
Investigating the effectiveness of play therapy
in improving cognitive-behavioral symptoms of
autistic disorder
Samira Hatami
1
and Fatemeh Rahmani
2
1
MA in General Psychology, Azad University of Torbat-e-Jam, Iran
2
Master of Clinical Psychology, Kharazmi University of Tehran, Iran
ABSTRACT
This study aims to determine the effectiveness of play therapy in improving cognitive-behavioral symptoms of
autism. The present research is a pretest-posttest quasi-experimental study design with two experimental and control
groups. The statistical population consists of all children with autistic disorder in Mashhad in the year 2009-2010. The
subjects (30 boy children with autism) were selected from Tabassom educational center for autistic children through
available sampling method and were randomly assigned into two experimental and control groups, each including
15 participants. To this end, a pretest was initially administered for both groups using Childhood Autism Rating
Scale (CARS) and then, play therapy was conducted for twelve 45-minute sessions with the experimental group and
nally, a posttest was implemented. In analyzing the data, analysis of covariance was applied. The research ndings
demonstrated that at the end of play therapy sessions, the experimental group compared to the control group showed
signi cant reduction in total scores obtained in Childhood Autism Rating Scale (P=0.05). In other words, play therapy
is effective in improved cognitive-behavioral symptoms of autistic disorder.
KEY WORDS: PLAY THERAPY, COGNITIVE-BEHAVIORAL SYMPTOMS, AUTISTIC DISORDER
249
ARTICLE INFORMATION:
*Corresponding Author:
Received 27
th
Dec, 2016
Accepted after revision 2
nd
March, 2017
BBRC Print ISSN: 0974-6455
Online ISSN: 2321-4007
Thomson Reuters ISI ESC and Crossref Indexed Journal
NAAS Journal Score 2017: 4.31 Cosmos IF : 4.006
© A Society of Science and Nature Publication, 2017. All rights
reserved.
Online Contents Available at: http//www.bbrc.in/
Biosci. Biotech. Res. Comm. Special Issue No 1:249-254 (2017)
INTRODUCTION
We live in an age when children’s disorders and diseases
are considered by families, specialists and health systems
more than any other time. A child who is born has the
highest and fullest growth potential. He is created at his
best and has the readiness and capacity to be trained in
the most appropriate way and achieve the highest per-
fections. Children’s nervous system like adults’ nervous
system has not reached full development since growth
continues and in other words, children are changing and
evolving; thus, their behavior is always changing. Given

250 INVESTIGATING THE EFFECTIVENESS OF PLAY THERAPY BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
Samira Hatami and Fatemeh Rahmani
that children depend heavily on parents and others and
are immature in terms of physical and mental capabili-
ties, the only thing they can do in the face of pressures
and discomforts is the incidence of behavioral disorders.
Indeed, the child’s behavior is his expressive language.
The more problems the child experiences in associa-
tion with others and expression of his own feelings and
needs, the greater his mental and behavioral disorders
will be (Glus, 1998; translated by Jamalfar, 1998).
Among exceptional children, autistic children have a
highly sensitive place. Fast and accurate detection and
diagnosis and subsequently treatment of such children
are of crucial importance. Man has failed to de nitively
treat this disorder; even in many cases, these patients
are not diagnosed. For this reason, it is often thought
that this disease is not highly prevalent. Parents of autis-
tic children are willing to know why their child is not
able to properly speak and communicate with peers and
people or play with age-appropriate toys. The question
is whether or not the incidence of these disorders is con-
genital. Accordingly, they seek treatment for their child’s
disease (Rafe’ei, 2006).
STATEMENT OF THE PROBLEM
Pervasive developmental disorder is a term that is cur-
rently used to refer to severe psychological problems
that appear in childhood. These disorders embrace seri-
ous disturbance in cognitive, social, behavioral and
emotional development of the child, which have broad
consequences and effects on the growth process. In
this group of diseases, social skills, language develop-
ment and behavioral repertoire either have not properly
developed or have been lost in early childhood (Kaplan,
Sadok & Gerb, 1987; translated by Fazel & Karimi, 1996).
Autistic children show impairment in social interac-
tion in several ways. Their nonverbal behaviors indicate
emotional distance which is characterized by avoidance
of making eye contact, strange facial effects and use
of special gestures to control interactions. Unlike most
children who like to play with other children, these chil-
dren avoid establishing relationships with peers. They
resist their parents’ hugging and fondling in childhood.
Autistic children are not able to talk or show too much
delay in language acquisition (Haldgin & Witborn, 1997;
translated by Seyyed Mohammadi, 2007).
Play therapy is also one of the effective methods in
the treatment of children’s behavioral and mental prob-
lems. Playing has a great impact on the child’s growth.
In fact, playing is a natural instrument for the child to
express “himself” and his feelings, establish communi-
cation, describe experiences, reveal the wishes and reach
self-actualization (Landreth, 1985; translated by Arian,
1995).
By reviewing the theoretical background and studies
conducted on the subject, it can be found that although
multiple investigations have been carried out about
variables of the subject and their relationship with one
another, few studies have been conducted on the effect
of play therapy on cognitive-behavioral symptoms of
disorders including autism pervasive developmental dis-
order. Further, in this eld, there is no research that has
directly addressed the effectiveness of play therapy in
improving cognitive-behavioral symptoms of autistic
disorder. Therefore, with regard to the above framework,
the researcher in the present study seeks to answer this
fundamental question as to “whether play therapy is
effective in improving cognitive-behavioral symptoms
of autism”.
RESEARCH HYPOTHESIS
Play therapy is effective in improving cognitive-behav-
ioral symptoms of autistic children.
RESEARCH VARIABLES
Independent variable: In this study, play therapy
is the independent variable.
Dependent variable: Cognitive-behavioral symp-
toms of autistic children are considered as the
dependent variable.
Control variable: In this study, age and gender are
regarded as the control variables. Intervening vari-
able: In this study, mental retardation, hyperactiv-
ity and other associated disorders are considered
as the intervening variables.
De nitions of terms Theoretical de nitions of vari-
ables Theoretical de nition of play therapy: Play ther-
apy is a form of psychotherapy that is used for young
children in response to their limited ability to express
oneself verbally (Levinger, 1994).
Theoretical de nition of cognitive-behavioral
symptoms of autistic disorder: These symptoms com-
prise the inability to mutually communicate with others
from early in life, having fun with objects rather than
humans, compulsive behavior in the face of changes,
impaired verbal communication and cliché and repeti-
tive behaviors (Aksline, 1997; translated by Mozayyani;
Nowzar Adan, 1989).
Theoretical de nition of autism: It is a severe dis-
ability that occurs in the rst 3 years of life and is
caused by the neurological disorder that affects brain
function (Rafe’ei, 2006). Operational de nitions of vari-
ables Operational de nition of play therapy Passive play
therapy techniques which include 13 activities are used
during 12 sessions of 45 minutes for the subjects of the
experimental group.Operational de nition of cognitive-

BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS INVESTIGATING THE EFFECTIVENESS OF PLAY THERAPY 251
Samira Hatami and Fatemeh Rahmani
behavioral symptoms of autistic disorder. It is the score
obtained by the individual in Childhood Autism Rating
Scale.
Operational de nition of autism: It starts at age 3 and
is characterized by having at least 6 cases of the features
mentioned in DSM-IV-TR. Checklist of Autism in Tod-
dlers (CHAT) can also be used.
Research type: This research is a quasi-experimental
study in which attempt has been made to control the
intervening variables to the extent possible.
Research design: This study is a pretest-posttest
quasi-experimental design with two experimental and
control groups.
RT
1
X
1
T
2
RT
3
T
4
Statistical population and sample: The research sta-
tistical population consists of all children with autism in
Mashhad in the year 2009-2010. The statistical sample
comprises 30 individuals (15 subjects in the experimen-
tal group and 15 subjects in the control group) from
among autistic boy children aged 5 to 13 years in Tabas-
som educational center for autistic children.
COMMUNICATION WITH PEOPLE
1. No evidence of forms of abnormality in commu-
nication with people: The child’s behavior is ap-
propriate to his age. When he is asked to do some-
thing, he may seem a little bit shy, fastidious or
upset; but it not abnormal. -1.5
2. Mildly abnormal communications: The child may
avoid eye contact with adults. He may keep aloof
from adults or become disturbed if he is forced to
interact. He may be greatly shy. He does not re-
spond normally to adults and is more attached to
his parents than the children of his age. -2.5
3. Moderately abnormal communications: The child
sometimes stays away from adults or it seems that
he is unaware of what adults do. Sometimes con-
tinuous and emphatic effort is essential to attract
the child’s attention. -3.5
4. Severely abnormal communications: The child
constantly avoids adults or is unaware of what
adults do. In contact with adults, he is almost nev-
er the initiator. Continuous effort is needed to at-
tract the child’s attention.
IMITATION
1. Appropriate imitation: The child can imitate the
sounds, words and movements according to his age and
skill level. -1.5 2. Mildly abnormal imitation: The child
imitates simple behaviors like clapping or monophonic
sounds. Sometimes he imitates after stimulation or with
little delay. -2.5 3. Moderately abnormal imitation: The
child only sometimes imitates and for this purpose, help
and insistence of adults are needed. He mostly imitates
with little delay. -3.5 4. Severely abnormal imitation: The
child rarely or never imitates the sounds, words or move-
ments unless with the stimulation and help of adults.
EMOTIONAL RESPONSE
1. Emotional responses appropriate to age and situation:
Type and degree of the child’s emotional responses are
appropriate and are determined by changes in his facial
expression, gesture and behavior. -1.5 2. Mildly abnormal
emotional responses: Type and degree of the child’s emo-
tional responses are sometimes appropriate. Reactions are
not usually associated with the objects or events around
him. -2.5 3. Moderately abnormal emotional responses:
Type and degree of the child’s emotional responses are
quite inappropriate. Reactions may be totally limited or
very severe and without any association with the situa-
tions. The child may mimic, laugh or become in exible
while there is no object or event explicitly causing this
issue. -3.5 4. Severely abnormal emotional responses:
Responses are rarely appropriate to the situation. When
the child has a stable temperament, it is very dif cult to
change it. Conversely, the child may show completely dif-
ferent feelings while nothing has changed.
BODY MOVEMENTS
1. Body movements appropriate to the age: The child can
move as easily and quickly as the children of his own
age. -1.5 2. Mildly abnormal body movements: Some
strange states such as clumsiness, repetitive movements,
poor coordination or rarely unusual movements may
exist. -2.5 3. Moderately abnormal body movements:
The child’s behaviors are quite strange and unusual
with regard to his age and include strange nger move-
ments, strange nger position or body gesture, staring
at the body, spontaneous aggression, wiggling, squirm-
ing, repetitive movements of the ngers and walking
on toes. -3.5 4. Severely abnormal body movements:
Severe or persistent movements of the above suggest
very abnormal body movements. These behaviors may
persist despite the efforts to prevent them or involving
children in other activities.
CHANGE ADAPTATION
1. Age-appropriate response to change: If the child nor-
mally notices changes or he is reminded, he accepts with
no insistence. -1.5 2. Mildly abnormal change adapta-
tion: If adults try to change the child’s tasks, he may
do the same activity or apply the same thing. -2.5 3.
Samira Hatami and Fatemeh Rahmani
252 INVESTIGATING THE EFFECTIVENESS OF PLAY THERAPY BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
Moderately abnormal change adaptation: The child usu-
ally resists changes and tries to do the old jobs so that
it is dif cult to dissuade him. If his xed and daily rou-
tines change, he may become upset and angry. -3.5 4.
Severely abnormal change adaptation: The child shows
severe reactions to change. If he is forced to adapt him-
self to the change, he becomes furious and does not
cooperate and his response is accompanied by turmoil.
IMPLEMENTATION METHOD
To do this research, after coordination carried out by the
University with Mashhad Bureau of Exceptional Educa-
tion, we were introduced to Tabassom educational center
for autistic children. It should be noted that comprehen-
sive diagnostic evaluation of autistic children was done
in two stages:
First stage: Preliminary diagnosis or initial assess-
ment
In this stage, child development screening test is per-
formed. Parents’ observations and information about
child development and its history can greatly help in
this step. Some of the screening tools which collect data
about the child’s social development and communica-
tion skills are as follows:
1. Checklist of Autism in Toddlers (CHAT)
2. Screening Tool for Autism in Two-Year-Olds
(STAT)
3. Social Communication Questionnaire (SCQ) for
children of 4 years and older
4. PDD assessment Scale/Screening Questionnaire
(ASSQ)
If suspicious signs of a problem or disorder are observed
in the diagnosis phase or initial assessment, the child is
referred for comprehensive diagnostic evaluation.
Second stage: Comprehensive diagnostic evalua-
tion: This evaluation is performed by a group of spe-
cialists including child psychiatrist, neurotourist, occu-
pational therapist and speech therapist. In this stage,
Autism Diagnostic Interview (ADI-R) which is a struc-
tured interview is completed with the help of the child’s
parents or caregiver. Additionally, CARS tool can be
applicable.In this study, 30 children were selected as
the sample through available sampling method. After
randomly assigning the subjects into the experimental
(n=15) and control (n=15) groups, the two groups took
a pretest using Childhood Autism Rating Scale (CARS).
Play therapy was passively implemented for the subjects
of the experimental group during 12 sessions of 45 min-
utes (3 sessions per week). At the end of play therapy, a
posttest was taken from both groups.
INFERENCE OF DATA
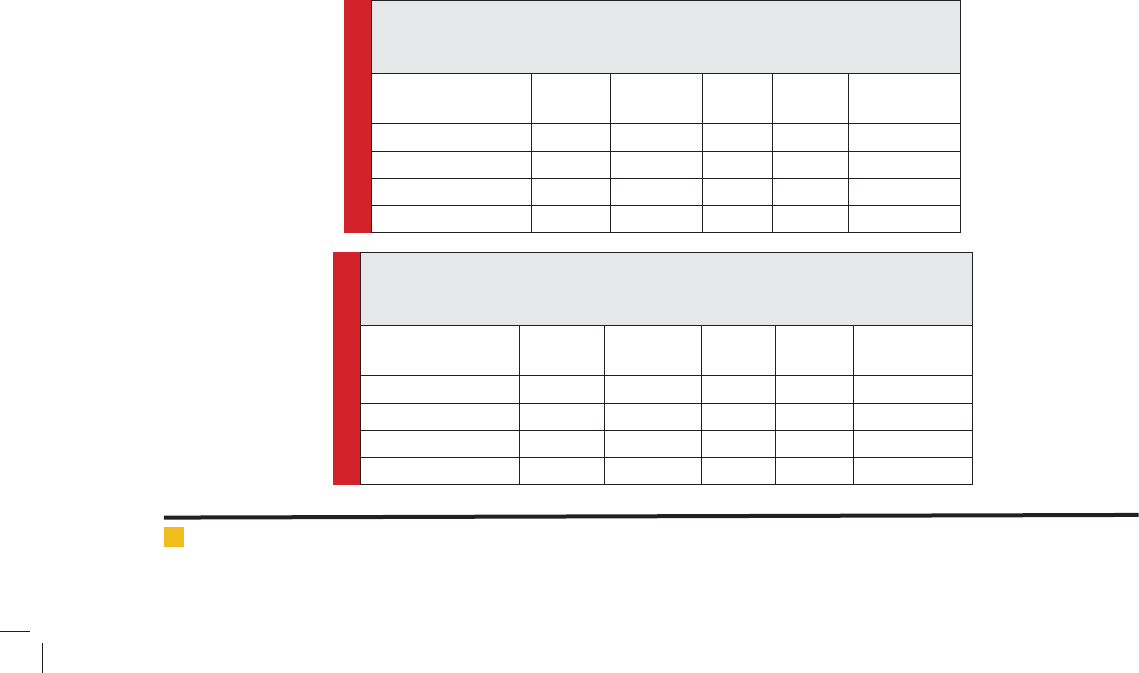
It can be observed in the above table that F coef cient to
compare the mean posttest score of the rst cognitive-
behavioral symptom of autism (communication with
people) in the experimental and control groups (after
controlling the pretest scores) was calculated to be 0.96
which is not statistically signi cant (P
0.05) and thus,
the null hypothesis is accepted and it is concluded that
the implementation of play therapy has no signi cant
in uence on improving the rst component of Child-
hood Autism Rating Scale (communication with people).
Table 1: Results obtained from covariance analysis of the experimental
group with the control group in the rst component of Childhood Autism
Rating Scale (communication with people)
Analysis of
covariance factors
Sum of
squares
Degree of
freedom
Mean
Square
F value Signi cance
level
Pretest 7.14 1 7.14 162.47 0.000
Intergroup 0.04 1 0.04 0.96 0.34
Error 1.18 27 0.043
Total 8.46 29
Table 2. Results obtained from covariance analysis of the experimental group
with the control group in the second component of Childhood Autism Rating
Scale (imitation)
Analysis of
covariance factors
Sum of
squares
Degree of
freedom
Mean
Square
F value Signi cance
level
Pretest 8.10 1 8.10 193.39 0.000
Intergroup 0.08 1 0.08 1.92 0.17
Error 1.31 27 0.04
Total 9.36 29
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS INVESTIGATING THE EFFECTIVENESS OF PLAY THERAPY 253
Samira Hatami and Fatemeh Rahmani
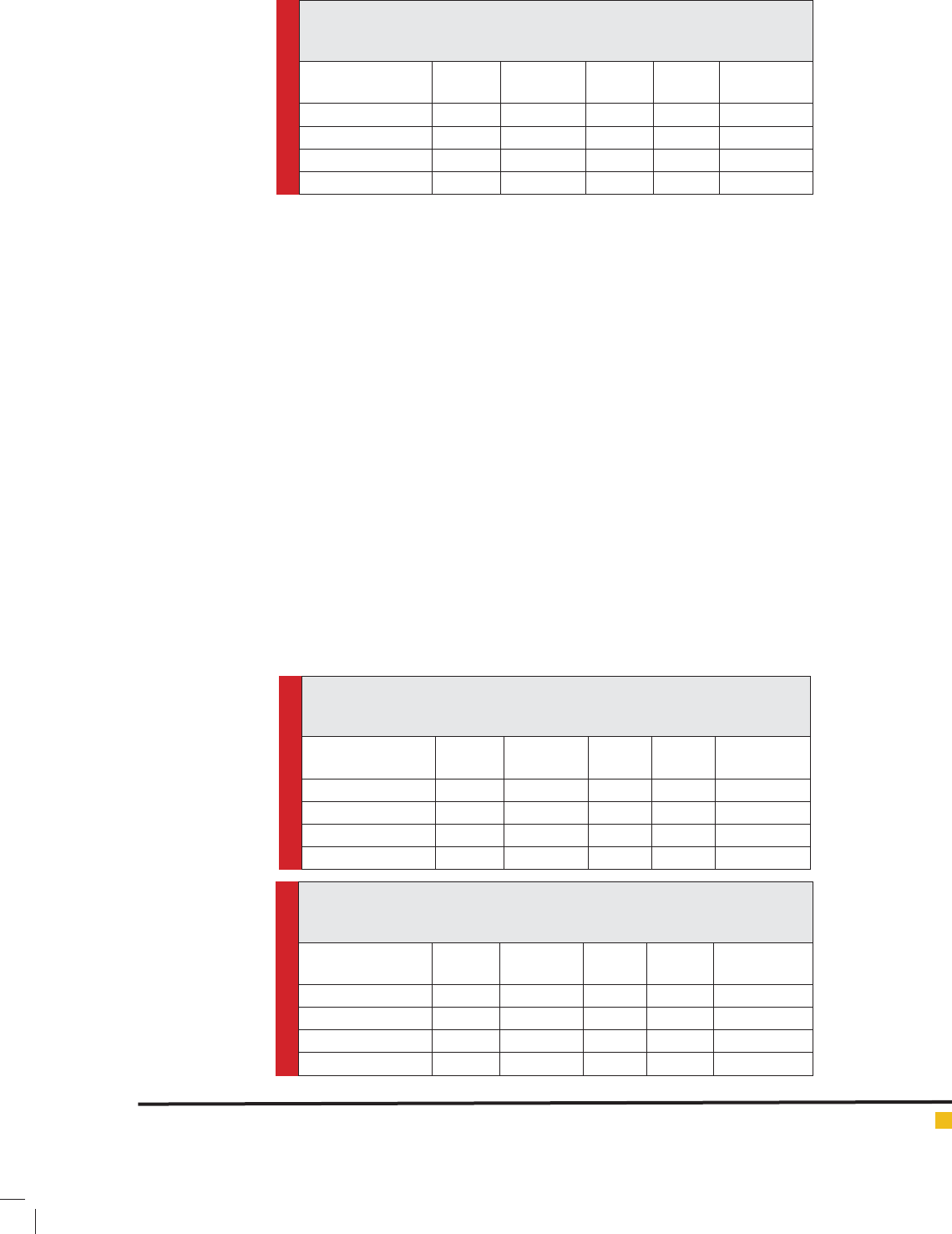
Table 3. Results obtained from covariance analysis of the experimental group
with the control group in the third component of Childhood Autism Rating
Scale (emotional response)
Analysis of
covariance factors
Sum of
squares
Degree of
freedom
Mean
Square
F value Signi cance
level
Pretest 2.98 1 2.98 31.66 0.000
Intergroup 0.003 1 0.003 0.003 0.95
Error 2.54 27 0.094
Total 5.74 29
Table 4. Results obtained from covariance analysis of the experimental group
with the control group in the fourth component of Childhood Autism Rating
Scale (body movements)
Analysis of
covariance factors
Sum of
squares
Degree of
freedom
Mean
Square
F value Signi cance
level
Pretest 5.74 1 5.74 104.24 0.000
Intergroup 1.89 1 1.89 0.000 0.98
Error 1.48 27 0.05
Total 7.24 29
Table 5. Results obtained from covariance analysis of the experimental group
with the control group in the fth component of Childhood Autism Rating
Scale (change adaptation)
Analysis of
covariance factors
Sum of
squares
Degree of
freedom
Mean
Square
F value Signi cance
level
Pretest 6.19 1 6.19 70.56 0.000
Intergroup 0.31 1 0.31 3.60 0.06
Error 2.37 27 0.08
Total 8.57 29
It can be seen in the above table that F coef cient
to compare the mean posttest score of the second cog-
nitive-behavioral symptom of autism (imitation) in the
experimental and control groups (after controlling the
pretest scores) was calculated to be 1.92 which is not
statistically signi cant (P
0.05) and hence, the null
hypothesis is accepted and it is concluded that the imple-
mentation of play therapy has no signi cant impact on
improving the second component of Childhood Autism
Rating Scale (imitation).
It can be seen in the above table that F coef cient to
compare the mean posttest score of the third cognitive-
behavioral symptom of autism (emotional response) in
the experimental and control groups (after controlling
the pretest scores) was estimated to be 0.003 which is
not statistically signi cant (P
0.05) and therefore,
the null hypothesis is accepted and it is concluded that
the implementation of play therapy has no signi cant
impact on improving the third component of Childhood
Autism Rating Scale (emotional response).
It can be observed in the above table that F coef-
cient to compare the mean posttest score of the fourth
cognitive-behavioral symptom of autism (body move-
ments) in the experimental and control groups (after
controlling the pretest scores) was calculated to be 0.000
which is not statistically signi cant (P
0.05) and so,
the null hypothesis is accepted and it is concluded that
the implementation of play therapy has no signi cant
effect on improving the fourth component of Childhood
Autism Rating Scale (body movements).
It can be seen in the above table that F coef cient to
compare the mean posttest score of the fth cognitive-
behavioral symptom of autism (change adaptation) in
the experimental and control groups (after controlling
the pretest scores) was calculated to be 3.60 which is
not statistically signi cant (P
0.05) and thus, the
null hypothesis is accepted and it is concluded that the
implementation of play therapy has no signi cant effect
on improving the fth component of Childhood Autism
Rating Scale (change adaptation).

254 INVESTIGATING THE EFFECTIVENESS OF PLAY THERAPY BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
Samira Hatami and Fatemeh Rahmani
In the present study, it has been hypothesized that
play therapy is effective in improving cognitive-behav-
ioral symptoms of autistic disorder. With regard to data
analysis in section 4, the research ndings revealed that
after implementing the techniques of play therapy, sig-
ni cant changes have been made in the whole cognitive-
behavioral symptoms of autistic children. Evaluation of
the experimental group scores after the implementation
of play therapy suggested that there is signi cant differ-
ence between autistic children and subjects of the control
group in cognitive-behavioral symptoms and this indi-
cates that this treatment method has had a positive effect
on improving cognitive-behavioral symptoms of autism.
The results obtained from this research are consistent
with the ndings achieved in some other studies in this
regard. Thorp et al., (1995) and also McDonough et al.
(1997) in a study investigated the effects of play therapy
and puppet show on the treatment of autistic children.
The obtained results demonstrated that this method is
effective in the treatment of such children. Forest (2004)
conducted a study and showed that play therapy is an
effective method regarding the children who have expe-
rienced events or problems in life. Sarlak and Rasouli-
yan (1388) have also referred to the effectiveness of
voice therapy in increasing the rate of hearing and thus
auditory responses of autistic children.
Qaderi, Asghari Moqaddam and Sha’eiri (2006) and
Zolmajd, Borjali and Arian (2007) also examined the
impact of play therapy on children’s aggression. The
ndings indicated a reduction in the level of aggression
in these children. Salehi (2009) has studied the effect of
play therapy on reduced oppositional de ant disorder.
The research results revealed that play therapy signi -
cantly reduces the severity of symptoms of oppositional
de ant disorder.
RESEARCH SUGGESTIONS
Application of the ndings of this study in Welfare
Organization, Exceptional Education and other cent-
ers that engage in counseling for children with disorder
and use of play therapy as an effective method in the
treatment of children’s disorders. Establishment of cent-
ers and institutions having specialized and experienced
personnel and all kinds of facilities for the treatment of
these children with an emphasis on play therapy method.
Reassessment of subjects after 3 or 6 months to examine
the effectiveness and stability of results and also evalua-
tion of the sustainability of this treatment method.
REFERENCES
Ahmadayi (Talarizadeh), A. (2003). Cultivation of mental abili-
ties and elimination of learning disorders. Tehran: Mabna.
Bardideh, M. R. (1998). Autism and pseudo autism disorders.
Shiraz: Sasan.
Bahrami, H. (1982). Child Psychology. Tehran: Iran Revolu-
tionary Guards University.
Torkman, M. & Moqaddam, M. (1997). Educational games.
Tehran: Madreseh.
Khodaei Khiyavi, S. (2001). Psychology of play. Tabriz: Ahrar.
Delavar, A. (2001). Research Method in Psychology and Educa-
tional Sciences. Tehran: Virayesh.
Rafe’ei, T. (2006). Autism, evaluation and treatment. Tehran:
Danzheh.
Rezazadeh, M. (2004). The impact of Educational games on
reduced severity of symptoms of attention de cit hyperactivity
disorder. Master’s thesis. Tehran: Faculty of Educational Sci-
ences and Psychology.
Sarlak, N. & Rasouliyan, M. (2009). Voice therapy in the treat-
ment of autistic children. Exceptional Education (92): 52-54.
Seif, A. A. (1998). Change in behavior and behavior therapy:
Theories and methods. Tehran: Dowran.
Sho’arinezhad, A. A. (1998). Psychology of development. Teh-
ran: Payam Noor University.
Qaderi, N., Asghari Moqaddam, M. A. & Sha’eiri, M. R. (2006).
Investigating the ef ciency of cognitive-behavioral play
therapy in the aggression of children with conduct disorder.
Daneshvar rafter, 4 (7): 75, 84.
Qazvininezhad, H. (2006). Generalities of play therapy. Tehran:
Ayizh.
Kendall, F. S. (2003). Childhood disorders. Translated by M.
Kalantari & M. Gohari Anaraki. Esfahan: Jahad Daneshgahi.
(Date of publication in the original language, 1998).
Lot Kashani, F. & Vaziri, Sh. (1997). Child psychopathology.
Tehran: Arasbaran.
Mohammadi, M. R., Mesgarpour, B., Sahimi Izadian, A. &
Mohammadi, M. (2007). Psychological and psycho-pharma-
ceutical tests of children and adolescents. Tehran: Teimour-
zadeh.
Mahjour, S. R. (1991). Psychology of play. Shiraz: Rahgosha.
Milanifar, B. (1999). Psychology of Exceptional Children and
Adolescents. Tehran: Qomes.
Halgin, R. P. & Whitbourne, S. K. (2007). Clinical Perspec-
tives on Mental Disorders (Volume II). Translated by Y. Seyyed
Mohammadi. Tehran: Ravan. (Publication date in the original
language, 1997)