
Unacceptable status of oral and dental health-related
knowledge among Iranian primary school students
Ghaffari Mohtasham
1
, Nasirzadeh Mostafa*
2
, Rakhshanderou Sakineh
3
and
Ramezankhani Ali
4
1Associate Professor, Department of Public Health, School of Public Health, Shahid Beheshti University of
Medical Sciences, Tehran, Iran
2Ph.D Candidate in Health Education and Health Promotion, Assistant Professor, Department of Public
Health, School of Public Health, Shahid Beheshti University of Medical Sciences, Tehran, Iran
3Assistant Professor, Department of Public Health, School of Public Health, Shahid Beheshti University of
Medical Sciences, Tehran, Iran
4Professor, Department of Public Health, School of Public Health, Shahid Beheshti University of Medical
Sciences, Tehran, Iran
ABSTRACT
Oral health as one of the health Criteria of people plays key role in general health. For improvement of oral health, it is necessary
to measure the knowledge level. This study has investigated the Oral health- related knowledge among Rafsanjan City Primary
Schools’ Students. The present descriptive-analytical study has been conducted on 429 primary students (second grade) in Rafsan-
jan, Iran. Samples are selected using random cluster sampling. Data collection method is the researchers’ questionnaire containing
24 items and that validity and reliability was respectively obtained through using opinions of experts and content validity and
test-retest method and extraction of Cronbach’s alpha. After collecting the data, the data are analyzed using SPSS-21 software
using independent t-test, one-way ANOVA and Pearson correlation at the signi cance level of 0.05.Mean score of knowledge of
students is 10.24±3.1 of 24 and 69% of students had knowledge in average level. The most important weakness points included
knowledge of students about mental, psychological and social complications of inadequate oral and dental health. Signi cant
correlation was between knowledge and education of parents and description of oral and dental health status of students excel-
lently and the variable of reporting regular brushing status.Making behavior needs increasing knowledge and changing attitude
in people. Despite to the advancements and communicative technologies, knowledge level of students is in undesirable, low and
unacceptable level. Hence, it would be better to arrange and announce required policy making to design intervention plans.
KEY WORDS: ORAL AND DENTAL HEALTH, KNOWLEDGE, STUDENTS
260
ARTICLE INFORMATION:
*Corresponding Author: mnasirzadeh13@yahoo.com
Received 27
th
Dec, 2016
Accepted after revision 2
nd
March, 2017
BBRC Print ISSN: 0974-6455
Online ISSN: 2321-4007
Thomson Reuters ISI ESC and Crossref Indexed Journal
NAAS Journal Score 2017: 4.31 Cosmos IF : 4.006
© A Society of Science and Nature Publication, 2017. All rights
reserved.
Online Contents Available at: http//www.bbrc.in/
Biosci. Biotech. Res. Comm. Special Issue No 1:260-266 (2017)
Ghaffari Mohtasham et al.
INTRODUCTION
Oral and dental health is one of the main health criteria
of the society and plays key role in general health and
quality of life of people and can affect overall public
health (1, 2). In most countries of the world, spread of
oral and dental diseases like Oral Cancer is reported 1-10
cases per 100 thousand people and tooth decay is also
the most common disease across the world and about
100% of adults suffer from it. Moreover, spread of the
disease is reported to 60-90% among school children,
(Daly and Batchelor 2012, WHO 2012, Nurelhuda et al
2009)
Oral and dental diseases like decay and periodontitis,
similar to systemic diseases, have chronic process and
similar behavioral features and multifactorial nature (4).
Urbanization, industrial and mechanized life, change in
nutrition style and poor eating habits, smoking, tobacco
and alcohol are the main factors causing increase in
tooth decay and gum disease. Other factors affecting
oral and dental diseases include change in lifestyle, lim-
ited children’s access to oral care services, social sta-
tus, knowledge, personality and attention to their own
health, poor diet such as eating too much sugar and gen-
erally, no observance of oral and dental hygiene (lack
of brushing and no ossing. In general, 4 main factors
creating decay include germs, sugar, teeth resistance and
time, (Maltz et al., 2010,Liu et al., 2009 Antonio et al.,
2007, Al Subait et al., 2016, Çolako
˘
glu and Has 2015
Castilho et al., 2015).
Oral and dental diseases can result in various compli-
cations including chewing food disorders, gastrointesti-
nal problems, bad breath, major social problems, cancer
and oral carcinomas and reduced life expectancy, speech
problems, mental disorders, in ammation of the gums,
tooth irregularity, low self-esteem, poor quality of life,
impaired nutritional status, reducing the growth of chil-
dren, the loss of more than 50 million hours of school
curriculum (10-15).
Torabi et al., 2009, Zeidi et al., 2013, Morowatishari-
fabad et al., 2011, Rahimi et al., 2011) Feldens et al., 207
and Peterson et al., 2008).
The most important strategies of WHO to prevent the
problems and to improve oral and dental health include
reducing load of unacceptable oral and dental health-
related disorders, promoting healthy lifestyles and
reducing risk factors (environmental, economic, social
and behavioral), development of health service provider
systems and arrangement of policies to promote oral and
dental health, WHO (2015).
The only effective and ef cient strategy to solve
problems related to oral and dental health is prevention
and various collections of activities in individual, job
and social level WHO (2015).
For effective improvement of oral and dental health-
related behaviors and planning in this eld, people
should have complete and comprehensive information
about factors affecting decision making, assessment
of nutrition status, measurement of public knowledge,
evaluation of health status and information, size of
tooth decays, assessing the status of self-case behaviors,
brushing and ossing, (Pakpour et al 2011 Pishva and
Asefzadeh 2010).
One of the most important and also initial steps in
eld of the process of changing behavior is assessing
knowledge in this eld and such knowledge can pave
the way for formation of attitude and improvement of
behavior. Studies have reported high level of knowledge
of children in eld of oral and dental health. Gao et
al (2014) has reported the amount of spread of tooth
decay among 12-15 years old children to 24% and has
also reported knowledge of students in undesirable level
and has reported no signi cant correlation between the
two variables. The status of this index is also reported
in undesirable level in Iranian children (Moeini et al.,
2013). For example, Moeini et al (2013) have studied the
knowledge level of primary students of Sanandaj to 8.5
of 20 and in undesirable level and have claimed that it
can pave the way for formation of other attitude vari-
ables such as sensitivity and perceived intensity. But
most of these studies have not analyzed the weaknesses
of children’s knowledge.
Children and adolescents are the large capital sources
and the most valuable resources of a society and the
more the society tries to save the resources, the society
can be more successful and healthy in future. Therefore,
according to role of knowledge in formation of behav-
ior, this study has been conducted with the purpose of
determining the knowledge level of students as one of
the determinants of behavior and Analysis of strengths
and weaknesses in eld of oral and dental health.
MATERIALS AND METHODS
The descriptive-analytical study has been conducted on
429 primary students of second period (fourth, fth and
sixth grade) in Rafsanjan (6 schools; 3 for girls and 3
for boys). Sampling is done using cluster sampling and
classes in each school are selected randomly. Data col-
lection instrument is formed of 2 parts of demographic
questions (9 questions) and researchers’ questionnaire
(using review of studies and scienti c references). Valid-
ity of the questionnaire was measured based on opinion
of 10 experts and adjustment of the results with Lavs-
heh table using test-retest approach among 57 students
and the Cronbach’s alpha was obtained to 0.74. Number
of questions in second part on measuring knowledge
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS UNACCEPTABLE STATUS OF ORAL AND DENTAL HEALTH-RELATED KNOWLEDGE 261
Ghaffari Mohtasham et al.
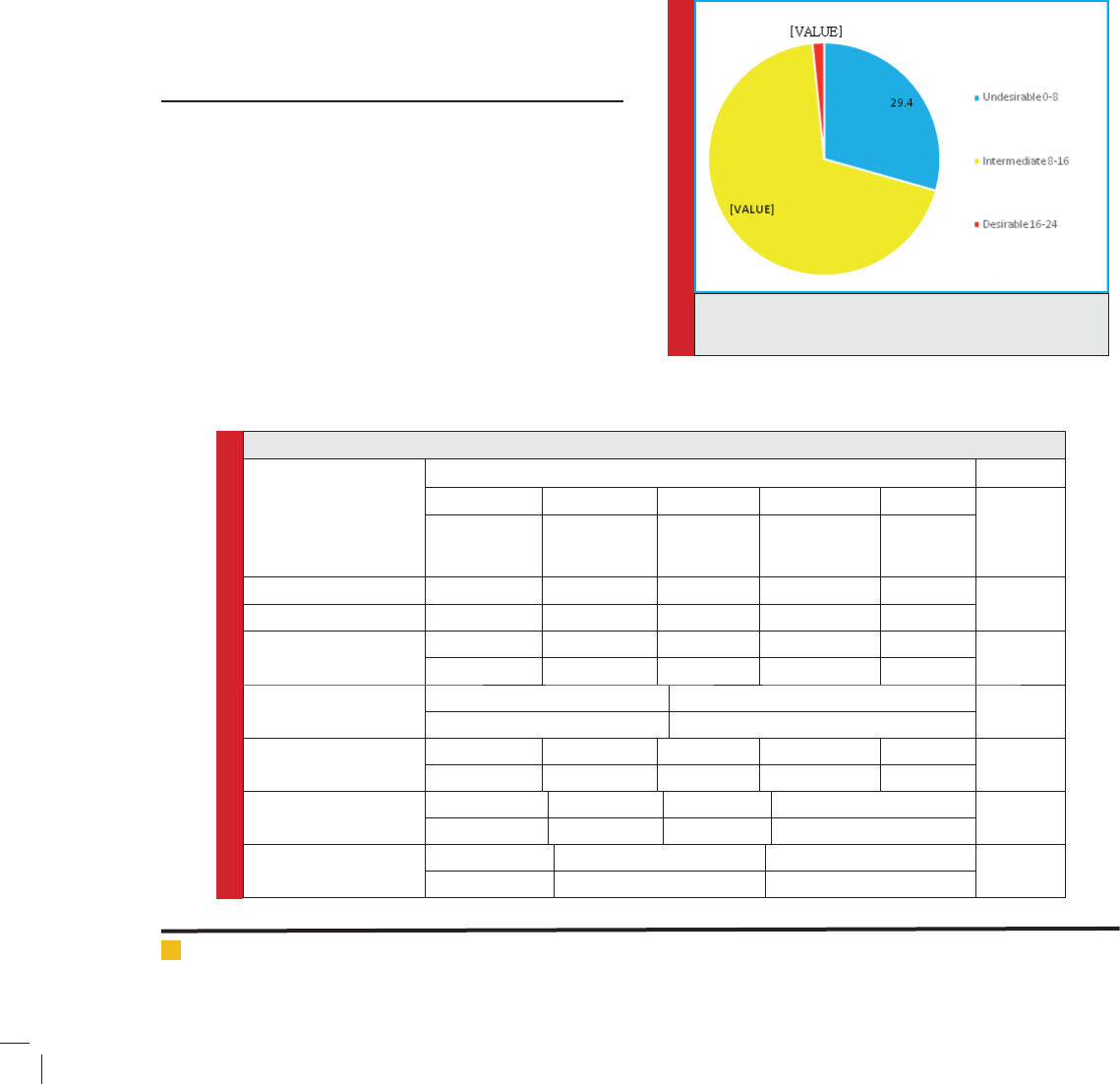
FIGURE 1. Frequency distribution of the state of
knowledge
of students includes 24 items, in which 11 questions
are 3-option for (true, false and I do not know) and 13
questions are 4-option items with self-report answering
method and with score range of (0-24). The true answers
were scored with point 1, false and I do not know answer
were scored with point 0. The inclusion criterion in this
study was the consent of participants and exclusion cri-
terion was incomplete responding to the questions. The
data processing and analysis was done using SPSS-21
software and using independent t-test, one-way ANOVA
and Pearson Correlation at the signi cance level of 0.05.
In terms of ethical considerations in this study, one can
refer to being ensured of secrecy and privacy of infor-
mation and anonymity of questionnaires, presenting the
results to the relevant parties, preservation of material
and spiritual rights of research team and considering the
contrast of interests of research team members.
RESULTS
The number of participants was 429 students (179 girls
and 250 boys). Education level of about one third of par-
ents was diploma and about 40% of fathers had free jobs
and 65.7% of mothers were housekeeper. About 17% of
participants reported excellent level of oral and dental
health and 45% reported that they brush their teeth reg-
ularly. The highest level of knowledge was reported in
student in sixth grade and the difference between classes
was signi cant (p<0.001) (table 1). Mean score knowl-
edge of students was 10.24±3.1 of 24 and only Less than
2% of students had desirable and acceptable knowl-
edge level ( gure 1). Mean score of knowledge level
was equal to 11±2.9 for girls and to 9.6±3.2 for boys
and the difference between two groups was signi cant
(p<0.001). In this study, no signi cant correlation was
observed between mean score of knowledge level of stu-
dents with age and parent’s job (P>0.05). However, there
was signi cant correlation between higher education
(academic education) of parents and description of oral
and dental health status and report of regular brushing
(P<0.01). Educational needs based on analysis of items
in the questionnaire are reported in table 1. As it is clear,
3 preferred educational needs of students are in eld
of knowledge in eld of beginning time of observing
Table 1. Distribution of demographic characteristics of students and its relationship with knowledge
Variable
variable modes P- Value
Illiterate Elementary Guidance Diploma Academic
P=0.03
Number
(Percent)
Number
(Percent)
Number
(Percent)
Number
(Percent)
Number
(Percent)
Father’s education 6 (1.6) 26 (7) 67 (18.2) 155 (42) 115 (31.2)
P=0.001
Mother’s education 2 (0.5) 41 (11) 59 (15.9) 149 (40.1) 131 (32.5)
Father’s job Unemployed Worker Employee Self-employed Retired
P=0.1
8 (1.9) 59 (14.1) 160 (38.5) 173 (41.6) 16 (3.8)
Mother’s job Housewife Employed
P=0.08
282 (65.9) 146 (34.1)
Describe the state of oral
health
Excellent Very good Good Average Weak
P<0.001
75 (17.7) 90 (21.2) 156 (36.8) 88 (20.8) 15 (3.5)
Describe the brushing Never Rarely Sometimes Regularly & Always
P=0.002
13 (3) 30 (7) 189 (44.1) 197 (945.9)
Grade Fourth (M±D) Fifth (M±D) Sixth (M±D)
P<0.001
9.5±3 10.5±3.2 11.03±3.06
262 UNACCEPTABLE STATUS OF ORAL AND DENTAL HEALTH-RELATED KNOWLEDGE BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
Ghaffari Mohtasham et al.
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS UNACCEPTABLE STATUS OF ORAL AND DENTAL HEALTH-RELATED KNOWLEDGE 263
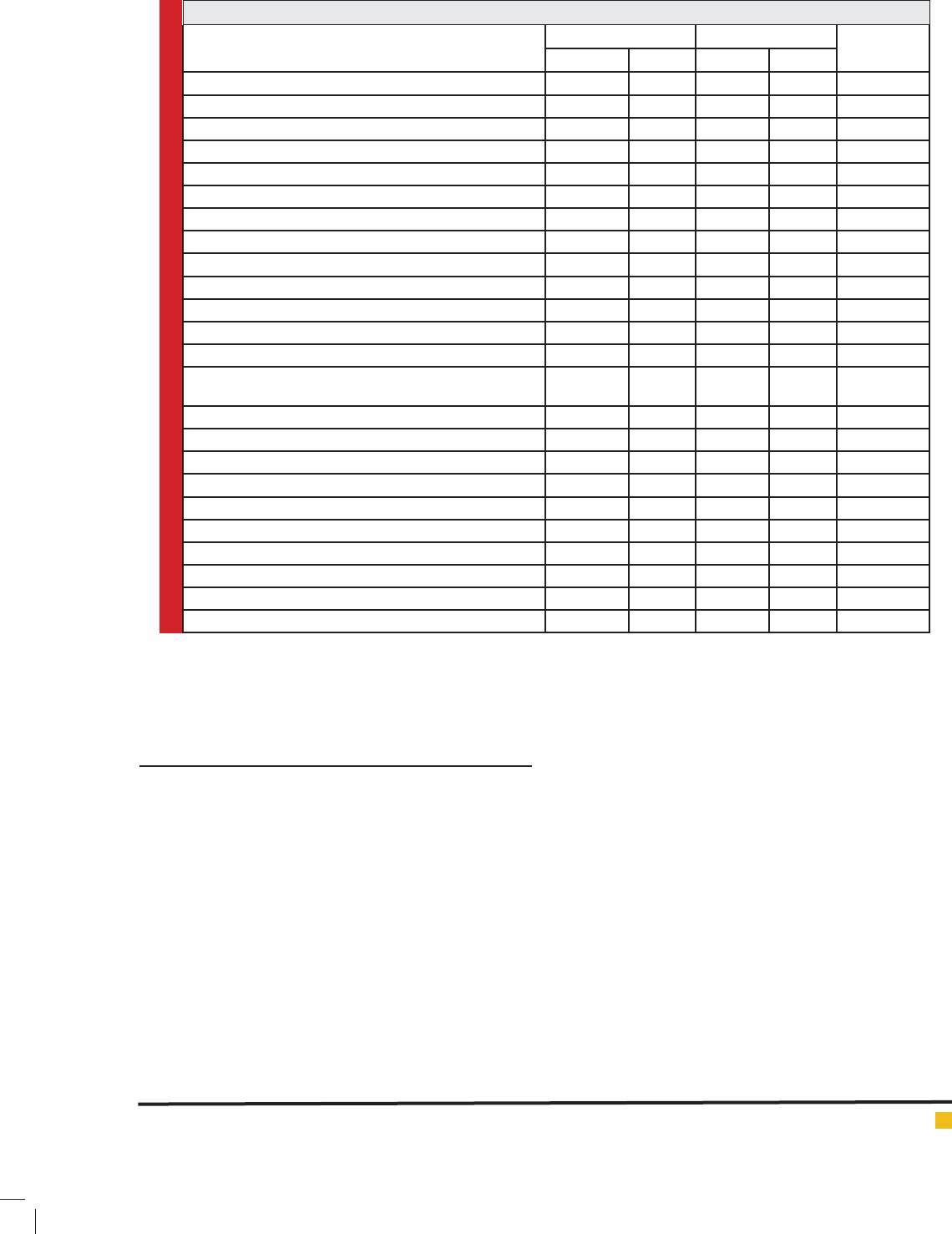
Table 2. check the status of responding to awareness questions and education priorities
questions Correct answers Incorrect answers Educational
priority
Number Percent Number Percent
the time of beginning observance of oral and dental hygiene 26 6.1 403 93.9 1
Mental complications of tooth decay (being ashamed, etc.) 49 11.4 380 88.6 2
right time to change the brush 60 14 369 86 3
right time to appoint a dentist for examination 89 20.7 340 79.3 4
least times of using oss per day 91 21.2 338 78.8 5
minimum brushing time 99 23.1 330 76.9 6
time of using mouthwash in children 106 24.7 323 75.3 7
type of teeth and their effect on decay 112 26.1 317 73.9 8
dental sensitivity to heat and cold (a sign of decay) 113 26.3 316 73.7 9
brushing style of outer surface of upper teeth 117 27.3 312 72.7 10
toothache or bleeding while brushing (a sign of decay) 151 35.2 278 64.8 11
task of teeth in speaking 181 42.2 248 57.8 12
the amount of using toothpaste in children 185 43.1 244 56.9 13
the time that food residuals remain on tooth and its effect on
decay
205 47.8 224 52.2 14
frequency of brushing behavior in day and night 222 51.7 207 48.3 15
the best way to clean the space between teeth 237 55.2 192 44.8 16
physical complications of decay (bad breath, etc.) 250 58.3 179 41.7 17
germs and their impact on decay 272 63.4 157 36.6 18
sugar and its impact on decay 281 65.5 148 34.5 19
task of teeth in protecting face beauty 286 66.7 143 33.3 20
brown and black spots on tooth (a sign of decay) 292 68.1 137 31.9 21
right times of brushing 295 68.8 134 31.2 22
task of teeth in chewing food 297 69.2 132 30.8 23
the time of beginning observance of oral and dental hygiene 377 87.9 52 12.1 24
oral and dental hygiene, mental complications of tooth
decay and the right time to change the brush.
DISCUSSION
Undoubtedly, to arrange interventions and educational
plans, comprehensive recognition of determinants of the
behavior is required, so that the arranged planning and
intervention could have the highest effect and result.
One of the most important and initial steps in eld of
process of changing behavior is measurement of knowl-
edge of individuals in eld of the studied issue. In this
study, mean value of total knowledge level of students
is obtained to 10.24±3.1 of 24 and majority had unac-
ceptable knowledge level. In other studies, knowledge
level of students was reported in weak level (Paula et
al., 2013). In a study conducted by Haleem et al (2013),
mean score of knowledge level of 10-12 years old stu-
dents in eld of oral and dental health was reported to
2.5 from12.
About 95% of students in this study reported that the
beginning time of oral and dental health behaviors was
from eruption time. It is necessary to provide required
information for them and their families in eld of obser-
vance of oral and dental health before eruption time.
Majority of the students were aware of physical com-
plications of lack of observing oral hygiene; although
majority of them were unaware of mental and psycho-
logical complications and social complications like self-
con dence, being ashamed and losing friends. This issue
is one of the most important issues to make children
sensitive and pave the way for them to begin oral health
behaviors, since having information about outcomes of
a phenomenon can lead to formation of attitudes and
encouraging children to take health behaviors. In the
study of Haleem A, it was reported that children have
unacceptable knowledge in eld of complications of no
observance of oral and dental health Haleem et al (2013).
Therefore, it is suggested to planners and designers of
intervention plans to consider this issue seriously, so
that the sensitivity of perceived intensity is formed in
Ghaffari Mohtasham et al.
264 UNACCEPTABLE STATUS OF ORAL AND DENTAL HEALTH-RELATED KNOWLEDGE BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
children to take healthy, rapid and sustainable behav-
iors. In this study, the students had acceptable knowl-
edge level about functions of teeth; although more than
half of them were unaware of tasks of teeth and their
role in speaking. Their knowledge in this eld can pave
the way to encourage them to take preventive behaviors.
Another issue to encourage children to take preven-
tive behaviors is having knowledge about the factors
creating tooth decay. According to report of WHO, 4
factors including sugar, germs, resistance and time (the
time that food remains in mouth) can affect teeth decay.
The knowledge of students about effects of sugar and
germs on decay was acceptable; although it was unac-
ceptable in eld of effect of type and resistance of teeth
and time. Knowledge of children about the philosophy
of teeth decay and role of important variable like time
and the time that food remains on teeth can be one of
the most effective factors in brushing behavior and these
results are in consistence with ndings of Gao et al.
(2014) reported signi cantly unacceptable knowledge of
12-15 years old children in eld of spread of teeth decay
and reported the value about 24% for it and mentioned
that this variable is one of the most effective variables in
decay and dental diseases.
In this study, variables such as brown and black and
white spots on teeth and dental sensitivity to heat and
cold, gum bleeding and perforated teeth are investigated
that are counted as signs of teeth decay in other studies
(Herendon et al., 2010). The knowledge of majority of
students about these signs was poor. However, aware-
ness of signs of decay and examination of these signs
by the person can be the most important factor encour-
aging in eld of formation of beliefs and intention of
behavior and pave the way for seriously formation of
preventive behaviors and urgent referral to dentist to get
preventive services in secondary level. In other studies,
insuf cient knowledge of children about signs of teeth
decay is reported.
Al-Darwish (2016) has reported in a study that only
25% of 12-14 year old students in Qatar have accept-
able knowledge level in eld of oral and dental health.
The students have poor knowledge about variables such
as decay signs, regular appointment of dentist with the
purpose of care and examination, role of uoride and
consumption of sweet drinks and foods and plaque. Only
3.7% of children brush their teeth regularly after eat-
ing food and this has been in direct correlation with
formation of brushing behavior Al-Darwish (2016). The
suggestion here is to provide required empowerments to
introduce the signs of teeth decay to children, so that
self-care and control behaviors are facilitated.
Another weakness in eld of knowledge of children is
being unaware of information of a well-designed brush,
time of changing it, role and effect of toothpaste and
ossing on improvement of oral and dental health, refer-
ring to dentist for regular examinations. As formation
of behavior was growing and promotion of knowledge
level is at the beginning of this process, it seems nec-
essary to arrange and implement comprehensive plans
by health authorities like school-oriented interventions
and family-oriented intervention’s in eld of increasing
knowledge of students.
In this study, girls had higher knowledge and aware-
ness than boys and this was proved in the study con-
ducted by Al-Subait et al (2015). The reasons for this
issue could be more sensitivity of girls to health issues,
especially oral and dental health. Moreover, signi cant
correlation was observed between knowledge level of
students and some demographic variables such as edu-
cation level of parents and beliefs and wrong descrip-
tions of oral and dental health and the result has been
in consistence with ndings of other studies (Anne
et al., 2016).
In a study conducted by Nurdan and Ethem (2015),
social-demographic variables had direct and signi cant
effect on oral and dental health. In the study, the status
of germ plaque was signi cantly correlated to the moth-
er’s job, family income, insurance status, family mem-
bers, number of children, educational level of mother,
caregiver, supervision of parents on oral health of chil-
dren and regular appointment of dentist and brushing
behavior in parents. In the study conducted by Alin-
Rogeria et al (2013), variables such as parent’s behav-
iors, parent’s positive attitude, supervision and control
of parents on health behaviors of children are reported.
Hence, it is suggested to consider the family as the main
and the rst center for education of children.
LIMITATIONS OF THE STUDY
The limitations with the present study include the way
of answering questions (self-report) and the strengths
in this study include partial consideration of the issue
of knowledge and its orientations in eld of oral and
dental health, which can be helpful for the interventions.
CONCLUSION
Taking behavior needs improving knowledge and infor-
mation and changing attitudes of people towards each
eld and issue. The results obtained from this study
showed that despite to advancement of modern tech-
nologies and increased amount of communications, still
some issues such as oral and dental health and aware-
ness of the causes and complications of teeth decay,

Ghaffari Mohtasham et al.
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS UNACCEPTABLE STATUS OF ORAL AND DENTAL HEALTH-RELATED KNOWLEDGE 265
decay signs and preventive behaviors are in unaccepta-
ble and undesirable level and this can be the main rea-
son for lack of achievement to desirable indices among
students. Designing, implementing and valuating the
health interventions and promotion of health in eld of
oral and dental health is suggested to improve knowl-
edge and improve relevant behaviors.
ACKNOWLEDGMENTS
At the end, the author would like to appreciate authori-
ties in Shahid Beheshti University of Medical Sciences
Tehran and Rafsanjan, the Education and Training Min-
istry of Rafsanjan, managers of schools and the students
who helped implementation of this research project
under the code 8555 in Shahid Beheshti University of
medical Sciences extracted from Ph.D thesis.
CONFLICT OF INTEREST
There is no con ict of interest.
REFERENCES
Al Subait AA, Alousaimi M, Geeverghese A, Ali A, El Met-
wally A. Oral health knowledge, attitude and behavior among
students of age 10–18years old attending Jenadriyah festival
Riyadh; a cross-sectional study. The Saudi Journal for Dental
Research. 2016;7(1):45-50.
Al-Darwish MS. Oral health knowledge, behaviour and prac-
tices among school children in Qatar. Dental Research Journal.
2016;13(4):342.
Antonio A, Kelly A, Valle D, Vianna R, Quintanilha LE. Long-
term effect of an oral health promotion program for school-
children after the interruption of educational activities. Jour-
nal of Clinical Pediatric Dentistry. 2007;32(1):37-41.
Çolako
˘
g
lu N, Has L. A Research for People to Determine the
Relationship between Oral Hygiene and Socio-Economic Sta-
tus. Procedia-Social and Behavioral Sciences. 2015;195:1268-
77.
Daly B, Batchelor P, Treasure E, Watt R. Essential dental public
health: OUP Oxford; 2013.
de Castilho ARF, Mialhe FL, de Souza Barbosa T, Puppin-Ron-
tani RM. In uence of family environment on children’s oral
health: a systematic review. Jornal de Pediatria (Versão em
Português). 2013;89(2):116-23.
de Paula JS, Leite ICG, de Almeida AB, Ambrosano GMB,
Mialhe FL. The impact of socioenvironmental characteristics
on domains of oral health-related quality of life in Brazilian
schoolchildren. BMC oral health. 2013;13(1):10.
Feldens CA, Vítolo MR, Drachler MdL. A randomized trial of
the effectiveness of home visits in preventing early child-
hood caries. Community dentistry and oral epidemiology.
2007;35(3):215-23.
Gao J, Ruan J, Zhao L, Zhou H, Huang R, Tian J. Oral health
status and oral health knowledge, attitudes and behavior
among rural children in Shaanxi, western China: a cross-sec-
tional survey. BMC oral health. 2014;14(1):144.
Haleem A, Siddiqui MI, Khan AA. School-based strategies for
oral health education of adolescents-a cluster randomized con-
trolled trial. BMC oral health. 2012;12(1):54
Herndon JB, Tomar SL, Lossius MN, Catalanotto FA. Preventive
oral health care in early childhood: knowledge, con dence,
and practices of pediatricians and family physicians in Florida.
The Journal of pediatrics. 2010;157(6):1018-24.
Liu H-Y, Huang S-T, Hsuao S-Y, Chen C-C, Hu W-C, Yen Y-Y.
Dental caries associated with dietary and toothbrushing hab-
its of 6-to 12-year-old mentally retarded children in Taiwan.
Journal of Dental Sciences. 2009;4(2):61-74.
Maltz M, Jardim JJ, Alves LS. Health promotion and dental
caries. Brazilian oral research. 2010;24(1):18-25.
Mazloomi-Mahmoodabad S, Moein-Taghavi A, Barkhordari A,
Alidoosti F. Effect of role modeling through theater show in
oral health education. Majallah i Dandanpizishki (Journal of
Islamic Dental Association of Iran). 2009;21(2):138-42.
Moeini B, Ghaderi A, Hazavehei S, Allahverdipour H, Moghim-
beigi A, Jalilian F. A comparative study of peer education and
trainer education on the basis of health belief model (HBM) in
improving oral health in sanandaj boy’s elementary schools.
TOLOE- BEHDASHT 2013;12(2):1-13.
Morowatisharifabad M, Fallahi A, Nadrian H, Haerian A,
Neamatshahrbabaki B. Inter-dental cleaning behavior and its
relationship with psychological constructs based on the Tran-
stheoretical model. Oral Health Prev Dent. 2011;9(3):211-20.
Nurelhuda NM, Trovik TA, Ali RW, Ahmed MF. Oral health
status of 12-year-old school children in Khartoum state, the
Sudan; a school-based survey. BMC oral health. 2009;9(1):15.
Pakpour AH, Yekaninejad MS, Zarei F, Hashemi F, Steele MM,
Varni JW. The PedsQL™ Oral Health Scale in Iranian children:
reliability and validity. International Journal of Paediatric
Dentistry. 2011;21(5):342-52.
Petersen PE. World Health Organization global policy for
improvement of oral health‐World Health Assembly 2007.
International dental journal. 2008;58(3):115-21.
Pishva N, Asefzadeh S. Community intervention to modify
beliefs, traditions and practices of oral health in Yahya-Abad
village. The Journal of Qazvin University of Medical Sciences
2010;4(3):45-51.
Rahimi F, Shojaeezade D, Zeraati H, Akbarian M. Oral health
care based on educational health belief model in child. Journal
of Health. 2011;2(1):74-81.
Torabi M, Karimi AS, Sheykhzadeh A, Karimi AM. Assessment
of oral health indices in Kerman adults aged 35-44 years. Jour-
nal of Isfahan Dental School. 2009;5(2):93-8.

Ghaffari Mohtasham et al.
266 UNACCEPTABLE STATUS OF ORAL AND DENTAL HEALTH-RELATED KNOWLEDGE BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
World Health Organization (WH0), Oral health, Strategies and
approaches in oral disease prevention and health promotion
2015 [updated 2015-9-8; cited 2015]. Available from: http://
www.who.int/oral_health/strategies/cont/en/.
World Health Organization (WH0), Oral health, The objec-
tives of the WHO Global Oral Health Programme (ORH) 2015
[updated 2015-9-9]. Available from: http://www.who.int/oral_
health/objectives/en/.
World Health Organization (WHO), Oral health, Key facts 2012
[updated 2015Sep07; cited 2012 Apr7]. Available from: : http://
www.who.int/mediacentre/factsheets/fs318/en/.
Zeidi IM, Pakpour A, Zeidi BM. Effectiveness of educational
intervention based on transtheoretical model in promoting
oral health self-care behaviors among elementary students.
Journal of Isfahan Dental School. 2013;9(1):37.