
Structure of solid waste management in hospitals of
Bandar Abbas city
Naser Rahmanian
1
, Abbas Ghavam
2
* and Abbas Yazdanpanah
3
1
Department of Healthcare Management, Marvdasht Branch, Islamic Azad University, Marvdasht Iran
2
Assistant Professor, Department of Environmental Science, Institute of Sciences and High Technology and
Environmental Sciences, Graduate University of Advanced Technology, Kerman, Iran
3
Assistant professor, Department of Healthcare Management, Marvdasht Branch, Islamic Azad University,
Marvdasht, Iran
ABSTRACT
One of the major sources of waste in each city is the hospital centers, which produce a wide range of waste. These
wastes should not be mixed with municipal wastes, because the spread of chemical and biological materials con-
taining the dangerous pathogens causes the speci c environmental and health hazards. Lack of control and lack of
attention to proper management of hospital wastes on how to collect, store, transport and dispose of such waste,
will lead to the prevalence of regional and urban epidemics and diseases and waste of money that this is a serious
threat to the public health and environment. The aim of this study is to evaluate trends in waste management in
hospitals of Bandar Abbas and adapt this process with the national standards. This is an applied study conducted
in a descriptive-analytic method. In this study, one sample t method was used. The sample consisted of 107 waste
production sites in 8 hospitals in Bandar Abbas that the census method was used. To evaluate the variables, it was
used the Health Ministry’s standard checklist for hospital waste review. The data was analyzed by SPSS software
and using the descriptive and inferential statistics. There is no signi cant difference between the average total per
capita solid waste per bed in hospitals in Bandar Abbas and the average total per capita solid waste per bed set by
the Ministry of Health (t = 1.922). It means the average per capita waste generation in hospitals in Bandar Abbas is
consistent with the regulations of the Ministry of Health. There is a match between the average per capita ordinary
solid waste generation with the average ordinary solid waste generation set by the Ministry of Health (t = 1.631). It
means the average ordinary waste in hospitals of Bandar Abbas is consistent with the regulations of the Ministry
of Health. The average duration of waste storage in hospitals of Bandar Abbas is consistent with the average waste
storage in accordance with regulations of the Ministry of Health related to similar areas (hot and humid conditions
(t = 22.12). This means that the average duration of waste storage in hospitals of Bandar Abbas corresponds to the
164
ARTICLE INFORMATION:
*Corresponding Author: ghavam39@gmail.com
Received 30
th
Dec, 2016
Accepted after revision 12
th
March, 2017
BBRC Print ISSN: 0974-6455
Online ISSN: 2321-4007
Thomson Reuters ISI ESC and Crossref Indexed Journal
NAAS Journal Score 2017: 4.31 Cosmos IF : 4.006
© A Society of Science and Nature Publication, 2017. All rights
reserved.
Online Contents Available at: http//www.bbrc.in/
Biosci. Biotech. Res. Comm. Special Issue No 1:164-171 (2017)

Rahmanian, Ghavam and Yazdanpanah
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS STRUCTURE OF SOLID WASTE MANAGEMENT IN HOSPITALS OF BANDAR ABBAS CITY 165
time determined by the Ministry of Health for the hot and humid weather conditions. Using the above results, it can
be concluded that the establishment of environmental health experts at hospitals, daily tracking and proper training
for personnel involved in the production, and collection and disposal of hospital wastes could play an effective role
in preventing the risks of hospital wastes.
Correct management training and disposal of hospital wastes should be one of the operational objectives of hos-
pital managers and this important issue should be included in planning courses for staff of all hospitals.
KEY WORDS: SOLID WASTE – MANAGEMENT – HOSPITAL –BANDAR ABBAS
INTRODUCTION
Today, increasing waste and environmental pollution
and health hazards resulting from it has been raised as
one of the most important problems in human societies
today, (Chartier, 2014). The whole extent of this waste
is so high in which we can nd the ordinary household
waste to the dangerous chemical and biological contam-
inants. One of the major sources of waste generation in
each city is the hospitals which produce a wide range of
waste (Zarei, Taghdisi, Keshavarz Mohamadi, & Tehrani,
2013).
The great thing about the medical wastes is that these
wastes should not be mixed with municipal wastes,
because the spread of chemical and biological materials
containing the dangerous pathogens causes the speci c
environmental and health hazards. Classi cation and
composition of medical waste with particular attention
to the collection and disposal of it include a wide range
of different materials, such as ordinary or household-
like, infectious, chemical, and pharmaceutical wastes
(Chartier, 2014), (Zarei et al., 2013). The household-like
wastes includes materials such as paper, cardboard, car-
ton, plastic materials, remnants of food and fruit that if
not mixed with the hazardous and infectious materials
are safe and they can be collected and disposed of as
the household waste (Kumar, Samrongthong, & Shaikh,
2013). The potentially infectious wastes exist in various
forms as the contaminated disposable supplies and sharp
instruments products containing blood, and laboratory
culture media, (Nie, Qiao, & Wu, 2014 and Ndejjo et al.,
2015).
Based on WHO, the infectious wastes include the
wastes that contain the pathogens to the extent that
can cause the disease in the susceptible hosts, (WHO,
2004). There are different opinions in the classi cation
and de nition of infectious wastes. The sharp wastes
include the needles, syringes, broken glasses and scal-
pels. Since these components can create the injury and
lead the pathogens such as hepatitis and AIDS to enter
the human body, therefore it is necessary to separate
them from other infectious wastes (Rastegar & Gholami,
2014). The chemical and pharmaceutical wastes includes
the drugs, pharmaceutical products and various chemi-
cals that are produced by the speci c health activities
in these centers. The drugs and chemicals returned or
discarded and expired are also part of this category.
Therefore, the particular attention to the separate col-
lection and disposal of them is very important. This is
while sometimes seen in Bandar Abbas that for reasons of
high cost of solid waste disposal, the illegal and hygienic
ways are used to dispose of the wastes. Since the lack
of control and lack of attention to proper management
of hospital wastes on how to collect, preserve, transport
and dispose of such waste will lead to the prevalence of
regional and urban epidemics and diseases and waste of
money, this is considered as a serious threat to the public
health and environment.
This study aimed to assess the waste management
process in hospitals of Bandar Abbas and adapt this pro-
cess with the national standards. So, at rst, the aim of
this study is to evaluate the waste management process
in hospitals of Bandar Abbas and adapt this process with
the national standards and secondly, to nd the stand-
ard deviation and provide the administrative approaches
to standardize the structure.
MATERIAL AND METHODS
In this descriptive-analytic study, the research environ-
ment was the hospitals of Bandar Abbas, including the
university hospitals (Shahid Mohammadi- chilrens’),
private hospitals (Om-e-Leila and Imam Reza), hospitals
af liated with the police and armed forces (Saheb-al-
Zaman, Seyed-al-Shohada and Khatam-ol-anbia) and
Persian Gulf hospital af liated to social security. The
study population consisted of 107 waste production sites
in the 8 hospitals of Bandar Abbas. (N=107)
The standard waste management checklist of Ministry
of Health related to the collection of waste management
data in country’s hospitals was used by the researcher
to collect the data. The standard checklist Ministry of
Health has been 105 years that after soliciting the opin-
ion of experts of environmental health department of
the Health Center in Hormozgan province and profes-
sors of environmental health department at the School
of Health in Bandar Abbas, it was summarized to the 42
Rahmanian, Ghavam and Yazdanpanah
166 STRUCTURE OF SOLID WASTE MANAGEMENT IN HOSPITALS OF BANDAR ABBAS CITY BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
questions to collect better data. So, the checklist used
to collect the research data had 42 questions that was
applied for the different stages of hospital waste man-
agement, including how to produce waste, status of col-
lection, transportation, weighing, disinfecting and nal
disposal of hospitals’ solid wastes in Bandar Abbas.
The checklist includes six scales that are the per cap-
ita waste, disinfecting procedures, management com-
ponents in waste disposal, waste separation, storage,
transportation and methods of nal disposal of waste.
Questions of subscales are as follows: Per capita waste,
questions 7, 8, 9, 10, 11, 12, 13, 14, 15 and 16; that how
to measure on these questions is as kg per day. Disin-
fecting methods, questions 17, 18, 19 and 20; which the
method of measurement is based on standard or non-
standard methods.
Management components in waste disposal, ques-
tions 21, 22, 23, 24 and 25; that the method of measur-
ing them is as yes / no, complete / incomplete. Waste
separation, questions 25, 26, 27 and 28, that the method
of measuring them is as yes / no, complete / incomplete.
Storage and transportation, questions 29, 30, 31, 32, 33,
34, 35, 36, 37, 38, 39, 40, 41, 42, 43 and 44, that the
measurement method is as yes / no, complete / incom-
plete. Methods for nal disposal of wastes, questions 45,
46, 47 and 48, that the measurement method is as yes /
no, complete / incomplete. In this questionnaire, obtain-
ing less points means more consistent with the standards
of the Ministry of Health.
In this review, after completing the paperwork and
obtaining the necessary permits, in collaboration with
the Deputy Treatment and Deputy Health of medical
university and hospital managers in Bandar Abbas, the
research data in hospitals of Bandar Abbas was collected
in 4 steps as follows.
FIRST STAGE
The research environments were visited in a eld method
(waste production sites, including wards, outpatient
departments, clinics, diagnostic departments, operating
rooms, drug stores, administration and support depart-
ments, kitchens and cafeterias) and the solid waste col-
lection sites, people involved in the production process,
collection, transportation, storage and nal disposal of
wastes were identi ed.
SECOND STAGE
At this stage, it was justi ed the people involved in the
production process to the nal disposal of wastes in hos-
pitals on the goal of the study, for this purpose, in coor-
dination with the hospital manager and health experts
based in hospitals, the people gathered in the audito-
rium of the hospital and the functional objectives and
implementation phases of the study were described for
them. As the number of people involved in the Shahid
Mohammadi hospital was great, 3 brie ngs were held in
this hospital and 2 brie ngs were held in the children’s’
hospital and Persian Gulf hospital. In other hospitals, a
meeting was held to justify the people involved.
THIRD STAGE
At this stage, the designated sites were daily visited
and then the process of collecting, transporting, stor-
ing, weighing and disposing of the wastes generated
was observed and recorded for each site and nally, the
completed information related to the various stages of
producing solid waste in each hospital was recorded in
the standard checklist of Ministry of Health (checklist
of visiting the management of the collection, storage,
transportation and disposal of wastes in the country’s
hospitals). It should be noted that the standard check-
list Ministry of Health related to the different stages
of solid waste disposal in country hospitals has been
105 years that after soliciting the opinion of experts of
environmental health department of the Health Center
in Hormozgan province and professors of environmen-
tal health department at the School of Health in Bandar
Abbas, it was summarized to the 42 questions by the
researcher to collect better data.
FOURTH STAGE
At this stage, after collecting the data required in all
hospitals, the data collected was entered into SPSS 16
software and then using the descriptive and analytic
statistics and statistical tests, the per capita produc-
tion, duration of waste storage and waste management
method in the hospitals of Bandar Abbas were compared
with the regulations of the Ministry of Health.
In this study, the SPSS 16 software and descriptive
statistics including frequency, mean and standard devi-
ation; and inferential statistics including one sample
t-test (at the signi cance level 0.05) were used to ana-
lyze the data.
RESULTS
According to the results of this study, the amount and
percentage of the waste generated is shown in Table 1.
Accordingly, the amount of waste produced daily in hos-
pitals was 1987.45 kg that the waste generation in the
university hospitals was 921.45 kg, in the private hospi-
tals 383 kg, in the military and police hospitals 296 kg,
and in the social security hospital 387 kg per day.
As seen in Table 1, the highest average total pro-
duction of waste is in Social Security hospitals in the
Rahmanian, Ghavam and Yazdanpanah
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS STRUCTURE OF SOLID WASTE MANAGEMENT IN HOSPITALS OF BANDAR ABBAS CITY 167
Table 1. The quantitative components of the waste by the type of surveyed hospitals
Parameter Production
(Kg / d)
Average
(Kg / d)
Standard
deviation
(Kg / d)
Minimum
(Kg / d)
Maximum
(Kg / d)
% of ordinary
waste production
to the total
ordinary waste
produced
% Of total
Production
The total amount of waste
produced in university
hospitals
921.45 26.32 30.17 5 160 3.387 4.366
The total amount of
waste produced in private
hospitals
383 14.18 11.23 3 45 2.933 1.279
The total amount of waste
produced in military and
police hospitals
296 8.96 10.87 4 30 1.199 1.894
The total amount of waste
produced at the Social
Security Hospital
387 32.25 24.51 7 140 19.5 1.479
Table 2. Per capita waste generation in different hospitals studied
Hospitals Number of active beds Ordinary waste per capita
per active bed(Kg/d)
total waste per capita
per bed(Kg/d)
University hospitals 325 1.34 2.83
Private hospitals 169 1.6 2.26
Military and police hospitals 163 1.33 1.81
Social Security hospital 107 1.85 3.61
All hospitals 758 1.52 2.62
amount of 32.25 kg per waste production site and then
in the university hospitals with an average 26.33 kg of
waste per site. The lowest total waste production is in
the military and police hospitals with an average 8.96
kg per waste generation site. It is observed 37.38% of
ordinary wastes are created in the university hospitals
that this seems natural considering that most active beds
are related to the university hospitals and on the other
hand, these hospitals are teaching and more staff and
university students are working in them. The lowest per-
centage of ordinary waste production (Alam, Sujauddin,
Iqbal, & Huda, 2008) is also related to the military and
police hospitals in Bandar Abbas.
According to the study results, the number of active
beds and per capita total waste generation in the univer-
sity hospitals with 325 beds is 2.83 Kg / d, in the private
hospitals with 169 active beds is 2.26 Kg / d, in the
military and police hospitals with 163 beds is 1.81 Kg /
d and in the social security hospital with 107 active beds
is 3.61 Kg / d per active bed.
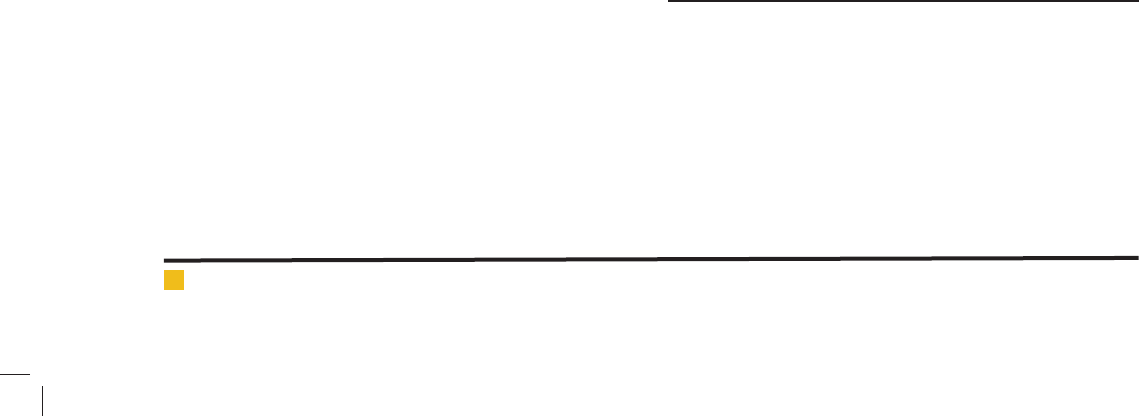
Another important indicator of waste management is
the waste storage time in the temporary storage site of
waste. The information in this section is presented in
Figure 1.
According to the gure, in 62.6% of the hospitals sur-
veyed, the waste storage time in temporary sites was
24 hours and in 25 percent of hospitals, the time was
between 24 to 48 hours and in 12.5% , the time was
between 48 and 72 hours.
According to the results of this study, most waste stor-
age time in temporary sites is respectively in the police
and military hospitals with an average of 56 hours, in
Social Security hospitals with an average of 28 hours, in
private hospitals with an average of 23 hours and less
time keeping waste is in the university hospitals with an
average of 21 hours.
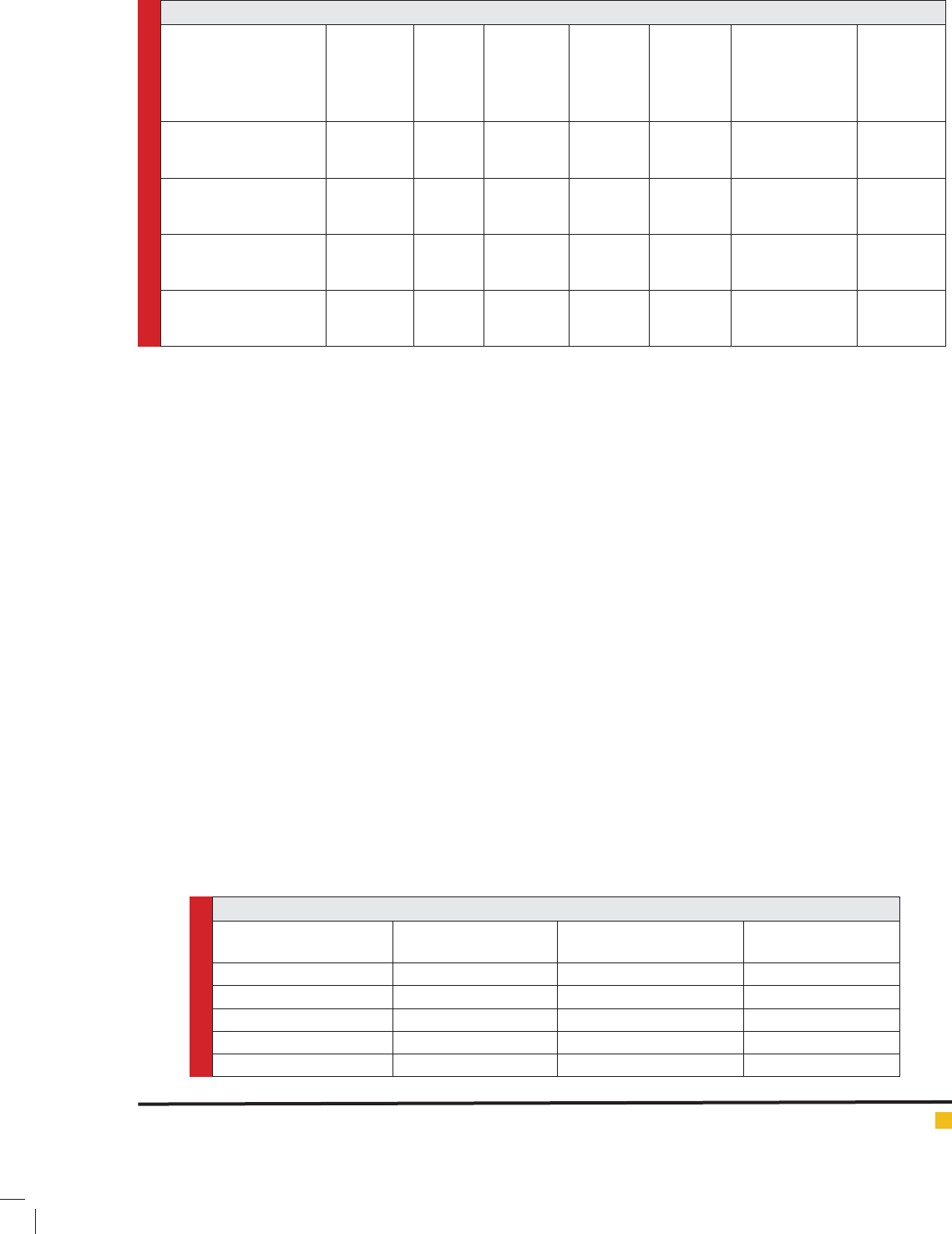
1. Lack of disinfection of waste containers
2. Disinfection of waste containers
3. Non-coding and labeling waste separated
4. Coding and labeling the waste
5. The absence of valid contracts with authorized
centers for transport and disposal of chemical and
pharmaceutical waste
6. Valid contracts with authorized centers for transport
and disposal of chemical and pharmaceutical waste
As seen in Figure 2, disinfection and labeling of waste
are done in 100 percent of hospitals, but only in 50 per-
Rahmanian, Ghavam and Yazdanpanah
168 STRUCTURE OF SOLID WASTE MANAGEMENT IN HOSPITALS OF BANDAR ABBAS CITY BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
cent of hospitals, it has been signed with authorized
centers to transport and dispose of chemical and phar-
maceutical waste.
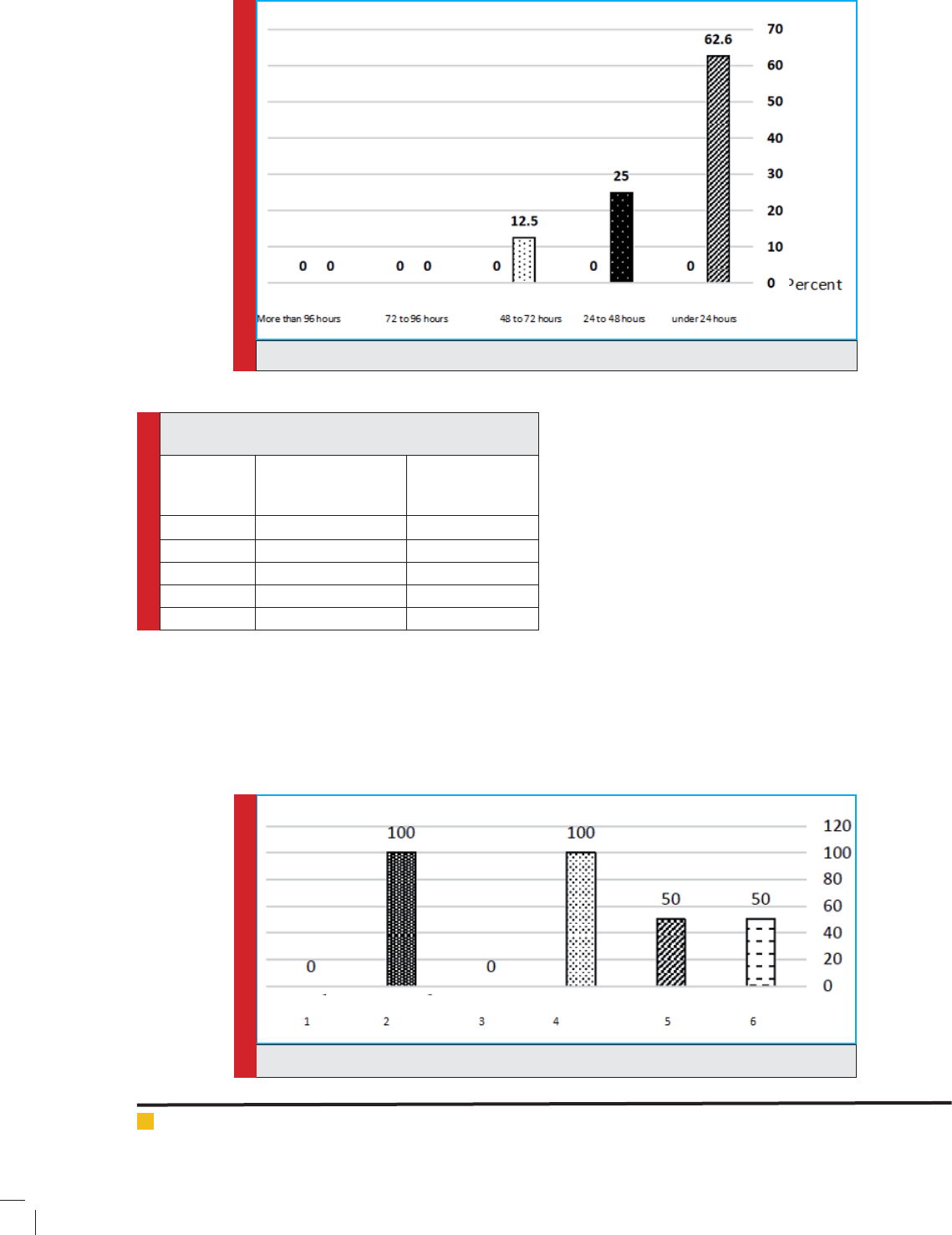
1. The absence of Safety Box to collect the sharp
waste
2. The existence of Safety Box to collect the sharp
waste
3. The lack of organs and limbs cut and dead fetus
4. Failure to collect the organs and limbs cut and
dead fetuses in accordance with regulations
5. Collecting the organs and limbs cut and dead fe-
tuses in accordance with the regulations
6. Collection along with other wastes
7. Separately storage method of chemical and phar-
maceutical wastes
As seen in Figure 3, the chemical, pharmaceutical and
biological wastes are separately kept in 75% of hospitals
studied. Also, in all the hospitals that have the patho-
logical wastes (organs and limbs cut and dead fetus, etc),
these wastes are collected according to regulations of
the Ministry of Health. This graph also shows that in the
majority of hospitals studied (87.5%), there is the safety
box for collecting the sharp wastes.
FIGURE 1. The waste storage time in temporary storage site of waste
Table 3. The average duration of waste storage by the
type of surveyed hospitals
Row Hospitals by the
type of ownership
The average
duration of waste
storage per hour
1 University Hospitals 21
2 Private Hospitals 23
3 Police Military Hospitals 56
4 Social Security Hospital 28
Total average 32
FIGURE 2. Maintenance management structureand transportation of waste containers
Rahmanian, Ghavam and Yazdanpanah
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS STRUCTURE OF SOLID WASTE MANAGEMENT IN HOSPITALS OF BANDAR ABBAS CITY 169
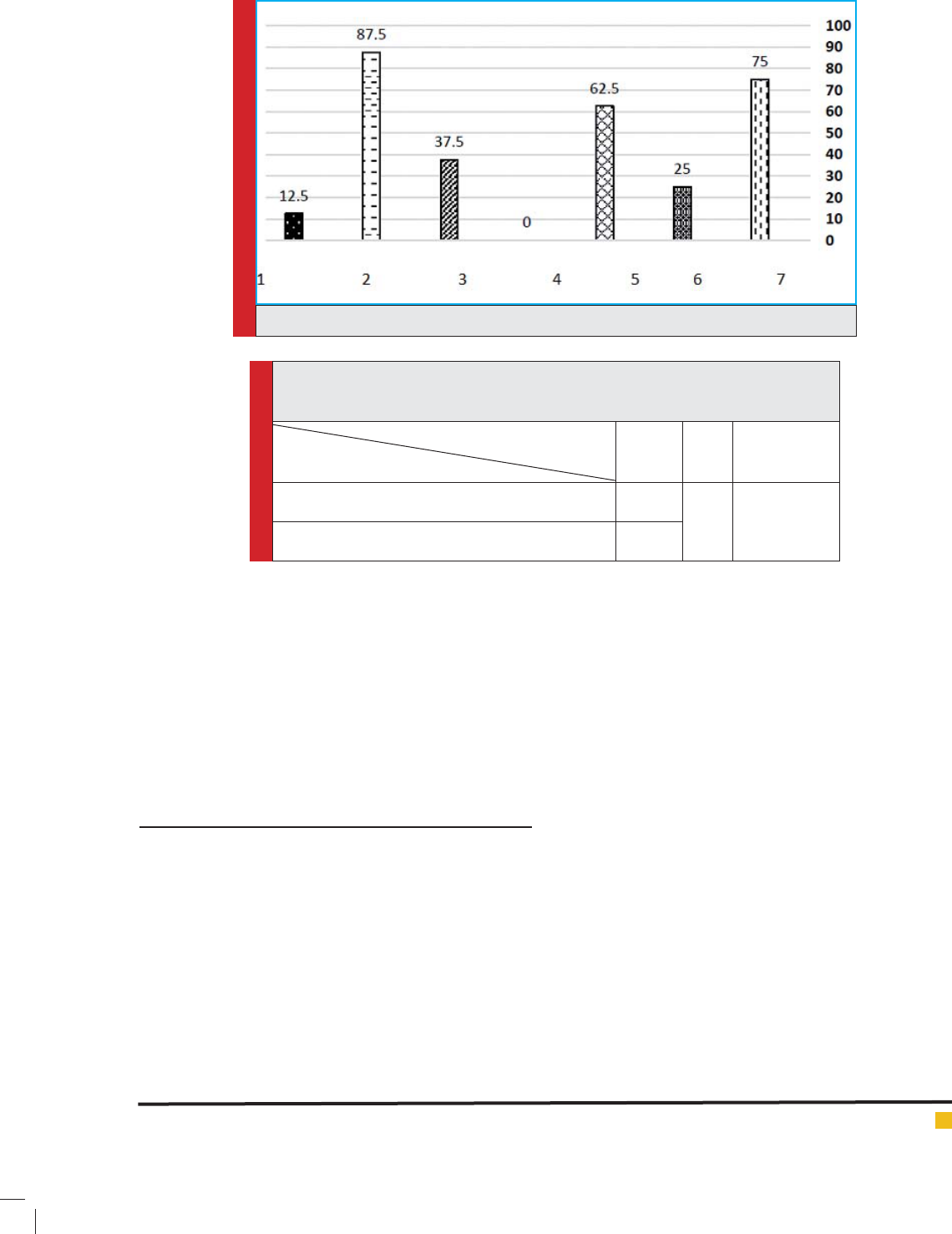
The above table shows that there is no signi cant dif-
ference between the average total per capita solid waste
per bed in hospitals in Bandar Abbas and the average
total per capita solid waste per bed set by the Ministry
of Health (p=<0.01 , t=1.922). The average total per cap-
ita solid waste generation in hospitals in Bandar Abbas
corresponds to the average total per capita solid waste
determined by the Ministry of Health.
DISCUSSION
Per capita waste production in hospitals studied in
Bandar Abbas was obtained 2.62 kg/b.d. In this study,
except ordinary wastes (1.5 per active bed per day, i.e.
57.25% of the total waste production), other wastes was
considered infectious that the amount of these wastes
is 1.12 kg/b.d, i.e. 42.74% of total wastes generated. In
a same study, entitled the hospital waste management
in hospitals in West Azerbaijan in 2007, the amount of
waste generated per bed per day had been equivalent
to 0.95 kg/b.d that the amount increased to 3 kg/b.d in
2012 that is consistent with the amount of waste gener-
ated in this study (2.62 kg/b.d) (2).
In the study of Dehghani et al that was done in hos-
pitals of Arak University of Medical Sciences, entitled
the review of medical waste management status, the
results showed that the rate of waste production is 4.42
kg/b.d, which is consistent with this study(Dehghani,
Azam, Changani, & Dehghani Fard, 2008). The results
also show that per capita waste generation was higher in
our study compared to the study of Al-Khatib et al with
0.59 to 0.93 kg/b.d medical waste production(Al-Khatib,
Al-Qaroot, & Ali-Shtayeh, 2009), study of A.B.Wahab
et al with 0.37 to 1.25 kg/b.d infectious waste in public
hospitals and 0.12 and 0.28 kg/b.d in private hospitals
(Wahab & Adesanya, 2011) and the study of Cheng.Y.W
et al with 0.19 to 0.88 kg/b/d infectious waste produc-
tion.
On the other hand, according to the results obtained
in this study, 57.25% of the ordinary wastes and 42.47%
of infectious wastes constitute the total wastes gener-
ated in the hospitals. The infectious waste generated in
this study compared to the Taghipoor’s study in Tabriz
were higher (29.4 percent)(Taghipour & Mosaferi, 2009).
The study of Farzad Kia et al in which the infectious
waste was 10 to 15 percent in Tehran educational hos-
pitals (Farzadkia, Moradi, Mohammadi, & Jor , 2009)
FIGURE 3. Separately storage management of Chemical, pharmaceutical and biological waste
Table 4. Comparing the total production of solid waste (infectious and non-infectious)
in the hospitals of Bandar Abbas with the regulations approved by the Ministry of
Health and Medical Education
Variables
Statistical indicators
Average t Signi cance *
Average per capita production of solid waste per active
bed in hospitals in Bandar Abbas
2.62
1.922 0.09
Average per capita production of solid waste per active
bed set by the Ministry of Health
2.7
Rahmanian, Ghavam and Yazdanpanah
170 STRUCTURE OF SOLID WASTE MANAGEMENT IN HOSPITALS OF BANDAR ABBAS CITY BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
is not consistent with this study. In a study of Davoodi
conducted in the hospitals of Mashhad, it was 34.90%
(Davoodi et al., 2014) and in the study of Alam MM et al,
it has been reported that the infectious waste (at a rate of
37%) is more than the present study (Alam et al., 2008).
Furthermore, in the study of Nemathaga F conducted
in South Africa and in Limpopo Province, the average
percentage of the components of medical wastes was
60.47% ordinary wastes and 30.32 % infectious wastes
that these results are almost consistent with the results
of this study(Nemathaga, Maringa, & Chimuka, 2008).
According to this study (Table 2), per capita waste pro-
duction in university hospitals is 2.38 kg/d, in private
hospitals is 2.26 kg/d, in police and military hospitals is
1.81 kg /d and in social security hospitals is 3.61 kg/d/b.
It seems that high per capita waste generation can be
due to the hospital inappropriate management struc-
ture, early replacement of hospital administrators and
inexperience of environmental health expert based in
the hospital.
According to the results of Figure 1, most waste stor-
age time in temporary sites is respectively in the police
and military hospitals with an average of 56 hours, in
Social Security hospitals with an average of 28 hours, in
private hospitals with an average of 23 hours and less
waste storage time is in the university hospitals with an
average of 21 hours. It seems that one of the reasons for
long-term accumulation of waste in public hospitals is
associated with the traf c problem of vehicles to col-
lect and transport waste in military areas as well as the
lower volume of daily waste than the volume of trucks
carrying the waste.According to Figure 4, in 62.5% of
hospitals, the pharmaceutical and chemical waste nal
disposal method is the sanitary land ll. In 25 percent of
these hospitals, the methods of container making and
piling up are used for nal disposal of the wastes and
in 12.5 percent of the hospitals studied, it is used other
methods. The sanitary land ll and incineration methods
are not used in any of the hospitals.
CONCLUSION
Lack of control and lack of attention to proper manage-
ment of hospital wastes on how to collect, store, trans-
port and dispose of such waste will lead to the preva-
lence of regional and urban epidemics and diseases and
waste of money that this is considered a serious threat to
the public health and environment. On the other hand,
due to urban sprawl and population growth, the pace
of creation of institutions and medical centers such as
the hospitals and paying attention to the management
of hospital wastes are necessary. Therefore, the present
study was conducted in this regard that the results of
this study showed total per capita waste generation in
hospitals of Bandar Abbas is 2.62 kg/b.d that 1.5 kg is
related to the household-like wastes (ordinary) and 1.12
kg belong to the infectious wastes including the sharp
waste, pharmaceutical waste, chemical and hazardous
wastes, pathological wastes and genotoxic waste.
According to the World Health Organization (2014),
which is approved by the Ministry of Health, 85% of
waste generated in hospitals are without risk or ordi-
nary and only 15 to 25% of them constitute the hazard-
ous waste. While in the hospitals studied, 42.74 percent
of hospital wastes are infectious and hazardous that
is more than the amount recommended by the World
Health Organization and the Ministry of Health. It seems
that this is often due to neglect and lack of awareness of
the environmental hazards and pollution and economic
losses caused by mixing the ordinary and infectious
wastes in all stages of production, transportation and
storage of waste in hospitals.
Based on the results of this study, we can conclude
that the per capita production of solid waste per bed
as well as the average duration of waste storage in the
temporary site of waste at hospitals of Bandar Abbas
is almost accordance with the standards recommended
by the World Health Organization and the Ministry of
Health. But there is no consistency in the waste compo-
sition, the infectious waste ratio to the total waste gen-
erated and the proportion of infectious and hazardous
waste in hospitals of Bandar Abbas is about 2 times the
amount recommended by the World Health Organization
and the Ministry of Health that it should be prevented
the mixing of infectious and ordinary waste, especially
in production by implementing more effective training
programs and making a commitment and responsibility
in all employees involved in the infectious waste pro-
duction and performing ongoing monitoring by manag-
ers and health experts in hospitals as well as the univer-
sity students in different elds in hospitals. Moreover,
it is necessary to force the hospital of cials and admin-
istrators in implementing the waste management rules.
OFFERS
With respect to the implementation of effective train-
ing programs for managers and personnel involved in
the production, transportation and disposal of hospital
waste, it is recommended at rst the training needs of
different groups involved in the production of hospital
wastes are determined based on scienti c principles and
then the required training programs are developed and
implemented based on these results.
In the educational needs of different groups based on
scienti c principles involved in the production of hospi-
tal wastes were determined and then based on the results
required training programs developed and implemented.

Rahmanian, Ghavam and Yazdanpanah
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS STRUCTURE OF SOLID WASTE MANAGEMENT IN HOSPITALS OF BANDAR ABBAS CITY 171
ACKNOWLEDGMENT
The authors thank and appreciate the sincere cooperation
of all managers, head nurses and health experts working
in hospitals of Bandar Abbas and also the health experts in
health center of Bandar Abbas and Hormozgan province.
REFERENCES
Al-Khatib, I. A., Al-Qaroot, Y. S., & Ali-Shtayeh, M. S. (2009).
Management of healthcare waste in circumstances of limited
resources: a case study in the hospitals of Nablus city, Pales-
tine. Waste Management & Research, 27(4), 305-312.
Alam, M. M., Sujauddin, M., Iqbal, G. M. A., & Huda, S. M.
S. (2008). Report: Healthcare waste characterization in Chit-
tagong Medical College Hospital, Bangladesh. Waste Manage-
ment & Research, 26(3), 291-296.
Chartier, Y. (2014). Safe management of wastes from health-
care activities: World Health Organization.
Davoodi, R., Eslami Hasan Abadi, S., Sabouri, G., Salehi, M.,
Ghooshkhanei, H., Rahmani, S.Gharaeian Morshed, M. (2014).
Medical Waste Management in the second largest City of Iran
(Mashhad) with Three-Million Inhabitants. Journal of Patient
Safety & Quality Improvement, 2(4), 160-164.
Dehghani, M., Azam, K., Changani, F., & Dehghani Fard, E.
(2008). Assessment of medical waste management in educa-
tional hospitals of Tehran university medical sciences.
Farzadkia, M., Moradi, A., Mohammadi, M. S., & Jor , S.
(2009). Hospital waste management status in Iran: a case study
in the teaching hospitals of Iran University of Medical Sci-
ences. Waste Management & Research, 27(4), 384-389.
Kumar, R., Samrongthong, R., & Shaikh, B. T. (2013). Knowl-
edge, attitude and practices of health staff regarding infectious
waste handling of tertiary care health facilities at metropolitan
city of Pakistan. Journal of Ayub Medical College Abbottabad,
25(1-2), 109-112.
Ndejjo, R., Musinguzi, G., Yu, X., Buregyeya, E., Musoke, D.,
Wang, J.-S Williams, P. (2015). Occupational health hazards
among healthcare workers in Kampala, Uganda. Journal of
environmental and public health, 2015.
Nemathaga, F., Maringa, S., & Chimuka, L. (2008). Hospital
solid waste management practices in Limpopo Province, South
Africa: A case study of two hospitals. Waste Management,
28(7), 1236-1245.
Nie, L., Qiao, Z., & Wu, H. (2014). Medical Waste Management
in China: A Case Study of Xinxiang. Journal of Environmental
Protection, 2014.
Rastegar, A., & Gholami, H. (2014). Survey of Solid Waste
Management in Small and Large selected Hospitals of Tehran.
www. sjimu. medilam. ac. ir, 22(2), 149-157.
Taghipour, H., & Mosaferi, M. (2009). Characterization of med-
ical waste from hospitals in Tabriz, Iran. Science of the total
environment, 407(5), 1527-1535.
Wahab, A., & Adesanya, D. (2011). Medical waste generation in
hospitals and associated factors in Ibadan Metropolis, Nigeria.
Res J Appl Sci Eng Technol, 3, 746-751.
WHO (2004). National Health-Care Waste Management Plan
2004 (pp. 7-23).
Zarei, F., Taghdisi, M. H., Keshavarz Mohamadi, N., & Tehrani,
H. (2013). Health Promoting Hospital: A pilot study in Bo-Ali
hospital, Qazvin, Iran. Journal of Fasa University of Medical
Sciences, 3(3), 215-223.