
Genetic basis of poor scholastic performance among
children: A review
Kavita Singh, Dinesh Parmar and CBS Dangi
Department of Biotechnology, RKDF University, Bhopal (Madhya Pradesh) India
ABSTRACT
This paper presents concise reviewon selective pioneering works and recent progress on the topic genetic basis of
poor scholastic performance among children. Formal school education plays a great role in everyone’s life. Poor
scholastic performance may be the result of Intellectual disability or mental retardation which manifests under age
18. Interaction of certain genes and environmental conditions can result in intellectual disabilities. This provides
ample de nitions of concepts, classi cation, causes and consequences, prevalence, and involvement of chromosomes
in mental disability cases. This reveals that the magnitude of genetic variations in mental de ciency and scholastic
performance of children suggests strong genetic component.
KEY WORDS: SCHOLASTIC PERFORMANCE SCHOOL CHILDREN GENETIC REASONS
766
Genetical
Communication
Biosci. Biotech. Res. Comm. 11(4): 766-772 (2018)
INTRODUCTION
Formal school education plays a great role in every-
one’s life. Unsettled poor scholastic performance poses
instant and lifelong unfavorable effects on a child and
adolescent’s growth and cognitive development. Opti-
mum cognitive development of a child in uences his/
her learning behavior which is in uenced by interac-
tion of family, society, psychology, education, and eco-
nomical atmosphere of the child. Poor scholastic perfor-
mance is observed among some children (Carlson and
Corcoran, 2001; Landry, 2014). Interactions of Gene and
environment can result in different disease phenotypes
and intellectual abilities (McKusick, 1983; Deary, 2012).
All traits of an individual are products of heredity and
environ ment interaction. Individuals with varied gen-
otypes appear differently by exposure to the common
environmental factors (Davies, 2016). Intelligence was
one of the rst human traits to be the target of genetic
research even before psychology emerged as a scien-
ARTICLE INFORMATION:
Received 6
th
Oct, 2018
Accepted after revision 25
th
Dec, 2018
BBRC Print ISSN: 0974-6455
Online ISSN: 2321-4007 CODEN: USA BBRCBA
Thomson Reuters ISI ESC / Clarivate Analytics USA
Mono of Clarivate Analytics and Crossref Indexed
Journal Mono of CR
NAAS Journal Score 2018: 4.31 SJIF 2017: 4.196
© A Society of Science and Nature Publication, Bhopal India
2018. All rights reserved.
Online Contents Available at:
http//www.bbrc.in/
DOI: 10.21786/bbrc/11.4/29

BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS GENETIC BASIS OF POOR SCHOLASTIC PERFORMANCE AMONG CHILDREN: A REVIEW 767
Kavita Singh, Dinesh Parmar and CBS Dangi
ti c eld. The correlation between DNA sequence and
behavioral differences such as intelligence is considered
causal because DNA variations can lead to behavioral
differences but behavioral differences do not change
DNA sequences (Deary et al., 2006; Sniekers et al., 2017).
Intellectual disability and Poor Scholastic Performance
The“poor scholastic performance” is a broad term and
de ned differently by scholars. Okoye (1982) de ned
poor scholastic performance as one in which a student
is not successful in attaining standard performance in a
speci ed evaluation exercises involving a test, an exam-
ination or a set of constant assessment. Poor scholastic
performance may be the result of Intellectual disabil-
ity or mental retardation which manifests under age 18.
American Association on Mental Retardation (AAMR)
and American Psychiatric Association (APA) de ne
mental retardation on the basis of certain formulations
developed by them. This refers to extensive limitations
in functioning characterized by radically sub-average
intellectual level, existing concurrently with limitations
in two or more of the following adaptive skill areas:
communication ability, self-care, social skills, self-direc-
tion, community use, health and safety, leisure, home
living and work (Luckasson et al. 1992).
The AmericanPsychiatricAssociation (APA) is respon-
sible for naming, de ning, and describing mental dis-
orders. Fifth edition of the Diagnostic and Statistical
Manual ofMentalDisorders (DSM-5), APA changed the
term mental retardation and proposed the new term intel-
lectual disability or intellectual developmental disorder.
De nition of Concepts
De ning mental retardation remains a challenge and a
matter of controversy. Ever since people have been able
to distinguish mental retardation from other forms of
mental disability, a central theme of de nitions has con-
cerned the failure of mentally retarded persons to adapt
adequately to their surroundings. Older de nitions were
couched in terms of adult behavior, and there was a ten-
dency to avoid precise criteria for deciding in borderline
instances.
Many writers have attempted to specify quantita-
tive standards for deciding mental subnormal level. The
most widely used objective criterion of this sort has
been the score obtained on a standardized test of intel-
ligence such as the Stanford-Binet Intelligence Scale or
the Wechsler Intelligence Scale for Children (WISC). In
1916, Terman introduced a grouping of ability accord-
ing to IQ’s obtained on the Stanford-Binet (Terman and
Merrill, 1937). This system became widely used and, in
fact, became the standard classi cation system (Table
1). An IQ of 70 has gained considerable popularity as a
cutoff score for the retarded group.
Doll (1953) provided more speci c de nition. In addi-
tion to the element of social adaptation, he emphasized
the emergence of handicap in childhood, its constitu-
tional nature and its incurability. He considered some
criteria generally considered essential to an adequate
de nition and concept. These involve social incompe-
tence, mental sub-normality, developmentally arrested,
obtained at maturity, constitutional origin and essen-
tially incurable. Tredgold (1956) de ned mental de -
ciency as a state of incomplete mental development of
such a kind and degree that the individual was incapable
of adapting himself to the normal environment of his
fellows in such a way as to maintain existence indepen-
dently of supervision, control or external support.
The American Association on Mental De ciency
de nes mental retardation as a signi cantly sub-aver-
age general intellectual function existing concurrently
with de cits in adaptive behavior, and manifested dur-
ing the developmental period. In this de nition the
retarded person is judged in terms of his success with
the developmental tasks appropriate for his age: in the
preschool period sensorimotor behaviors assume great-
est importance, while during the school years academic
ability is of rst interest, and during adulthood eco-
nomic independence and social recognition (Suess et al.,
1983; APA, 2000). Furthermore, this de nition makes
it clear that a designation of mental status should be a
description of present behavior and implicitly disowns
the notion of potential intelligence.
There are a number of dif culties with these scoring
criteria. Because an IQ is simply a score obtained on the
basis of a restricted sample of behavior, there are signi -
cant limitations as to what can or should be expected of
it, even if the tests are perfectly reliable and children are
always able to put forth their best efforts. Furthermore, no
cutoff score will ever be adequate to de ne mental retar-
dation independent of the setting in which the individual
nds himself. Different skills and abilities are required at
different ages and in different environments. Retardation
must therefore be gauged in large part against current
environmental demands, (Reschly et al., 2002).
Apart from this, the cutoff scores for measures of
intellectual function are better recognized than the cutoff
scores for measures of adaptive behavior. There is open
agreement in the major diagnostic systems that perfor-
mance on the intellectual dimension must be approxi-
mately two or more standard deviations below the popu-
lation mean, which translates into an IQ score of 70 or less
on measures with a mean of 100 and a standard deviation
of 15 (Reschly et al. 2002; Greene et al., 2004).
Classi cation systems
Mentally Retarded or intellectually disabled individu-
als comprise a very heterogeneous group both in their
768 GENETIC BASIS OF POOR SCHOLASTIC PERFORMANCE AMONG CHILDREN: A REVIEW BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
Kavita Singh, Dinesh Parmar and CBS Dangi
behavior and in the causes of their de ciency. Different
classi cation systems have been proposed in the past
to bring some order in this disarray. Most systems have
approached the problem from one of three viewpoints:
severity of the handicap, etiology of the symptoms, and
the symptom collection.
Additional criteria for classi cation
Persons with mental retardation can also be grouped by
age, an important criterion in education and longitudinal
evaluation. Mainly for purposes of management, mental
retardation can also be subdivided according to the bio-
logical syndrome. This classi cation offers advantages
for special training and schooling in mentally retarded
patients with associated de cits such as blindness, deaf-
ness, and spina bi da, (Halgin and Whiteborne, 2005).
Causes and Consequences
The causes of poor scholastic performance can be
broadly classi ed into two groups that involve genet-
ics and environment. The present study exclusively aims
to focus on genetic causes of PSP however, discussion
on medical and varied environmental factors remains
imperative. There may be genetic basis of various medi-
cal problems associated with PSP, and many problems
are purely environmental in their origin. Poor scholas-
tic performance (PSP) shows multiple etiologies. Many
reasons are responsible for poor scholastic performance
of children involving speci c learning disability, atten-
tion de cit hyperactivity disorder, low IQ level, emo-
tional problems and psychiatric disorders. Other reasons
involve a poor socio-cultural home environment and
additional environmental causes, (Bruno and Njoku,
2012).
The causes of PSP can be further divided into extrin-
sic or environmental and intrinsic or individual factors.
School dif culty (SD) and learning disability (LD) are
two different manifestations of some school attending
children. Former is related to pedagogical dif culties.
Apart from diseases and related disabilities, pedagogical
dif culties can also pose poor scholastic performance.
It is extrinsic in nature with no possibilities of organic
impairment (Siqueira and Gurge-Giannetti, 2011). Envi-
ronmental reasons may infuse lack of interest in stud-
ies and distraction among some children may results in
disappointment, frustration, low self-esteem and failure
(Karande and Kulkarni, 2005).
Emotional causes are also important while consid-
ering poor scholastic performance being secondary to
environmental factors involving lack of inspiration, low
self-esteem and lack of sympathy and unresponsive-
ness (Valiente et al. 2012). It is argued that emotions
in uence school performance of children and that inte-
grating cognition and emotion can demonstrate school
performance and scholastic achievement in early for-
mal education (Blair, 2002; Raver, 2002). Therefore, for
a ourishing learning process, numerous cognitive skills
associated with proper opportunities are essential.
Present work exclusively focuses on genetic causes of
Poor scholastic performance hence; this largely involves
Mental De ciency (MD) which is again a developmen-
tal disability characterized by sub-mental level or lower
than average intelligence of the age of a child. This is
chie y associated with biological causes that may show
developmental delay or/and involvement of genes or
chromosome. The investigation of the genetic basis of
mental de ciency focuses mainly on identi cation of
smaller and smaller chromosome variations associated
with disease, (Raynham et al., 1996; Lucy Raymond and
Tarpey, 2006).
The modest beginning of the investigation of the
genetic basis of mental de ciency started long back in
1938 with a preliminary study of patients con ned to
hospital institutions (Penrose, 1938). In later years focus
was on identi cation of smaller and smaller chromo-
some variations associated with disease (Raynham et al.,
1996; Raymond and Tarpey, 2006 ).
Abnormal development of a child that leads to men-
tal retardation may be due to trauma before birth caused
by an infection or exposure to alcohol, drugs, or other
toxins and trauma during birth caused by deprivation
of oxygen or premature delivery of a new born child.
Inherited disorders involve point mutation(s) and gross
chromosomal abnormalities. Certain point mutations
cause metabolic disorders that lead to mental retarda-
tion phenotype such as phenylketonuria (PKU). On the
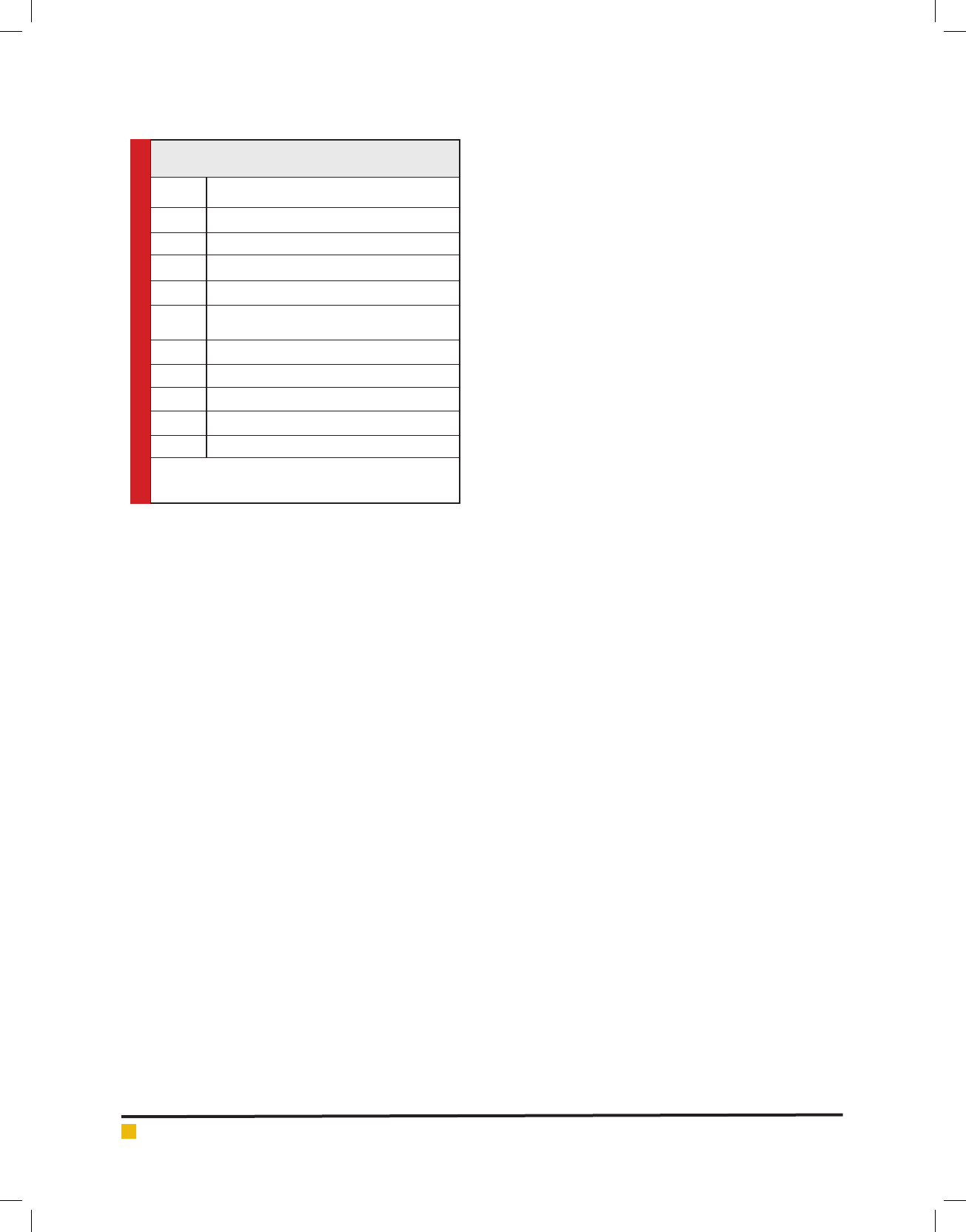
Table 1. showing WHO List of Causal Factors of
Mental Retardation
S. No. Causal factors
1.
Infections and intoxications
2.
Trauma and physical agents
3.
Disorders of metabolism, growth or nutrition
4.
Gross brain damage (postnatal)
5.
Diseases or conditions due to unknown prenatal
in uences
6.
Chromosome abnormalities
7.
Prematurity
8.
Major psychiatric disorder
9.
Psycho-social (environmental) deprivation
10.
Other and unspeci ed
Source: WHO: Mental health: strengthening our response (www.
who.int/news-room/fact-sheets/detail/mental-health-strengthening-
our-response)

BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS GENETIC BASIS OF POOR SCHOLASTIC PERFORMANCE AMONG CHILDREN: A REVIEW 769
Kavita Singh, Dinesh Parmar and CBS Dangi
other hand, chromosomal abnormality such as Down
syndrome demonstrates peculiar morphological and
abnormal behavioral traits. The averageIQof matured
persons with Down syndrome remains 50 that remain
widely variable, (Malt et al. 2013).
Prevalence
Social integration of a moderately mental retardate will
be more dif cult in a competitive, industrialized com-
munity than in a rural environment with the long-term
support of an old fashioned, extended family (Durkin et
al. 1995). Almost all studies dealing with mental sub-
normality in children report a higher incidence in males
than in females. Moreover, in addition to the data col-
lected from population and institution surveys, recent
studies of family pedigrees more speci cally demonstrate
that X-linked recessive disorders represent a substantial
proportion of mentally retarded males (Raymond, 2006).
The prevalence of mental retardation is in uenced by
a great number of environmental factors such as com-
munity, age, racial and ethnic background, geographic
region, and sex (Hernandez and Blazer, 2006).
According to WHO estimates globally more than 450
million people suffer from mental disorders. Currently,
mental and behavioral disorders account for 12% of the
global burden of disease. This is likely to increase to
15% by 2020. The major proportions of mental disor-
ders come from low- and middle-income countries. The
problem is further complicated by a lack of adequate
trained manpower and a low priority of mental health in
health policy (Reddy et al. 2013).The severely retarded
are mostly identi ed before the age of one year, espe-
cially in the presence of physical abnormalities such
as hydrocephaly, spasticity, and sensorial disturbances.
Mildly mentally retarded individuals with IQ’s ranging
between 50 and 70 are recognized at school age (Boat
and Wu, 2015).
In India, mental disorders have a prevalence of
1.05%. Urban population has slightly higher rate being
at 1.1% as compared to rural being at 1.008%. Age was
found to be highly correlated with prevalence among
children of rural areas (Lakhan et al. 2015). Once the
critical period of adolescence and school attendance
is over, however, many of the mildly mentally handi-
capped are assimilated into society and join the ranks
of the dull-normal, living for the most part in marginal
socio economic circumstances.
Genetic Disorders
Genetic disorders are divided into two main groups.
The rst group includes chromosome disorders, such as
Down syndrome, which may involve an entire chromo-
some including thousands of genes, while the second
group involves only a single gene. Single gene disorders
are divided into three main categories based on the mode
of inheritance of the abnormal gene. The categories are
autosomal recessive, autosomal dominant, and X-linked
(Thompson and Thompson, 1986; Pradhan et al., 2011).
Involvement of Chromosomes in Mental Disability
There are genetic components to mental disability.
Examination of persons with chromosomal variations
and mental disabilities may be a way of overcoming
dif culties faced with the proper diagnostic processes.
Unfortunately, chromosomal analysis is rarely under-
taken in subjects with psychiatric disorders. However,
the rate of chromosomal abnormality has signi cantly
increased in persons with learning disability, and may
be as high as 20% in those with mild learning dis-
ability (Gostason et al. 1991).It has been established
in many other medical conditions with a genetic basis
that chromosomal variations, either by direct gene dis-
order or by positional effects, can produce identical or
similar phenotypes to those caused by point mutations
and their existence has greatly facilitated the physi-
cal mapping and cloning of candidate genes (Collins,
1992, 1995).
Once a chromosomal anomaly is detected in a sub-
ject with mental disability, it may be considered non-
coincidental and related to the disorder if one or more
of the following criteria are met: (a) the chromosomal
abnormality is rare and there are independent reports of
the abnormality being associated with mental disability;
(b) there is proximity of the abnormality with a region
of suggestive linkage ndings; or (c) there is co-segre-
gation of the abnormality with mental disability within
the patient’s family, (Evans et al. 2001).
Some variations in chromosomes are very small and
they only involve a single gene called single gene dis-
orders. However, when variations in chromosomes are
large enough and can be seen under light microscope,
they are called chromosome anomalies or aberrations.
There are many types of chromosome anomalies. Chro-
mosome anomalies usually occur when there is an error
incell divisionfollowingmeiosisormitosis. They can be
organized into two basic groups viz. Numerical anom-
alies (aneuploidy or an abnormal number of chromo-
somes) and Structural anomalies. Numerical anomalies
occur due to nondisjunction where abnormal numbers
of chromosomes may nd their way into gametes, and
a disorder of chromosome numbers may result. Altera-
tion in chromosome structure can take several forms
described as under:
• Deletions: A portion of the chromosome is missing
or deleted.
• Duplications: A portion of the chromosome is
duplicated

770 GENETIC BASIS OF POOR SCHOLASTIC PERFORMANCE AMONG CHILDREN: A REVIEW BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
Kavita Singh, Dinesh Parmar and CBS Dangi
• Translocations: A portion of one chromosome is
transferred to another chromosome. There are two
main types of translocations:
Reciprocal translocation: Segments from two dif-
ferent chromosomes have been exchanged.
Robertsonian translocation: An entire chromo-
some has attached to another at the centromere
• Inversions: A portion of the chromosome has
broken off, turned upside down, and reattached,
therefore the genetic material is inverted.
There are two main types of Inversions:
Paracentric inversions: Both breaks occur in
one arm of the chromosome and do not include
thecentromere
Pericentric inversions: Breaks occur in each arm
of the chromosome and involved the centromere
• Insertions: A portion of one chromosome has been
deleted from its normal place and inserted into
another chromosome.
• Rings: A portion of a chromosome has broken off
and formed a circle or ring. This can happen with
or without loss of genetic material.
• Isochromosome: Formed by the mirror image copy
of a chromosome segment including the cen-
tromere.
The chromosomes observed at metaphase stage pos-
sess two chromatids called sister chromatids. Chroma-
tids of two different chromosomes are called non-sister
chromatids. Conventionally, all the chromosomal aber-
rations are broadly divided into two groups.
Chromosome-type: In this type, breaks and re-joins
always involvebothsister-chromatids at any one locus.
Chromatid-type: In this type, breaks and re-joins
always involveonlyoneof the sister-chromatids at any
one locus.
Common Chromosomal Anomalies in Mental De ciency
Down syndrome
Down syndrome is unique in its prominent role in
exploring biology of mental retardation for the rst
time in 1866 by John Longdon Down whose contribu-
tion was signi cant in understanding biology of normal
and abnormal development (Down, 1866). The discovery
of an extra 21 chromosome (trisomy 21) in the cells of
individuals with Down syndrome exhibiting 47 chro-
mosomes in place of 46 normal numbers by Professor
Lejeune in 1959 established role of chromosome varia-
tions in development.
This was the discovery of chromosome aneuploidy in
man that rmly established study of chromosome called
cytogenetic as bona de medical discipline (Smith and
Warren, 1985; Patterson, 2009). Karyotype of normal
human exhibits that chromosome 21 is one of the small-
est autosomes, comprising nearly 1.9% of human DNA,
Non-disjunction of this autosome during formation of
the gametes at meiosis I or meiosis II in one of the par-
ents result in Down syndrome. Down syndrome is the
most common genetic form of mental retardation fol-
lowed by X-linkedmental retardation.
Fragile X syndrome
Fragile sites are heritable points on a chromosome which
are susceptible to breakage and are consistently found on
certain human chromosomes (Sutherland, 1982a, 1982b).
These sites may represent structural chromosome muta-
tions. Fragile X syndrome (FXS) causes learning disabil-
ities and cognitive impairment. Usually, the penetrance
of this genetic condition is higher in males as compared
to females because males are hemizygous having sin-
gle X-chromosome (McKusick, 1983). The maximum
numbers of single genes that cause mental retardation
are located on X chromosome. The rst identi ed gene
was FMR1 that causes fragile X syndrome being the
commonest single gene abnormality. The fragile site on
the long arm of the X (Xq 27.3) is associated with a form
of familial X-linked mental retardation (Lubs, 1969). It
has been estimated that from one third to one half of all
families with (nonspeci c) X-linked mental retardation
express the fragile site in some proportion of their cells
(Brookwell et al, 1982).
The fragile site can be detected in chromosome prepa-
rations from lymphocytes grown in tissue culture media
lacking folic acid and thymidine. Speci c culture condi-
tions can signi cantly alter the frequency with which
the fragile site is expressed. Female carriers of this disor-
der may or may not express the fragile Xj some express
it in only a small number of their cells. Thus, Xq fragile
site demonstration in such carriers and in some affected
males may be dif cult due to a low level of expression.
As with most X-linked recessive disorders, carrier detec-
tion is an important: aspect of genetic counseling for
families with this syndrome.
Males with fragile X syndrome show mild to moder-
ate intellectual disability whereas considerable propor-
tions of females with this disorder being nearly one-third
remain intellectually disabled. Majority of males and
nearly half the females withfragile X syndromeshow
characteristic morphological features involving long
and narrowface, prominent jaw and forehead, atfeet,
large ears and in males additionally enlarged testicles
after puberty. A mutation of FMR-1 known as fragile-X
mental retardation gene located on the X- chromosome
causes this syndromic condition. The FMR1 gene codes
a protein known as fragile X mental retardation protein
(FMRP) required for normal brain development. Inci-
dence was noted in all races and ethnic groups. Nearly

BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS GENETIC BASIS OF POOR SCHOLASTIC PERFORMANCE AMONG CHILDREN: A REVIEW 771
Kavita Singh, Dinesh Parmar and CBS Dangi
10% affected males have severe intellectual disability
(Hagerman and Hagerman, 2002).
In fragile X syndrome, CGG pattern in a part of DNA
in FMR1 gene is repeated many times. In majority of
persons, the number of repeats remains small at 5 to 44
repeats, which is common whereas; when the number of
repeats is very high being greater than 200 repeats, the
gene turns off and protein production is halted leading
to development of FXS which is also known as trinucle-
otide repeat disorder. This is heritable condition trans-
mitted from parents. Intermediate number of repeats at
nearly 45 to 54 may have somewhat higher probability
of having some symptoms but they do not have fragile
X syndrome (Willemsen et al. 2011).
Sequence repeats in the range of 55-200 do not
develop FXS but there may be development of other
condition known as fragile X-associated disorder. Cou-
ple with premutation can transmit this to their children
with the same condition or full mutation leading to
development of FXS (Gallagher andHallahan, 2012).
The global prevalence of fragile X syndrome (FXS) in
males is estimated nearly 1 in 4,000 while in females it
is nearly 1 in 5,000. It has been demonstrated in both
animal and human studies that changes in the environ-
ment radically impact behavior, (Restivo et al. 2005).
A peaceful high quality home environment has been
found associated with fewer autistic behaviors, higher
IQ scores and better adaptability in children with Fragile
X syndrome (Glaser et al. 2003).
The magnitude of genetic variations in mental de -
ciency and scholastic performance of children suggests
strong genetic component. Genetic effects that in uence
general and verbal cognitive ability are largely respon-
sible for scholastic performance. Remedial intervention
remains a more immediately attainable goal while Sub-
sequent research will entail more genetic analyses lead-
ing to identi cation of genes that in uence academic
achievement.
REFERENCES
APA (2000): Diagnostic and statistical manual of mental disor-
ders, 4th ed. Washington, DC: American Psychiatric Associa-
tion, USA.
Blair, C. (2002): School readiness. Integrating cognition and
emotion in a neurobiological conceptualization of children’s
functioning at school entry. Am Psychol. 57(2):111-27
Boat, T.F. and Wu, J.T. editors (2015): Mental Disorders and
Disabilities Among Low-Income Children. Washington (DC):
National Academies Press (US);
Brookwell, R: Daniel, A; Turner, G; Fishburn, J. (1982): The
fragile X(q27) form of X-linked mental retardation: FudR as
an inducing agent for fraX(q27) expression in lymphocytes,
broblasts and amniocytes. Am J Med Genet, 13: 139-148.
Bruno, U.D.O. and Njoku, J. (2012): Classroom Management
of Mental Retardation. International Journal of Learning &
Development, 2(5): 105-111.
Carlson, M. J. and Corcoran, M. E. (2001): Family structure and
children’s behavioral and cognitive outcomes. Journal of Mar-
riage and Family, 63:779-792.
Davies, G; Marioni, R E; Liewald, D C; Hill, W D; Hagenaars, S
P; Harris, S E. et al. (2016): Genome-wide association study of
cognitive functions and educational attainment in UK Biobank
(N=112 151). Molecular Psychiatry,21: 758–767.
Deary, I. J, Spinath F.M; Bates T.C. (2006): Genetics of intel-
ligence. European Journal of Human Genetics, 14, 690–
700.
Deary, I.J.Intelligence.Annu. Rev. Psychol.63, 453–482 (2012)
Doll, Edgar A The Measurement of Social Competence: A Man-
ual for the Vineland Social Maturity Scale1953MinneapolisEd-
ucational Test Bureau (720 Washington Avenue, S. E.)641
Down, J. L. H. (1866): Observations on an Ethnic Classi cation
of Idiots. London Hospital Reports, 3:259-262,
Durkin, M.S; Wang, W; Shrout, P.E; Zaman, S.S; Hasan, Z.M;
Desai P, et al. (1995): Evaluating a ten question screen for
childhood disability
Evans K.L; Muir, W.J; Blackwood, D.H; Porteous, D.J. ( 2001):
Nuts and bolts of psychiatric genetics: building on the Human
Genome Project. Trends 92 Genet; 17: 35–40
Gallagher, A, and Hallahan B. (2012): Fragile X-associated dis-
orders: a clinical overview. J Neurol. , 259(3):401-413.
GlaserB, Hessl D, Dyer-Friedman J, et al. Biological and envi-
ronmental contributions to adaptive behavior in FXS. Am J
Med Genet A. 2003;117A (1):2–29.
Gostason, R; Wahlstrom, ;Johannisson, T; Holmqvist, D. (1991):
Chromosomal aberrations in the mildly mentally retarded. J
Men De c Res; 35: 246- 246.
Greene, B. A; Miller, R. B; Crowson, H. M; Duke, B. L; Akey, K.
L. (2004): Predicting high school students’ cognitive engage-
ment and achievement: Contributions of classroom percep-
tions and motivation. Contemporary Educational Psychology,
29, 462 – 482.
Hagerman, R.J. and Hagerman, P.J., editors. (2002): FXS: diag-
nosis, treatment, and research. Baltimore (MD): Johns Hopkins
University Press.
Halgin, R. and Whiteborne, K. (2005). Abnormal Psychology.
New York: McGraw Hill.
Hernandez, L.M; Blazer, D.G; editors.(2006):Genes, Behavior,
and the Social Environment: Moving Beyond the Nature/Nur-
ture Debate. Washington (DC): National Academies Press (US).
Karande S, Kulkarni M. (2005): Poor school performance.
Indian J Pediatr. ,72:961-7.
Lakhan, R; Ekúndayò, O. T; Shahbazi, M. (2015). An estimation
of the prevalence of intellectual disabilities and its association
with age in rural and urban populations in India. Journal of
Neurosciences in Rural Practice, 6(4), 523–528

772 GENETIC BASIS OF POOR SCHOLASTIC PERFORMANCE AMONG CHILDREN: A REVIEW BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
Kavita Singh, Dinesh Parmar and CBS Dangi
Landry, S.H. (2014): The role of parents in early childhood
learning. Encyclopedia on Early Childhood Development, USA.
Lubs, H. A. (1969): A marker X chromosome. Am. J. Hum.
Genet, 21: 231-244.
Luckasson, R., Coulter, D. L., Polloway, E. A., Reiss, S., Schalock,
R. L., Snell, 98 M. E., Spitalnick, D. M., & Stark, J. A. (1992):
Mental retardation: De nition, classi cation, and systems of
supports (9th Edition). Washington, DC: American Association
on Mental Retardation
Lucy Raymond, F. and Tarpey, P.(2006): The genetics of mental
retardation. Human Molecular Genetics, 15(l): 110-116.
Malt, EA; Dahl, RC; Haugsand, TM; Ulvestad, IH; Emilsen, NM;
Hansen, B; Cardenas, YE; Skøld, RO; Thorsen, AT; Davidsen,
EM (2013): Health and disease in adults with Down syndrome.
TidsskrNorLegeforennr. 133 (3): 290–294.
McKusick, V.A. (1983): Human Genetics. 3rd Edition, Prentice-
Hall foundations of modern genetics series.
Okoye, N. N. (1982). Why students fail examinations: Psychol-
ogy for everyday living; A Nigeria Journal of Applied Psychol-
ogy 11(2): 1 – 5.
Patterson D (2009): Molecular genetic analysis of Down syn-
drome. Hum Genet. 126(1):195-214.
Penrose, L. S. (Lionel Sharples) (1938): A clinical and genetic study
of 1280 cases of mental defect. H. M. Stationery off, London.
Pradhan, S; Sengupta, M; Dutta, A; Bhattacharyya, K; Bag,
S.K; Dutta, C; Ray, K. (2011): Indian genetic disease data-
base,Nucleic Acids Research, 39(suppl_1):933–938.
Raver, C.C. (2002); Emotions matter: Making the case for the
role of young children’s emotional development for early
school readiness. Social Policy Report, Society for Research in
Child Development. 16:3–18.
Raymond, F. L. (2006). X linked mental retardation: a clinical
guide. Journal of Medical Genetics, 43(3), 193–200.
Raynham, H;Gibbons, R;Flint, J;Higgs, D. (1996): The genetic
basis for mental retardation, 89(3):169-175.
Reddy, V.B; Gupta, A; Lohiya, A, Kharya, P..(2013): Mental
health issues and challenges in India. IJSER, 3:1-3.
Reschly, D.J; Myers, T.G; Hartel, C.R. Editors (2002): Mental
Retardation: Determining Eligibility for Social Security Ben-
e ts, National Research Council (US) Committee on Disability
Determination for Mental
Restivo L, Ferrari F, Passino E ( 2005): Enriched environment
promotes behavioral and morphological recovery in a mouse
model for the FXS. Proc Natl AcadSci U S A.;102 (32):115-57 .
SiqueiraI, C. M. and Gurge-Giannetti, J. (2011). Poor school
performance: an updated review. Revista da Associação Médica
Brasileira, 5(1): 78-8
Sniekers, S; Stringer, S; Watanabe, K; Jansen, P.R; Coleman,
J.R.I; Krapohl, E. et al. (2017): Genome-wide association meta-
analysis of 78,308 individuals identi es new loci and genes
in uencing human intelligence. Nature Genetics, 49:1107–
1112.
Suess, J.F; cotton, P.D; Sison, G.F. Jr (1983): The American
Association on Mental De ciency--adaptive behavior scale:
allowing credit for alternative means of communication. Am
Ann Deaf, 128(3):390-393.
Sutherland. G. R. (1982b): Heritable fragile sites on human
chromosomes, IX.Population cytogenetic and segregation
analysis of the BrdU-requiring fragile site at 10q25. Am. J.
Hum. Genet, 34: 753-756.
Terman, L. M. and Merrill, M. A. (1937): Measuring Intel-
ligence: A Guide to the Administration of the New Revised
Stanford-Binet Tests of Intelligence. Boston Houghton Mif in
Co461
.
Thompson, J.S. and Thompson, M.W. (1986): Genetics in Medi-
cine. W.B Saunders Co., Philadelphia, Pennsylvania.
Tredgold, A. F., and Soddy, K. 1956. A textbook of mental
de ciency. 9th ed. Baltimore: Williams & Wilkins
Valiente, C., Swanson, J., & Eisenberg, N. (2012). Linking Stu-
dents’ Emotions and Academic Achievement: When and Why
Emotions Matter. Child Development Perspectives, 6(2), 129–
135.
Willemsen, R., Levenga, J., and Oostra, B. A. (2011): CGG
repeat in the FMR1gene: size matters. Clinical Genetics, 80(3),
214–225