
Medical
Communication
Biosci. Biotech. Res. Comm. 10(4): 689-696 (2017)
Prevalence of the root canal treatment errors and its
related factors in patients treated by undergraduate
dental students
Dadresanfar B
1
, Mohammadzadeh Akhlaghi N
2
and Z. Khodabakhsh
3
*
1,2
Assistant Professor of Endodontic Department, Islamic Azad University, Dental Branch, Tehran, Iran
3
Postgraduate Student of Operative Department, Islamic Azad University, Dental Branch, Tehran, Iran
ABSTRACT
Since errors of root canal treatment can result in tooth loss, it is important to study effective factors on incident
of these errors. In recent years, aiming at reducing errors of root canal treatments and improving performance of
dentaldepartment in Islamic Azad University, Tehran, facilities were provided which included apex locator, teaching
Passive-step back in pre-clinic period and presence of professional assistants and professors who helped students.
Studying and investigating errors during treatment by students and providing proper preventative solutions increases
the chance of successful treatment of patients. According to the changes in methods of teaching root canal prepara-
tion and considering bene t that annual and biennale assessment of prevalence of errors during the treatment has
for studying educational performance and future planning, in this study we studied prevalence of errors during root
treatment by dental students in general dentistry major and its effective factors, in order to study whether these
applied changes reduced errors or not? Firstly, it is hypothesized that effective factors on this errors include qual-
ity of radiography, numbers of radiographies, patients’ age, type of tooth, type of jaw, canal curvature, periapical
lesion, student’s semester of the study, student’s gender, and numbers of treatment sessions, rst treatment of root
and second treatment of root. In this research 840 record of patients who had received root canal treatment in public
Endodontics sector were evaluated from 2010/9/23 to 2012/09/23. Firstly, two endodontists were calibrated in order
to make sure that kappa coef cientis positive and they both agreed on that, and then endodontists, separately, com-
pleted data forms pertinent to errors during root treatment and related factors. Prevalence of errors was identi ed in
the samples and then role of associated factors was evaluated by logistic regression as statistical test. And after rst
evaluation of records, sample of study consists of 613 teeth (1131 canals) which out of them 567 teeth received RTC
and 46 teeth received re treatment (Redo). Results indicated that there is statistical difference in frequency of errors
689
ARTICLE INFORMATION:
*Corresponding Author: Khodabakhsh_narges@yahoo.com
Received 27
th
June, 2017
Accepted after revision 27
th
Sep, 2017
BBRC Print ISSN: 0974-6455
Online ISSN: 2321-4007 CODEN: USA BBRCBA
Thomson Reuters ISI ESC and Crossref Indexed Journal
NAAS Journal Score 2017: 4.31 Cosmos IF: 4.006
© A Society of Science and Nature Publication, 2017. All rights
reserved.
Online Contents Available at:
http//www.bbrc.in/
DOI: 10.21786/bbrc/10.4/12
690 PREVALENCE OF THE ROOT CANAL TREATMENT ERRORS AND ITS RELATED FACTORS IN PATIENTS BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
Dadresanfar B et al.
INTRODUCTION
Root treatment, aiming at preventing periapical perio-
dontitis and improving periapical lesion, has been recog-
nized as a complicated treatment in dentistry treatments.
This treatment is conducted by removing necrosis pulp,
infectious pulp and batteries and via irrigation and pre-
paring canal, mechanical cleaning and also high qual-
ity obturation. Epidemiologic studies introduced errors
in mentioned procedure as the main reason of treat-
ment failures and imposing higher costs (Lynch 2006;
Mozayeni 2006; Yousuf, 2015). It has been indicated that
acceptable RCT refers to treatments in which root ll-
ings terminate within 2mm of the radiographic apex and
that are of adequate homogene density and without void
from crown to apical area (Bramanten 1987; Kulic 2011).
Applied method for studying quality of root treatment
is assessing PA Radiographs that are provided before
and after root treatments, radiographically (Kelbauskas
2009; Mosby Co. 2009). Literature review indicated that
errors rate varies from 10 to 58% in different centers
while prevalence of these errors rate in academic centers
(25-45%) is signi cantly higher than professional cent-
ers (10-16%) (Cohen 1998; Er 2006; Estrela, 2017).
Estrela1 et al (2017) performed a research titled as
“Common Operative Procedural Errors and Clinical Fac-
tors Associated with Root Canal Treatment”. They con-
cluded that in each phase of RCT, an operative error can
have adverse implication on prognosis, and these errors
show that risk factors lead to failure.Akbar (2015) per-
formed radiographic study of the endodontic treatment’s
problems and failures. His results illustrated that com-
pare to anterior and premolar teeth, endodontic prob-
lems and failures were most common in molars. The
most frequently canals with endodontic problems and
failures included Mesiobuccal, mesiolingual and dis-
tobuccal root canals. Finally, based on results he con-
cluded that the most common cause of endodontic treat-
ment failure was under lling followed by poor lling
and over lling and rst molar was the most frequently
involved tooth with endodontic problems and failures.
Yousuf, et al., (2015) studied endodontic procedural
errors and showed that the most frequently treated tooth
was right permanent mandibular rst molar. The least
commonly treated teeth were the permanent mandibu-
during rst root treatment and re treatment. In addition, factors including jaw type, tooth type, canal curvature, peri-
apical lesion, and student’s semester of study have signi cant effect on Non homogene-Exact lling length ‘Trans-
portation ‘Ledge’ Over lling’s error. However, numbers of treatment sessions was effective with low correlation.
Comparing frequencies of errors during root treatment in this study and paper, it was clari ed that adding tools such
as apex locator, teaching Passive-step back in pre-clinic period and presence of professional assistants and professors
who helped students reduces errors during root treatment.
KEY WORDS: DENTAL STUDENTS, RADIOGRAPHIC ENDODONTIC ERRORS, QUALITY OF ROOT CANAL TREATMENT
lar third molars. Bakhshi and Shahabi (2015) identi ed
the least mistakes compared to obturation phase, with
the most frequent errors including void, over lling and
imperfect cleaning.
A research was carried out by Kulic et al in 2011
in Serbia which indicated that 51.6% treatments were
acceptable with accurate working length and homogeny
density. In Fonseka et al (2015) study, it was reported
that 74.3% treatments were acceptable. In addition, in a
research in 2008 in Islamic Azad University, endodontics
department, Tehran, it was reported that 51.5% errors
happened during root canal treatment while 49.5% were
error-free. Most of the studies illustrated that highest
error incident was occurred in posterior teeth (Braman-
ten CM. 1987; Eleftheriadis GI. 2005; Khabbaz M.G.
2010) and factors including increasing instruction hours
reduces errors (Yousuf, W. 2015). Study and considera-
tion of students’ errors during treatment and providing
appropriate preventive ways increase treatment success
in patients (Bramanten CM. 1987) Recent years, facili-
ties including apex-locator, teaching Passive-step back
method in pre-clinic, presence of professional assistants
and professors who helped students were added into
endodontics department of Islamci Azad University in
order to reduce errors during treatment.
Based on literature review (Estrela, 2017; Lynch 2006;
Yousuf, 2015), popular errors during endodontic treat-
ments are as follow:
Last years equipment including teaching Passive-
step back method in pre clinic and presence of profes-
sional assistants helping students were applied in order
to reduce errors during treatment in endodontic sector.
According to the changes made in methods of teaching
root canal preparation and considering the bene ts that
annual and biennale assessment of prevalence of errors
during the treatment has for studying educational per-
formance and future planning, thus due to lack of infor-
mation about the subject in endodotics sector of Islamic
Azad University, Tehran, and also because of differences
and lacks of previous researches (Er O. 2006 and You-
suf 2015), studying students’ error during treatment and
providing proper methods increase chance of successful
treatment of patients. This study, therefor, investigates
prevalence of errors during root trees and related factors
in patient referring to endodontics sector of Islamic Azad
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS PREVALENCE OF THE ROOT CANAL TREATMENT ERRORS AND ITS RELATED FACTORS IN PATIENTS 691
Dadresanfar B et al.
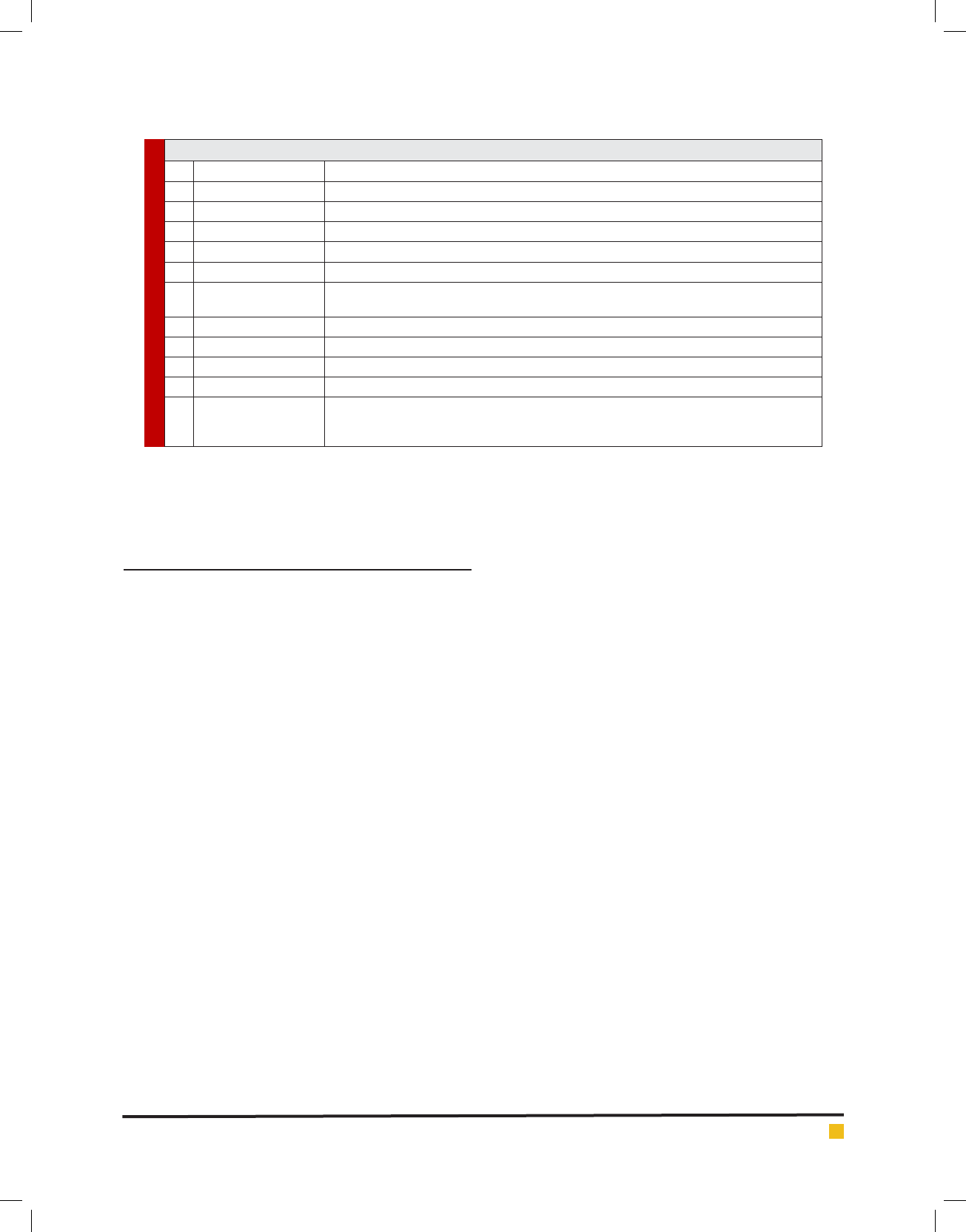
Table 1. popular errors during endodontic treatments are as follow
Error type Description
1 Under lling Space between canal obturation and radiographic apex is more than 2 mm
2 Over lling Radiographic beyond apex lling
3 Non-homogen Lack of homogene density of lling material from coronal area to apical area
4 Ledge Deviation from main path of canal and creating one step in some cases is cause of under lling
5 Transportation Deviation from main path of canal and nding new path in root
6 Zipping Perforation of apical area which results in reverse cone and it disrupts apical seal
7 Strip perforation Association of pulp space with periodontal space in root branching region
8 Cervical perforation Association of pulp space with periodontal space in cervical region of tooth
9 Forcation perforation Association of pulp space with periodontal space in forcal region of tooth
10 Broken Instrument Broken instrument that is not extracted from canal
11 Gouging Over
Opening cavity more than required space due to not locating grinder in longitudinal axis of
tooth or futileattempt for accessing to the pulp
University, Tehran, during 2010-2012 in order to nd out
whether these applied changes reduced error or not?
MATERIALS AND METHODS
All people who received root treatment from 2010/9/23
to 2012/09/23 in public Endodontics sector in Islamic
Azad University; Tehran belonged to the population
of the current study. Then, out of endodontics sector
records’ list that belonged to two years and was gathered
statistically, accurate records were selected and studied.
In this study, research method was performed by exist-
ing data which collected by observation and ling infor-
mation forms. In addition, samples were selected statis-
tically from all treated patients by dentistry students in
general coarse. Out of 840 selected records, 227 records
(27%) were eliminated due to poor radiography quality
(182 records, 21.6%) and lack of suf cient radiography
(45 records, 5.3%).
Records that lacked nal radiography, or did not
contain at least both diagnostic and nal radiography
and also records that, in spite of second recording, their
radiographic quality was poor were eliminated from
the study. Lack of radiography quality happens due to
manual radiography developing and xing by student
in public sector of endo which results in over developing
the lms, insuf cient xing, and lack of PA Radiographs
quality. Assessing quality of student’s performance in
root treatment procedure was conducted in two steps
including preparation and root canal obturation based
on recorded radiographic images in patients’ records.
Nevertheless, there are 2 dimension images instead of
3 dimension structures, this system has been applied in
different studies (Cohen 1998; Guttman 1997).
Assessing images of all records was conducted by two
experts from university endodontic sector, separately,
by microscope with at times enlargements and desktop
negatoscope. Before study, observers agreed on similar
interpretation for radiographic PA Radiograph after per-
forming an experiment. Evaluators were calibrated and
Kappa coef cient was reported as 0.88 which proved
there is perfect coef cient of agreement among evalu-
ators. Due to perfect coef cient of agreement among
evaluators, mentioned samples were assessed again in
cases with no agreement among observers. This method
was utilized by Khabbaz et al. (2010).
For PA Radiograph homogenization by observers, ray
radiation direction considered mesial in all radiogra-
phies. Poor radiographies were xed again and reevalu-
ated. Records which lacked 2 diagnostic and nal radi-
ographies were eliminated. Two endodontists conducted
diagnostic and nal radiographies and used microscope
at ve times enlargement and one negatoscope. In addi-
tion, some rare errors mentioned in the record and they
were not observable in radiography but they were men-
tioned in the record were studied. Firstly, errors’ evalu-
ators explained errors, thencoef cientof concordance
(Kappa) were identi ed and then records’ assessment
was started. Evaluators were calibrated in order to make
sure that Kappa coef cient is positive and they are com-
patible. For preventing errors of answers, each endo-
dontist lled data forms separately and then errors that
endodontist were agreed upon considered as real error.
In cases that observers did not agree on, due to perfect
coef cient of agreement between evaluators, mentioned
samples were reassessed and evaluators agreed on that.
In epidemiologic studies, there are different standards
for categorizing root treatment quality. The most preva-
lent parameters of acceptable treatment categorization
Dadresanfar B et al.
692 PREVALENCE OF THE ROOT CANAL TREATMENT ERRORS AND ITS RELATED FACTORS IN PATIENTS BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
are length of root canal lling, lling homogenization
without void, and absence of iatrogenic errors (Cohen
2006; Haji-Hassani, 2015; Mozayeni 2006). In this study,
standards of determining radiographic categorization of
root treatment were based on length and density of ll-
ing in the absence of iatrogenic errors and they were
categorized into two acceptable and unacceptable treat-
ments.
The lling material ends 0-2 mm shorter than radio-
graphic apex with no visible voids within the material
or between the material and root canal walls. 2) Unac-
ceptable treatments: A) the lling material ends more
than 2mm from radiographic apex or beyond the radio-
graphic apex. B) Visible voids within or between lling
material and root canal walls
1. Acceptable treatment: under lling is 0-2 mm and
density of lling material is homogene with no
visible void within the material or between crown
and apical area. Besides no observable iatrogen-
icerror is in patient’s record and in canals.
2. Unacceptable treatment
a. The lling material ends more than 2mm from ra-
diographic apex or beyond the radiographic apex
b. Density of lling material in not homogene and
there is void between crown to apical area.
c. Iatrogenic error is observed in canals and it is also
reported in pateint’s record.
In addition, in this study we assessed demographic
information of students (gender, and the semester) and
factors pertinent to patient and tooth including patient
gender, age, tooth location, tooth root numbers, canal
numbers, periapical radiolucencies, canal curvature and
treatment sessions numbers.
RESULTS AND DISCUSSION
Results indicated that 61% rst treatments (RCT) were
acceptable and 39% had errors during root treatment.
Acceptable treatment which consists of exact length of
lling and proper density of lling and no incidence of
iatrogenic errors, in anterior teeth was 75.6%, in pre-
molar was 72% and in molars was 38.4%. Redo were
acceptable for 100% cases and the most prevalent redo
tooth was Mandibular second premolar. Previous short
lling was identi ed as the most common cause of redo.
In table 2, there is information about frequency of
errors during root treatment in patients who received
treatment by dental students in general coarse in endo-
dontics sector of Islamic Azad University, dentistry
department, during 2010-2012. In addition, table 2 indi-
cates frequency of errors during root treatment associ-
ated to relevant factors.
Based on table 2 and table 3 and results of logistic
regression, it is concluded that:
1. 55% studied canals had curvature which it was
more in molar teeth. 24.2% canals with curva-
ture had errors during root treatment. 14.5% tooth
that received RCT had periapical lesion which was
more in mandibular rst molar. 47% canals had
periapical error during treatment.
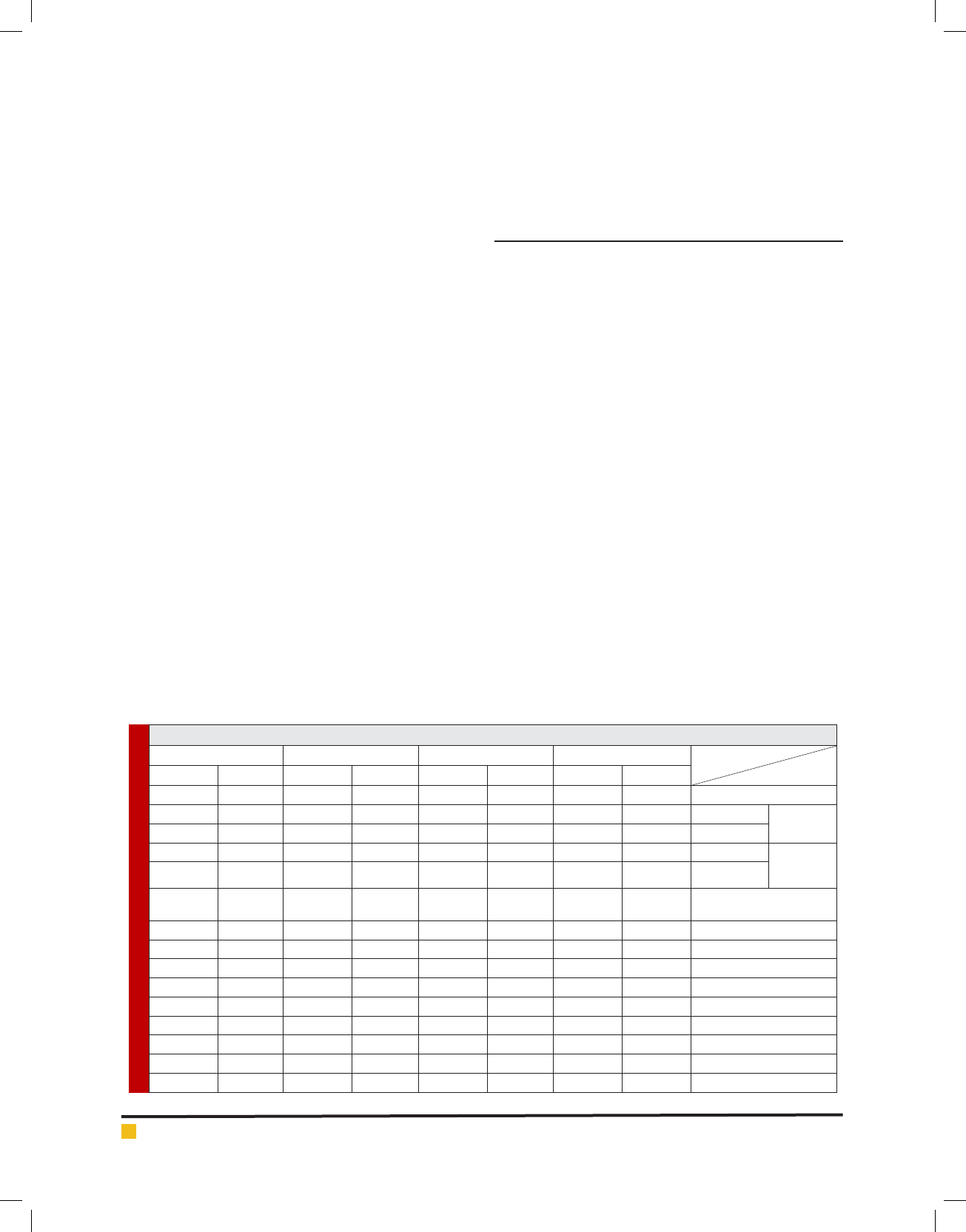
Table 2. Prevalence of errors during root treatment
total Molar premolar anterior
Error type
Tooth type
Percentage Frequency Percentage Frequency Percentage Frequency Percentage Frequency
100 7 42.8 3 28.6 2 28.6 2 Broken instrument
100 40 67.5 27 20 8 12.5 5 Homogen Over lling
Root canal
100 22 59 13 32 7 9 2 Nonhomogen
100 35 45.7 16 25.7 9 28.6 10 Homogen Under
Filling
Root canal
100 28 67.8 19 21.4 6 10.8 3 Nonhomogen
100 102 60.8 62 23.5 24 15.7 16 Nonhomogen- Exact lling
length Root canal
0 0 0 0 0 0 0 0 Forcal Perforation
0 0 0 0 0 0 0 0 Cervical Perforation
100 5 100 5 0 0 0 0 Strip Perforation
100 9 100 9 0 0 0 0 Strip preparation
100 25 52 13 16 4 24 6 Ledge
100 54 72.2 39 18.5 10 9.3 5 Transportation
100 4 75 3 25 1 0 0 Zipping
100 6 0 0 33.3 2 66.7 4 Gouging
100 567 35.8 203 35.9 204 28.2 160
Dadresanfar B et al.
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS PREVALENCE OF THE ROOT CANAL TREATMENT ERRORS AND ITS RELATED FACTORS IN PATIENTS 693
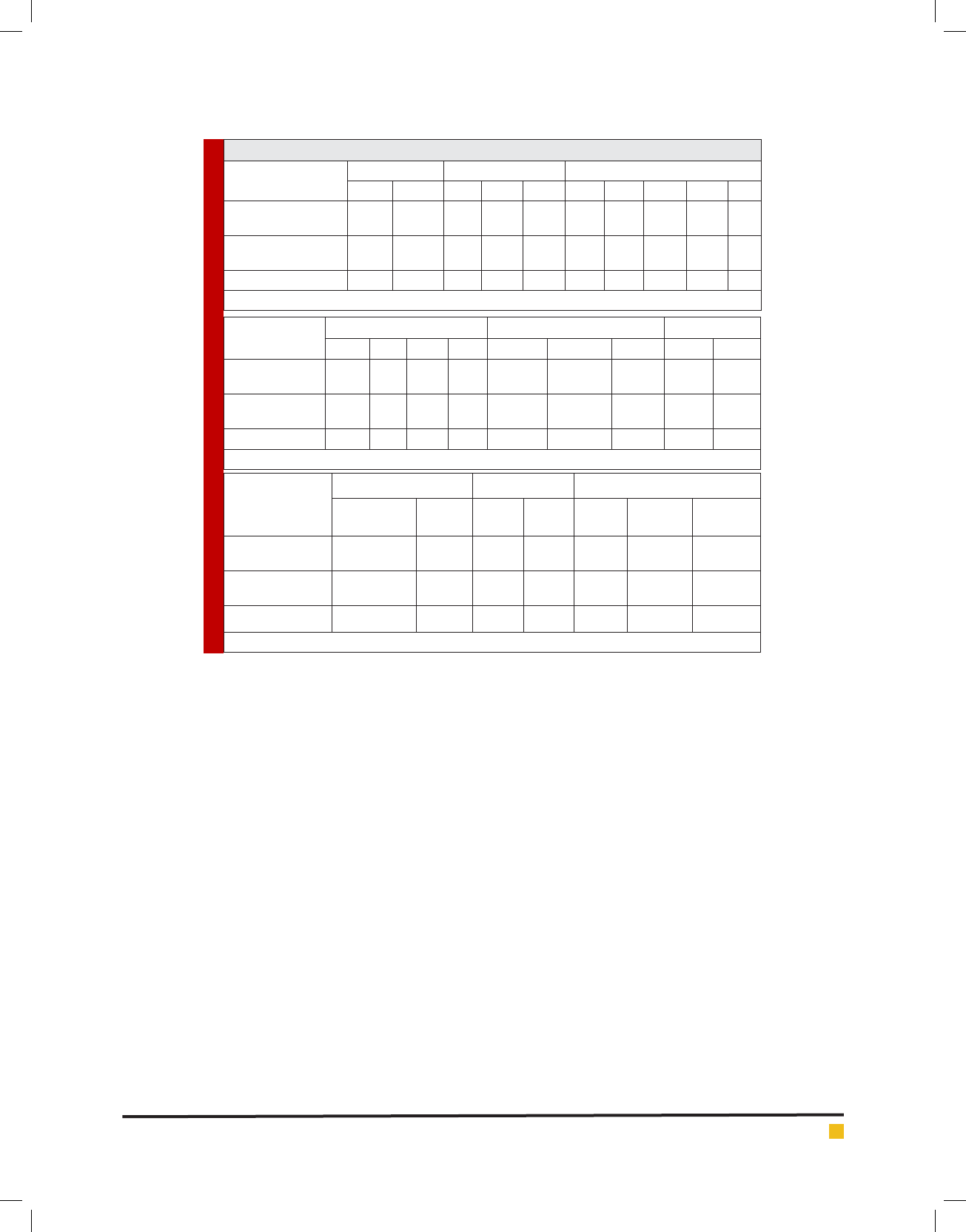
Table 3. related factors to errors during treatment
Related factors Error gender manual endo coarse Numbers of treatment sessions
male Female two three four one two three Four Five
No error 148
61.7
197
60.3
192
71.9
96
60
59
41.1
112
70.4
185
63.8
45
44.1
4
28.6
1
50
With error 92
38.3
130
39.7
75
28.1
64
40
81
57.9
47
31.6
105
36.2
57
55.9
10
71.4
1
50
Total 240 327 267 160 140 159 290 102 14 2
(A)
Related factors
Error
Canal numbers Tooth type Jaw type
one two three four anterior Premolar molar lower upper
No error 205
75.3
69
67.6
64
40
9
28.1
121
75.6
147
72
78
38.4
125
53.9
221
66
With error 68
24.7
23
32.4
96
60
23
71.9
39
24.4
57
28
125
61.6
107
46.1
114
34
Total 273 92 160 32 160 204 203 232 335
(B)
Related factors
error
Canal curvature lesion PA Patient age
Direct canal Curved
canal
With
error
No
error
Under
30
Between
30-45
Older
than 45
No error 412
84.1
451
75.8
44
53
819
81.7
143
60.3
123
57.5
80
69
With error 78
15.9
144
34
39
47
183
19.3
94
39.7
91
42.5
36
31
Total 490 335 83 1002 237 214 116
(C)
2. 39.7% treatments conducted by female students
and 38.3% performed by male students had errors
during the treatment. But there was no signi cant
difference between students’ gender and errors
during treatment (p>0.05).
3. 71.4% four sessions treatment and 29.1% one ses-
sion treatment had errors during the treatment. It
means that there was signi cant difference be-
tween errors rate during treatment and treatment
sessions number (p<0.001). However, considering
correlation coef cient (= 0.21), this relationship
was poor.
4. Considering root treatment error, there was sig-
ni cant difference between two jaws (p=0.004).
Regarding that its incidence in mandibular teeth
was signi cantly more than maxillary teeth (34%).
Considering correlation coef cient, = -0.12, this
error was more prevalent in mandibular than up-
per jaw.
5. Error incidence rate by students in manual endo
coarse 2 was identi ed 28.1%, by manual endo
coarse 3 was 40%, and by manual endo coarse
4 was 57.1%, which indicated that there is sig-
ni cant relationship between errors during treat-
ment and students study in manual endo coarse
(p<0.001) and considering correlation coef cient,
= 0.52, this relationship was average.
In addition, results obtained from prevalence of errors
during treatment indicated that:
a. Non homogen-Exact llng length was identi ed
in 13.4% canals (145 canal) as the most prevalent
error in root lling procedure ( lling with in ade-
quate quality in exact length of function). This er-
ror was signi cantly more prevalent in molar teeth
canal (60.8%) than premolar and anterior teeth
(p<0.001) but considering correlation coef cient,
= 0.25, this relationship was poor. This error was
35.3% in mandibular molars and 25.5% in maxil-
lary molars. Highest prevalence was identi ed in
mandibular molars and mesiobacal canal (18%)
and then it was observed in mesiolingual (17.2%).
b. In eld of errors during root canal preparation,
the most common error was transportation which
was observed in 9.5% teeth (54 teeth) highest
rate of this error happened among molars which
prevalence rate was 72.3% and highest preva-
lence happened in mesiobacal canal of mandib-

Dadresanfar B et al.
694 PREVALENCE OF THE ROOT CANAL TREATMENT ERRORS AND ITS RELATED FACTORS IN PATIENTS BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
ular rst molar. There was signi cant relation
between transport and canal curvature (p<0.05).
However, considering correlation coef cient, =
0.1, this relation was weak. There was signi cant
difference in transport incidence among molar
teeth (72.2%) and premolars (18.5%) and anteriors
(9.3%) (p<0.05).
c. Second prevalent error during canal preparation
was ledge which was observed 4.4% of total teeth.
There was signi cant relation between canal ledge
and curvature (p<0.05) however considering cor-
relation coef cient, = 0.06, this relation was
poor. In molar teeth, error prevalence was 52%
which was more than pre molar and anterior teeth.
In addition, ledge prevalence was signi cantly
higher in mandibular (40%) than maxillary (12%)
(P<0.005). Highest rate of error happened in rst
mandibular (32%) and mesial root and it is ob-
served equally in mesiobacal canals (25.6%) and
mesiolingual (25.6%).
d. Over lling has been studied in 6.8% canals and
it was identi ed that 4.2% were over homogene
and 2.6% were over non-homogene. the highest
prevalence rate happened in mesiolingual canals
of mandibular molars. Signi cant difference was
observed in over lling and teeth with priapical
lesion (p<0.05) however considering correlation
coef cient, = 0.08, this relation was very poor.
e. Foracal Perforation and Cervical Perforation were
not observed. 6 Strip Perforation cases, 7 Broken
Instrument cases, 4 zipping cases, 6 Gouging cases
and 9 Strip Preparation cases were identi ed and
there was not signi cant relationship with related
factors.
In this study, maximum error happened in root ll-
ing step, Non homogen-Exact lling length ( lling with
inadequate quality in exact length of function) and the
most prevalent error in eld of errors during root canal
preparation was transportation error. Second prevalent
error during canal preparation was ledge. In this study,
613 teeth including 1131 canal were evaluated which
consists of 567 teeth which received RCT and 46 teeth
received retreatment. Acceptable treatment in ante-
rior teeth was 75.6%, 72% in premolars and 38.2% in
molars. 100% redo were identi ed as acceptable treat-
ment and the most prevalent retreated tooth was man-
dibular second premolar and under- lling was identi ed
as the most prevalent cause of retreat.
In this study, similar to Kulic et al (2011), multi root
teeth which had error during treatment, even in one
canals, was considered as unacceptable treatment. Unal
et al (2011) reported highest prevalence of acceptable
treatment in anterior teeth was 90.1% and the least
prevalence was reported in 46.6% molars. In 71% ante-
rior teeth, 61% premolars and 30% molars were reported
as acceptable treatment prevalence by Khabbaz et al
(2010). In current study, 61% treatments were acceptable
and 39% treatment were unacceptable. Acceptable treat-
ment in anterior teeth was 75.6%, in premolars was 72%
and in molars was 38.2%.
Mozayeni et al (2006) reported that the most preva-
lent error during root canal preparation was transporta-
tion. In addition, Dadresanfar et al (2008) reported that
transport prevalence was 27.5%. Statistical difference
of these ndings can be due to applying Passive-step
back preparation method in pre clinic coarse, applying
Gates-Gliden drills for coronal preparation of root which
reduces coronal interferences from deviation of rst
path canal and also due to professional assistance and
their help to students. High prevalence of transportation
in molar teeth its signi cant difference with anterior and
pre molar teeth can be due to complicated anatomy of
these teeth, high numbers of canals and curvature of
canals in these teeth. There was signi cant statistic rela-
tionship between root canal curvature and transporta-
tion which shows there is potential effect of root canal
curvature on canal displacement. Lack of attention to
canal curvature, not providing Pre curve to les during
preparation of curved canals and lack of removing inter-
ferences of root canal Ori ces can be reasons of high
transportation rate in canals.
Second prevalent error during anal preparation was
ledge. Al-Kahtani et al reported that ledge prevalence
was 7.5% which is compatible with current study.
Eleftheriadis et al reported that ledge prevalence in
molars were 34.9% which is caused by step-back technic
and curvature of molar canals. Less prevalent of ledge
in this study can be due to using other canal preparation
technics including Passive-step back and applying les
with higher exibility such as Flexo File by dentistry
students.The most prevalent error during root lling was
Non homogen-Exact llng length. More errors in molars
can be because of lack of adequate access of students
to these teeth and in adequate canal aring which is
caused by their stress for bad incidents. Because inad-
equate canal aring prevents suitable penetration of
spreader, especially stainless spreaders, which will cause
bad lling density.
Er et al (2006) reported that 48.8% lling had inad-
equate density. In addition, Khabbaz et al (2010) stated
that 33.5% lling had inadequate density and Kulic L
et al (2011) in 25% and Dadresanfar et al reported that
29.2% lling had inadequate density. Statistical dif-
ference of these results with mentioned studies can be
stemmed from increase of assistants and professors’

Dadresanfar B et al.
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS PREVALENCE OF THE ROOT CANAL TREATMENT ERRORS AND ITS RELATED FACTORS IN PATIENTS 695
numbers and continuous study of patients during treat-
ment by professors via providing constancy control
radiographies during obscuration which reduces preva-
lence of errors during canal lling.
Maximum error prevalence of over lling was nd
out in mesiolingual canal of mandibular molars and
there was signi cant statistical difference between over-
lling and teeth with periapical lesion, because periapi-
cal lesion root top resorption so students cannot deal
with length control easily then it ends to over lling. Kel-
bauskas et al (2009) reported that 5.42% had over lling
which was compatible with this study. Kulic et al (2011)
reported3.3% over lling which this low prevalence can
be due to less numbers of their samples (306 canal). Er
et al (2006) reported 13% over lling cases and Khabbaz
et al reported 22.6% over lling. Statistical difference of
current studies with those can be due to studying more
canals in samples (1109 canals).
Highest rate of under lling error happened in Mesio-
bacal canal of mandibular molars. It can be due to
higher rate of transportation and ledge in molars which
results in diversion from main canal path and interfer-
ence in lling steps. In addition in Step-back technic
there is possibility of debris and dentin debris packag-
ing in apex top so there is no way for lling with exact
length. Kelbauskas et al (2009) reported that in 10.5%
cases, underi lling happened. They also reported that
the main reason is ledge and debris packaging.
CONCLUSION
It seems that using tools such as apex locator, presence
of professional assistants and attention of professors of
the related sector and also applying Passive-Step back
in curved canals by some students reduces preparation
error rate and errors of root canal ling. However utiliz-
ing more exible les, emphasizing on before-during-
and after treatment radiographies, meticulous super-
vision of professors during treatment and presence of
lower semester students with higher semester students
and professional assistants in third and second year of
experience could be considered as a guide for increasing
quality of root treatments and reducing errors.
REFERENCES
Barriesh-Nusair KM, Al-omari MA, Al-Hiyasat AS. (2004).
Radiographic technical quality of root canal treatment per-
formed by dental student at the Dental Teaching Center In Jor-
dan. J Dent 3:301-7
Bramanten CM, Berbert A, Barges RP. (1987). A Methodology
for Evaluation of Root Canal Instrumentation. Endod J 13:
243.
Cohen S, Burns RC. (1998). Pathways of the pulp,7 th
ed,Missouri, Mosby. ch8:209.
Cohen S, Burns RC. (2006). Pathways of the pulp. 9th ed. St.
Louis: Mosby, Elsevier. ch26:1025-1026, ch9:327
Dadresanfar B, Mohammadzadeh Akhlaghi N, Vatanpour M,
Atef Yekta H. (2008). Technical quality of root canal treatment
performed by undergraduate dental students. Iranian Endo-
dontic J 3:73-78
Eleftheriadis GI, Lambrianidis TP. (2005). Technical quality of
root canal treatment and detection of iatrogenic errors in an
undergraduate dental clinic. Int Endod J 38:725-34.
Er O, Sagsen B, Maden M, Cinar S, Kahraman Y. (2006). Radio-
graphic technical quality of root canal lling performed by
dental students in Turkey. Int Endod J, 39, 867-72
Estrela, C., Pécora, J. D., Estrela, C. R., Guedes, O. A., Silva, B.
S., Soares, C. J., & Sousa-Neto, M. D. (2017). Common Opera-
tive Procedural Errors and Clinical Factors Associated with
Root Canal Treatment. Brazilian Dental Journal, 28(2), 179-
190.
Farzaneh M, Abitbol S, Friedman Sh. (2004). Treatmen Out-
come in Endodontic: The Toronto study. Phases 1 and 2:
Orthograde Retreatment. Endod J 30:627-33
Friedman Sh, Abitbol S, Lawrence H. (2003). Treatment Out-
come in Endodontics: The Toronto Study. Phase 1: Initial
Treatment. Endod J 29:787-93
Guttman J, Dumsha T, Lovdahl P, Hovland E. (1997). Problem
solving in endodontics 3th ed mosby U.S.A, 5-6
Haji-Hassani, N., Bakhshi, M., & Shahabi, S. (2015). Frequency
of Iatrogenic Errors through Root Canal Treatment Procedure
in 1335 Charts of Dental Patients. Journal of international oral
health: JIOH, 7(Suppl 1), 14.
Ingle J, Bakland L (2008). Endodontics. 6th Ed. Ch27:921
Javidi M, Shoja Razavi A, Esmaieli H. (2006). A Comparision
between conventional and digital radiography in estimating
the working length of root canal. J Dent, 30:30-44
Kelbauskas E, Andriukaitien L, Irena N. (2009). Quality of root
canal lling performed by undergraduate students of odontol-
ogy at Kaunas University of Medicine in Lithuania. Stomato-
logic, Baltic. Dental and Maxillofacial J 1:92-96
Khabbaz M.G, protogerou E., douka E. (2010). Radiographic
quality of root llings performed by undergraduate students.
Int Endod J 43:499-508
Kulic L, Nogo-Zivanovic D, Krunic J, Vujaskovic M, Stojanovic
N. (2011). Radiological Assessment of the Quality of Root Canal
Filling in Teeth Endodontically Treated at Students’ Practical
session. Serbian Dent J; 3:139-143
Lynch CD, Burke FM. (2006). Quality of root canal lling per-
formed by under graduate dental students on single rooted
teeth.Eur J Den;10:67-22
Mozayeni MA, Asnaashari M, Modaresi J. (2006). Clinical and
radiographic evaluation of procedural accidents and errors
during root canal therapy. Iranian Endodontic J 97-100

Dadresanfar B et al.
696 PREVALENCE OF THE ROOT CANAL TREATMENT ERRORS AND ITS RELATED FACTORS IN PATIENTS BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
Pratten DH, McDonald NJ. (1996). Comparison of radiographic
and electronic working lenghts. J Endod; 22:173.
CV Mosby Co. (2009) Toronto; Ch18:322
Unal GC, Kececi AD, Kaya BU, Tac AG. (2011). Quality of root
canal llings performed by undergraduate dental student. Eur
J Dent 3:324-30
Yousuf, W., Khan, M., & Mehdi, H. (2015). Endodontic proce-
dural errors: frequency, type of error, and the most frequently
treated tooth. International journal of dentistry, 2015.
Zinman EJ. (2002). Records and legal responsibilities. In: Cohen
S, Burns RC, editors. Pathways of the pulp. 8th ed. St.Louise:
Mosby; P. 400.