamental change in knowledge and
attitude has always been effective in health, disease, and
all aspects of human life. It is also considered as a factor
affecting the quality of life of patients in many previous
studies. We found in the present study that heart failure
patients with college education have much more desir-
able quality of life than other groups. In other words, the
higher the educational level, the more favorable quality
of life the patient will have. This theory has been proven
in some other studies (Rahnavard et al., 2006) (Esmaeili,
2004; Shojaei, 2008).Percentage of ejection fraction is
the ratio of end-diastolic volume of blood in each con-
traction that exited from heart chambers and is affected
in heart failure. We did not nd any correlation between
the amount of ejection fraction and the quality of life
of patients but Juenger et al (2002) expressed that with
increase in the severity of heart disease and decrease
in ejection fraction, the quality of life will be signi -
cantly decreased. They also expressed that the percent-
age of ejection fraction is a measure of heart function
and its reduction demonstrates the disease severity.
Another variation that affects the quality of life of these
patients is the stage of heart failure. The stage of heart
failure shows the severity of the disease and represents
the responsibility of patients to our treatment package.
In our study, patients were divided into four groups
according to the stage of their disease. The scores of the
quality of life questionnaire in stage four of heart failure
were less than other groups.
Interventions are some actions that in uence on all
aspects of life especially its quality. Percutaneous inter-
vention is an invasive intervention that may affect the
quality of life of heart failure patients. Our results also
revealed that patients who underwent this intervention
in course of their disease had lower scores of the ques-
tionnaire dimensions than patients without any inter-
vention. We think that some of our results and com-
parisons were unstable due to small sample size of the
study. We suggest to choose a bigger sample in future
studies in order to evaluate heart failure patients` qual-
ity of life more exactly. The burden of the disease on
patients, their family, and society are some related vari-
ations that could be assessed in next studies. Our results
indicated that the majority of heart failure patients had
poor and undesirable quality of life and the women have
weaker scores of quality of life variations than men.
Therefore, controlling some available variables among
these patients is suggested.
ACKNOWLEDGMENT
This article is the result of medical student theses In Fasa
University of Medical Sciences, Iran. We appreciate the
deputy of research and technology of Fasa University of
medical sciences for supported this research.
REFERENCES
Abedi, H. A., Yasaman A. M. and Abdeyazdan G. H. (2011).
Quality of life in heart failure patients referred to the Kerman
outpatient centers, 2010.
Cline, C. M., Willenheimer, R. B., Erhardt, L. R., Wiklund, I., &
Israelsson, B. Y. (1999). Health-related quality of life in elderly
patients with heart failure. Scandinavian Cardiovascular Jour-
nal, 33(5), 278-285.
Dehghan, A., Ghaem, H., Borhani-Haghighi, A., Safari-Far-
amani, R., Moosazadeh, M., & Gholami, A. (2016). Evaluation
of reliability and validity of PDQ-39: questionnaire in iranian
patients with parkinson’s disease. Zahedan Journal of Research
in Medical Sciences, 18(3).
Dehghan, A., Ghaem, H., Borhani Haghighi, A., Kash , S., &
Zeyghami, B. (2011). Comparison of quality of life in Parkin-
son’s patients with and without fatigue. Bimonthly Journal of
Hormozgan University of Medical Sciences, 15(1), 49-55.
Dunderdale, K., Thompson, D. R., Miles, J. N., Beer, S. F., &
Furze, G. (2005). Quality‐of‐life measurement in chronic heart
882 FISH DIVERSITY OF WULAR LAKE KASHMIR INDIA BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS

Mahshid Borumandpour
failure: do we take account of the patient perspective? Euro-
pean journal of heart failure, 7(4), 572-582.
Ebrahimi Tabas , E., Khamrani, M., Rezvani Amin, M., & Pour-
namdar, Z. (2007). Quality of life and related factors in patients
with heart failure in CCU wards of Khatam the (PBUH) and Ali
Ibn Abi Talib (AS) hospitals in Zahedan. 21-22.
Esmaeili, M. (2004). Self-care self-ef ciency and quality of life
among patients receiving homedialysis.
Gholami, A., Jahromi, L. M., Zarei, E., & Dehghan, A. (2013).
Application of WHOQOL-BREF in measuring quality of life in
health-care staff. International journal of preventive medicine,
4(7).
Jaarsma, T., Halfens, R., Tan, F., Abu-Saad, H. H., Dracup, K.,
& Diederiks, J. (2000). Self-care and quality of life in patients
with advanced heart failure: the effect of a supportive educa-
tional intervention. Heart & Lung: The Journal of Acute and
Critical Care, 29(5), 319-330.
Johansson, P., Dahlström, U., & Broström, A. (2006). Factors
and interventions in uencing health-related quality of life in
patients with heart failure: a review of the literature. European
Journal of Cardiovascular Nursing, 5(1), 5-15.
Juenger, J., Schellberg, D., Kraemer, S., Haunstetter, A., Zugck,
C., Herzog, W., & Haass, M. (2002). Health related quality of
life in patients with congestive heart failure: comparison with
other chronic diseases and relation to functional variables.
Heart, 87(3), 235-241.
Kash , S. M., Nasri, A., Dehghan, A., & Yazdankhah, M. (2015).
Comparison of quality of life of patients with type II diabetes
referring to diabetes association of Larestan with Healthy peo-
ple in 2013. J Neyshabur Univ Med Sci, 3(2), 32-38.
Lloyd-Jones, D., Adams, R., Carnethon, M., De Simone, G., Fer-
guson, T. B., Flegal, K., . . . Greenlund, K. (2009). Heart disease
and stroke statistics—2009 update a report from the American
Heart Association Statistics Committee and Stroke Statistics
Subcommittee. Circulation, 119(3), e21-e181.
Mårtensson, J., Dracup, K., Canary, C., & Fridlund, B. (2003).
Living with heart failure: depression and quality of life in
patients and spouses. The Journal of heart and lung transplan-
tation, 22(4), 460-467.
McMurray, J., & Stewart, S. (2002). The burden of heart failure.
European Heart Journal Supplements, 4(suppl D), D50-D58.
Molloy, G. J., Johnston, D. W., & Witham, M. D. (2005). Family
caregiving and congestive heart failure. Review and analysis.
European journal of heart failure, 7(4), 592-603.
Nedjat, S., Montazeri, A., Holakouie, K., Mohammad, K., &
Majdzadeh, R. (2008). Psychometric properties of the Iranian
interview-administered version of the World Health Organiza-
tion’s Quality of Life Questionnaire (WHOQOL-BREF): a popu-
lation-based study. BMC health services research, 8(1), 1.
Park, W., Sands, J., & Marek, J. (1995). Medical surgical nurs-
ing: Concepts and clinical practice. St. Louis: Mosby, 17.
Rahnavard, Z., Zolfaghari, M., Kazemnejad, A., & Hatamipour,
K. (2006). An investigation of quality of life and factors affect-
ing it in the patients with congestive heart failure. Journal of
hayat, 12(1), 77-86.
Rahnavard , Z., Zolfaghari, M., Kazermnejad, A., & Hatamipour,
K. (2006). An investigation of aulity of life and factors affect-
ing it in the patients with congestive heart failure. Journal of
Hayat, 77-86.
Riedinger, M. S., Dracup, K. A., Brecht, M.-L., & Investigators,
S. (2002). Quality of life in women with heart failure, norma-
tive groups, and patients with other chronic conditions. Amer-
ican Journal of Critical Care, 11(3), 211-219.
Shojaei, F. (2008). Quality of life in patients with heart failure.
Journal of hayat, 14(2), 5-13.
Stewart, S., & Blue, L. (2008). Improving outcomes in chronic
heart failure: a practical guide to specialist nurse intervention:
John Wiley & Sons.
Wielenga, R. P., Erdman, R. A., Huisveld, I. A., Bol, E., Dun-
selman, P. H., Baselier, M. R., & Mosterd, W. L. (1998). Effect
of exercise training on quality of life in patients with chronic
heart failure. Journal of psychosomatic research, 45(5), 459-
464.
Zambroski, C. H., Moser, D. K., Bhat, G., & Ziegler, C. (2005).
Impact of symptom prevalence and symptom burden on qual-
ity of life in patients with heart failure. European Journal of
Cardiovascular Nursing, 4(3), 198-206.
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS APPLICATION OF WHOQOL-BREF FOR THE EVALUATION OF HEART FAILURE 883