
Ergonomic effects on workers of selected healthcare
areas of King Abdulaziz Medical City, National Guard
Hospital, Riyadh Saudi Arabia
Fayz Al Shahry,
1
Wejdan Mohammed Alhuwail
2
, Ghadah Mohammed Alshehri
2
, Jihan Ali
Al-Motairi
2
, Smily Jesupriya Victor Paulraj
3
*, Fatma Othman
4
and Galib Algamdi
5
1
Assistant Professor. CAMS, KSAU-HS, Consultant Neurorehabilitation Service, King Abdulaziz Medical City,
2
Student, Occupational Therapy, CAMS, KSAU-HS, Riyadh Saudi Arabia
3
Senior lecturer, CAMS, KSAU-HS, Riyadh Saudi Arabia
4
Assistant Professor CAMS, KSAU-HS, Riyadh Saudi Arabia
5
Occupational Therapy Program Manager CAMS, KSAU-HS, Riyadh Saudi Arabia
ABSTRACT
Ergonomics’ is composed of two words which are ‘ergo’ a Greek word meaning work, and ‘nomics’ which means
study. Ergonomics factors that contribute to the health are inappropriate lighting, tools design, chair design, heavy
lifting and repetitive motion and others. These factors can cause musculoskeletal disorders (MSDs). The aim of this
study was to assess ergonomic effect on workers of ultrasound and microbiology areas in King Abdulaziz Medical
City, (KAMC)-Riyadh. The second objective of this study was to identify the ergonomic factors and the presence of
work related injuries, also to compare awareness of ergonomics of work sites of health workers. This study was a cross
sectional quantitative study conducted at KAMC,National Guard Hospital (NGH), the sample size for workers in radi-
ology department was 27, and the sample size for workers in the laboratory was 27. Two questionnaires distributed
among laboratory and radiology workers constructed of questions and demographic data were adapted for our study
to determine the effect of ergonomics, the most common physical problems that workers experience in their worksta-
tion, and the awareness of ergonomic among the health care workers 18 participants (40.0% of the total) from the
Microbiology-technicians were completed the questionnaire and were 27 participants (60.0%) form the Ultrasound-
sonographers completed the questionnaire. There was an ergonomic effect on gender for microbiology technicians
(p-value was 0.043). Moreover, the ultrasound-sonographers had a signi cant association between gender and pain
595
Medical
Communication
Biosci. Biotech. Res. Comm. 11(4): 595-602 (2018)
ARTICLE INFORMATION:
Corresponding Authors: shahryf@hotmail.com
Received 1
st
Aug, 2018
Accepted after revision 23
rd
Nov, 2018
BBRC Print ISSN: 0974-6455
Online ISSN: 2321-4007 CODEN: USA BBRCBA
Thomson Reuters ISI ESC / Clarivate Analytics USA
Mono of Clarivate Analytics and Crossref Indexed
Journal Mono of CR
NAAS Journal Score 2018: 4.31 SJIF 2017: 4.196
© A Society of Science and Nature Publication, Bhopal India
2018. All rights reserved.
Online Contents Available at:
http//www.bbrc.in/
DOI: 10.21786/bbrc/11.4/9
Fayz Al Shahry et al.
596 ERGONOMIC EFFECTS ON WORKERS OF SELECTED HEALTHCARE AREAS BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
related to work (p value < 0.001). Awareness however, in microbiology technicians, was found to be 83% who knew
the meaning of ergonomics and 85% in ultrasound sonographers. In conclusion, there was a signi cant effect of
ergonomic on sonographers and microbiology technician. The study showed a good level of knowledge and aware-
ness about ergonomics, however, still there is a quiet high percentage of them who did not receive health education
on ergonomics and also a high percentage who aren’t implementing ergonomics. There is a need for educational and
implementation empowerment programs in this regard.
KEY WORDS: ERGONOMIC, ULTRASOUND, MICROBIOLOGY, OCCUPATIONAL THERAPY, MUSCULOSKELETAL DISORDERS
INTRODUCTION
‘Ergonomics’ is composed of two words which are ‘ergo’
a Greek word meaning work, and ‘nomics’ which means
study, Tayya et al. (1997) Pao et al. (2001) have de ned
ergonomics as a branch of science which analyses the
optimal relationship between workers and their environ-
ment. It is also described as a system that the work-
ers interact with the work environment, the tasks and
the workplace, (Brooks 1998). Ergonomics signi cantly
developed during World War II, and now includes design,
medicine, and computer science, (Goyal et al., 2009) as it
includes a variety of conditions that can affect workers
in different aspects such as health and comfort. Besides,
it also has factors that are contributing to the health
such as lighting, tools design, chair design, heavy lift-
ing and repetitive motion and others. These factors can
cause injuries and problems related to muscles, tendons
or nerves which can lead to musculoskeletal disorders
(MSDs), (Jaffar et al., 2011, Mcatamney et al., 2017).
Musculoskeletal disorders MSDs are injuries and dis-
orders that affect the nerves and soft tissues which are
muscles, tendons, ligaments and joints. According to Yelin
et al. (1999) the majority of the old workers were disabled
due to MSDs, which were also observed among female
care givers. Therefore, poor ergonomics have an impact
on the worker’s health and can lead to occupational health
injuries. According to Lee, ergonomics is promoting com-
patibility between humans and systems, (Lee 2017).
Considering the workers’ limitations and capabilities
by tting environments, and tasks to improve the pro-
ductivity and safe work performance reduce costs due
to work injuries. There are many types of jobs which
require moderate to heavy physical work such as health
care workers, engineers, food industry workers, manual
workers, and of ce workers and other service staff.
Inappropriate workplace design, tools and equipment
machine lead to fatigue, frustrate, and hurt the workers.
The most extreme risk factors which affect the workers
on the worksite are the uncomfortable static position,
repetitive motion, vibration, heavy lifting, temperature,
and lighting. Many studies have shown that work inju-
ries and pain caused by risk factors of ergonomics result
from frequent bending, twisting, heavy physical activi-
ties, heavy (manual) lifting and whole-body vibration,
(Estryn-Behar et al. 1990, Kuiper et al. 1999 and Lee
2017).
One of the most arduous professionals that require over-
load on the body, forced position, and long working hours
are working in health care. Doctors, Nurses, Radiologists,
Dentists and other groups in the healthcare professions
show a high incidence of work-related injuries and pain
result from a singular (acute) event to gradual events of
repetitive movement which lead to handling patients and
equipment. Several studies are showing high-risk factors
of ergonomics among healthcare workers. The primary
factors which can increase musculoskeletal injuries and
induce pain among health care workers are load (weight
and size of materials, the force needed to push or pull, a
position of handholds, and a shape of handles) and posture
(disadvantageous positions of the arms and legs, forward
bend and twist of the trunk) and environment (inappro-
priate oor conditions, insuf cient equipment, inadequate
lighting and thermal conditions, and time pressure). Ergo-
nomics have a high impact on the worker, and poor ergo-
nomics may lead to MSDs. The job of health care workers
and other professionals demand a tremendous physical
load to improve the productivity of healthcare and hence
adequate quality; the ergonomics prevents the risk fac-
tors and work-related injuries. Proper of ce ergonomics
contribute to increase workers’ effectiveness and reduce
musculoskeletal injuries that associated with of ce work-
ing. Recent studies pointed out that poor ergonomics of
the above areas lead to MSDs and pain on the workers.
Work in radiology area demands physical tasks such
as patient’s transfer and using imaging equipment and
computer-related task. Accordingly, improved ergonom-
ics of the radiology department will contribute to reduce
the risk of work-related injuries and provide the safety
when dealing with patients, (Siegal et al. 2010, Ruess
et al. 2003). In regards to laboratory work, it needs a
prolonged standing position. Because of that laboratory
healthcare workers are more exposed to MSDs and poor
ergonomics can lead to pain in the different area of the
body, (Agrawal et al. 2015).
There is a paucity of data on the ergonomics of places
involving patient care, sites of diagnosis of diseases such
as radiology and laboratories. Hence the present study
was planned and proposed so that the evidence created
from the study will give light to the ergonomic effects
Fayz Al Shahry et al.
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS ERGONOMIC EFFECTS ON WORKERS OF SELECTED HEALTHCARE AREAS 597
Table 1. Participant characteristics
Male Female
Microbiology-technicians (N) 4 14
Percentage (%) 22.2 77.8
Years of experience (mean) 2.67
Ultrasound-sonographers ( N) 4 23
Percentage (%) 14.8 85.2
Years of experience (mean) 10.22
on workers of selected healthcare areas. This study was
aimed to assess the ergonomic effect on workers of ultra-
sound and microbiology technicians of areas in KAMC-
Riyadh, and to identify the ergonomic factors and the
presence of work-related injuries, it also compared the
ergonomical awareness of the workers.
MATERIAL AND METHODS
This was a cross-sectional quantitative study conducted at
National Guard Hospital (NGH), in Riyadh over 6-months
period from Aug to Nov 2017. The study was approved
by the Institutional Review Board at King Abdullah Inter-
national Medical Research Center (KAIMRC). The study
included technicians from two different areas. The rst
area is radiology; the inclusion criteria of radiologist
workers were a technician working at Ultrasound areas
(which include sonographers works in general Ultra-
sound, Mammogram areas, Echo areas, and OB-GYN
areas), including all ages and both genders. The exclusion
criteria were the other areas such as Magnetic Resonance
Imaging (MRI) and Computed Tomography (CT). The other
area is a laboratory, the inclusion criteria were microbiol-
ogy technician, including all ages and both gender. The
exclusion criteria were workers in other areas of labora-
tory such as hematology. With a population of 60 techni-
cians, 50% margin of error of 95% of con dence level,
the required sample size was calculated as 53. Selection
of samples based on the departments. The sample size for
workers in the radiology department is 18, and the sample
size for workers in the laboratory is 27.
A self-developed questionnaire was used to collect the
data from the workers. The questionnaires constructed of
yes or no questions (microbiology department 37 ques-
tions and radiography department 30 questions) and
demographic data was adapted for our study to determine
the most common physical problems that workers experi-
ence in their workstation, the effect of ergonomics, and
the awareness of ergonomic among the healthcare work-
ers. The procedure of the study done after identi cation of
the subjects and the consent form was obtained from the
participants before enrolling in the study. The question-
naires were distributed randomly among laboratory and
radiology workers. All the data collected were analyzed
by SPSS version 21 software, and descriptive statistics
were used to summarize the data.
RESULTS AND DISCUSSION
STUDY POPULATION
We identi ed 45 microbiology-technicians and Ultra-
sound-sonographers. The Microbiology-technicians
were 18 participants (40.0%) completed the question-
naire, with a mean age of 26 years (SD = 3.97). The
Ultrasound-sonographers were 27 participants (60.0%)
completed the questionnaire, with a mean age of 35
years (SD = 7.17) (see Table 1 for further information).
Ergonomic Effects on Health Care Workers
Ergonomic Effects on Microbiology-technicians
A signi cant association between gender and pain
related to work (p-value was 0.043). We found that 50%
of male and 92% of female have pain or discomfort
related to work. We reveals that the most common pain
positions among both genders were lower back (16%),
followed by Feet heel (14%), Neck and shoulder blade
(12%), Shoulders and headache (10%), dry eyes (9%),
eye strain (7%), depression and wrist (5%). We found
that (60%) of both genders reported that the pain started
at the end time of the workday (p-value was 0.017).
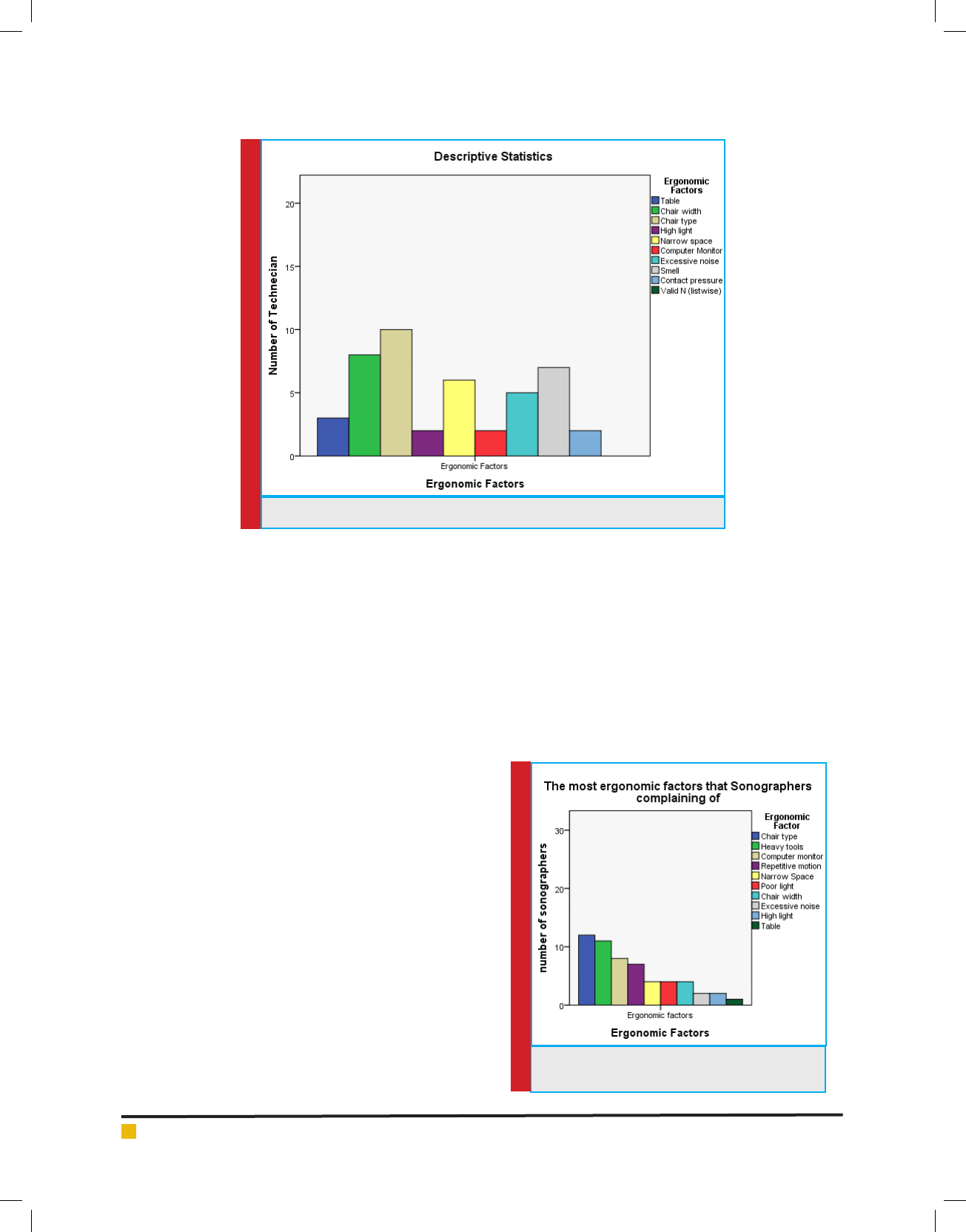
Table 2 & gure 1 shows that most common activities
of daily living that affected by work-related pain were
social activities and sleep (33%), family demands (27%),
work productivity and health maintenance (16%). The
results show that, the most common factor the partici-
pants were complaining of was chair type (55%), fol-
lowed by chair width (44%), smell (38%), narrow space
(33%), excessive noise (27%), table (16%), high light and
computer monitor and contact pressure (11%). Regard-
ing the techniques and changes that technician used to
decrease the pain related to work, we found that most
of them applying stretching exercise (50%), massage
(44%), and the rest either take painkillers, smoking or
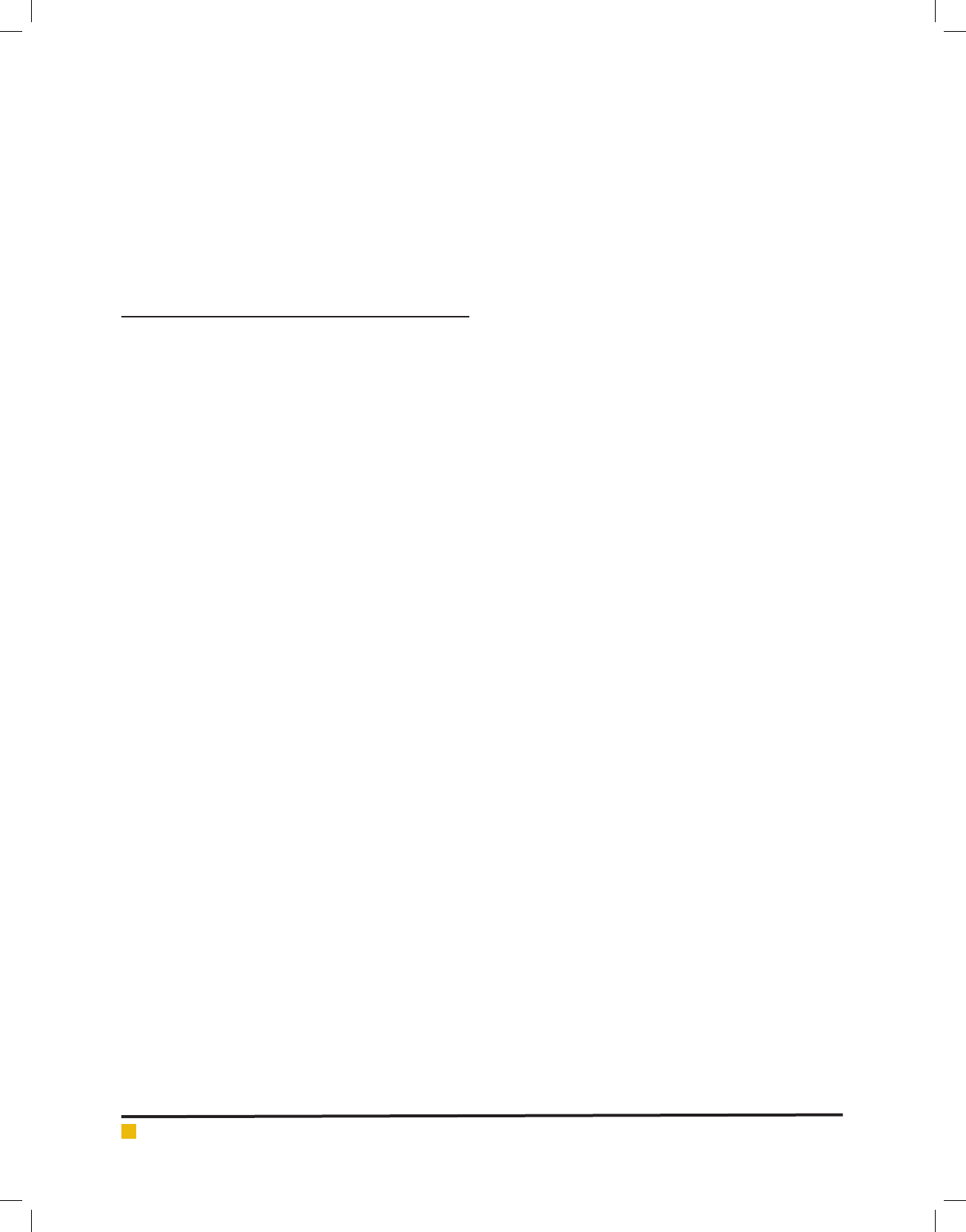
Table 2. Activities that affected by work injuries on
microbiology technicians
n Total Pearson
Chi-Square
p-value
Social activity 6 18 .643ª 0.432
Sleep 6 18 .643ª 0.423
Family demands 5 18 .020ª 0.888
Work productivity 3 18 .257ª 0.612
Health maintenance 3 18 4.114ª 0.043
Fayz Al Shahry et al.
598 ERGONOMIC EFFECTS ON WORKERS OF SELECTED HEALTHCARE AREAS BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
FIGURE 1. The most ergonomic factors that microbiology complaining
nothing. None of them try to visit Occupational therapy
clinics to get help and education about some techniques
and changes that help to decrease and eliminate pain
and injuries related to work. As a solution to reduce and
eliminate pain related to work, we found that most of
technician suggest to add regular short breaks (50%),
decrease the work hours (33%), increase the number of
technicians (33%), add regular stretching exercise (33%),
made changes in the workplace (22%), and training and
education about proper ergonomics (22%).
Ergonomic Effects on Ultrasound-sonographers.
A signi cant association between gender and pain
related to work (p-value < 0.001). We found that 75% of
the male and 86% of the female have pain or discom-
fort related to work. Fig 2 reveals that the most com-
mon pain positions among both genders were shoulders
(17%), followed by upper back (12%), Neck (11%), shoul-
der blade and lower back (10%), foot heel and dry eyes
(8%), ngers (7%), wrist (6%), and elbow-forearm (5%).
We found that (77%) of both genders reported that the
pain started at the end time of the workday. Table 3
shows that most common activities of daily living that
affected by work-related pain were family demands
(48%), work productivity (40%), social activities (37%),
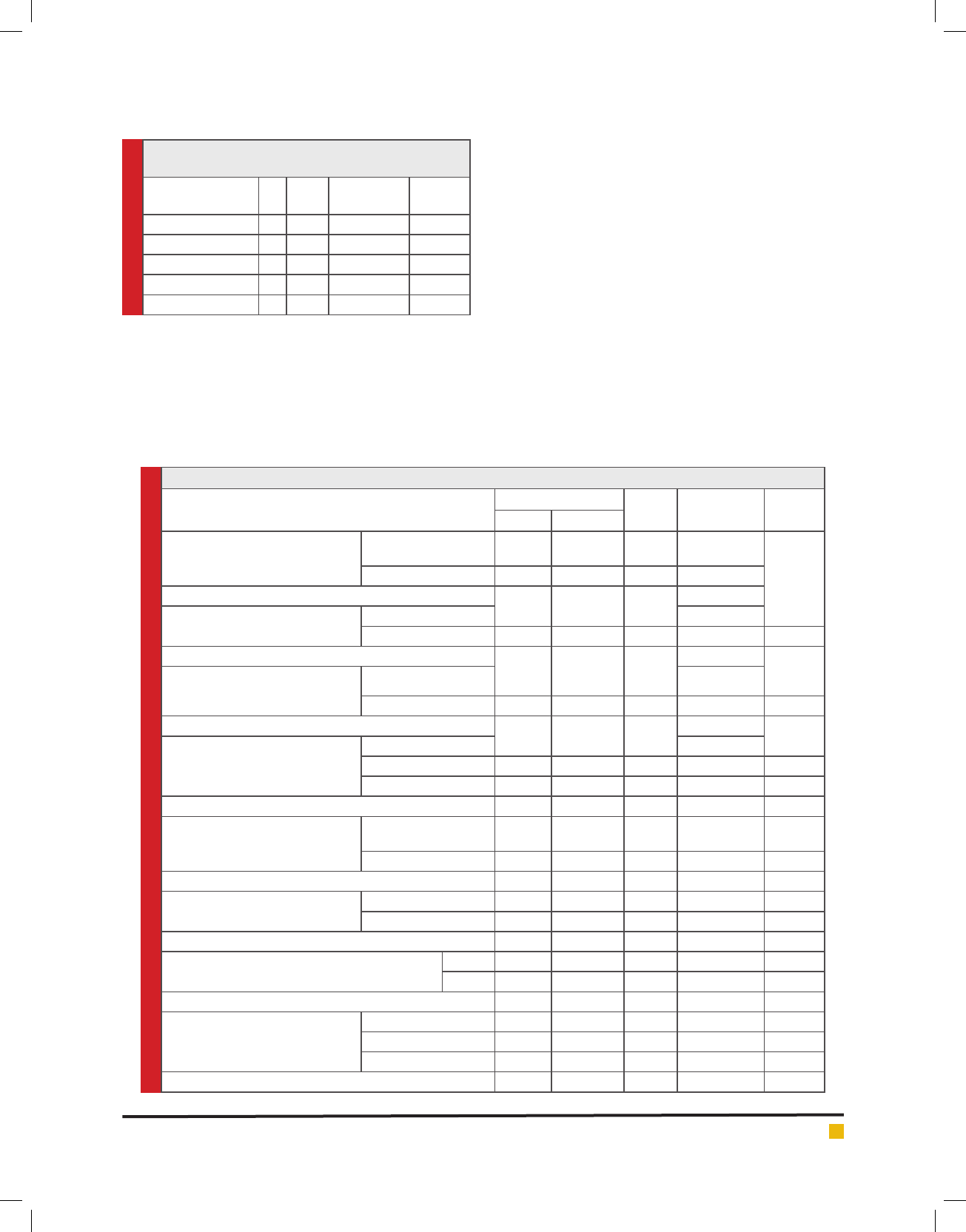
sleep (33%), and health maintenance (18%). The results
show that, the most common factor the participants were
complaining of was chair type (44%), followed by heavy
tools (40%), computer monitor (29%), repetitive motion
(25%), narrow space and poor light and chair width
(14%), excessive noise and high light (7%), and table
(3%) (Figure 2). Regarding the techniques and changes
that sonographers used to decrease the pain related to
work, we found that most of them doing massage (62%),
stretching exercise (55%), ask for sick leave and go to
physician (14%), and go to physiotherapy clinics (7%).
None of them try to visit Occupational therapy clinics
to get help and education about some techniques and
changes that help to decrease and eliminate pain and
injuries related to work. As a solution to minimize and
eliminate pain related to work, we found that most of
technicians suggest having training and education
FIGURE 2. The most ergonomic factors that
sonographers complaining
Fayz Al Shahry et al.
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS ERGONOMIC EFFECTS ON WORKERS OF SELECTED HEALTHCARE AREAS 599
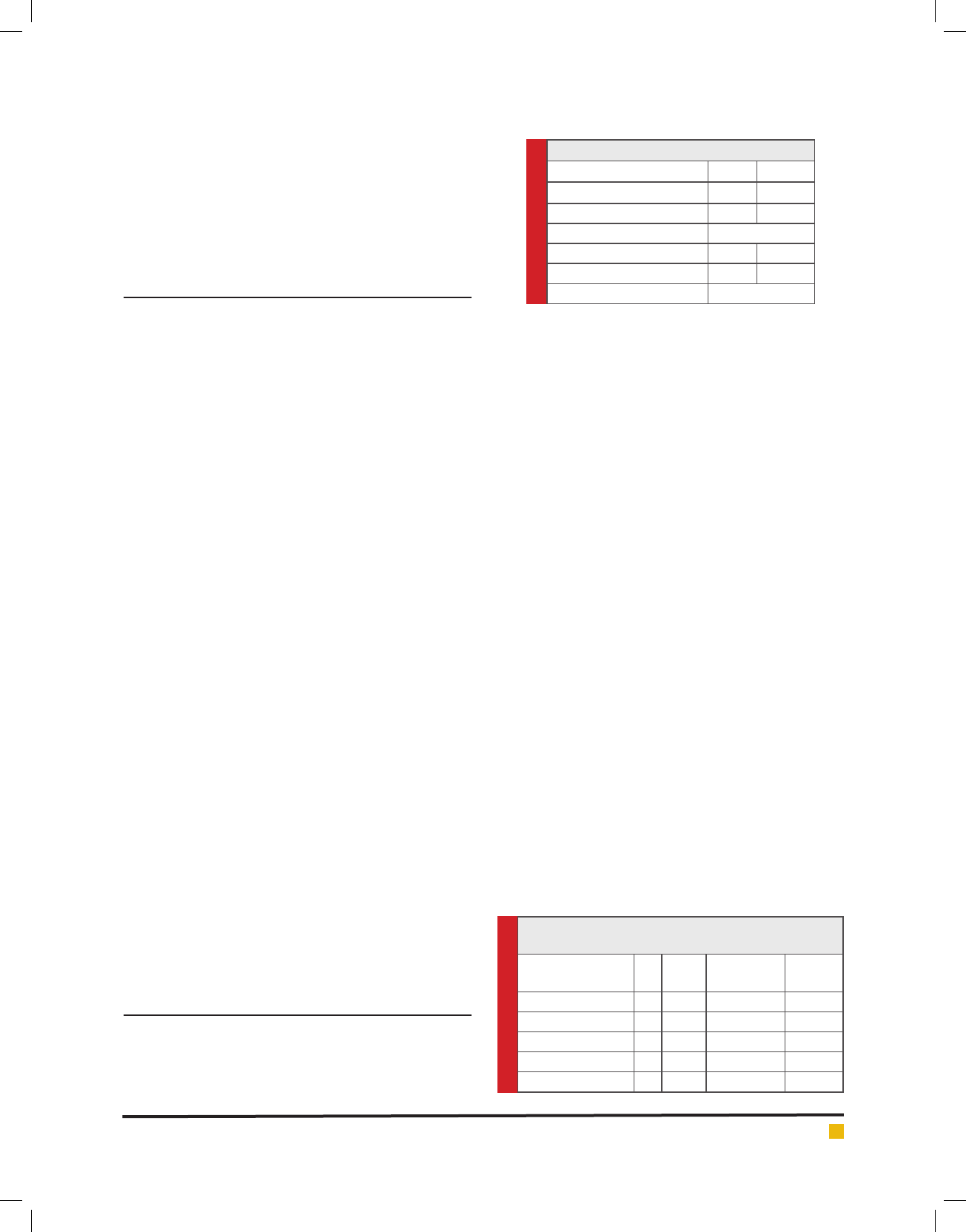
Table 3. Activities that affected by work injuries on
sonographers
N Total Pearson
Chi-Square
p-value
Family demands 13 27 .006ª 0.088
Work productivity 11 27 .167ª 0.683
Social Activities 10 27 2.902ª 0.936
Sleep 9 27 .147ª 0.720
Health maintenance 5 27 1.067ª 0.302
Table 4. Awareness of Ergonomics
Gender Total Pearson Chi-
Square
p-value
Male Female
Microbiology-technicians
Know the meaning of ergonomics No 1 2 3 .257ª .612
Yes 3 12 15
Total 4
1
14
1
18
2
Poor ergonomics lead to health risk No
Yes 3 13 16 1.004ª .316
Total 4
1
14
8
18
9
Educated about proper posture No
Yes 3 6 9 1.286ª .257
Total 4
2
14
5
18
7
Implement proper body mechanics No
Yes 1 7 8
not applicable 1 2 3 .815ª .665
Total 4 14 18
Ultrasound-sonographers
Know the meaning of ergonomics No 1 3 4
Yes 3 20 23 .386ª .534
Total 4 23 27
Poor ergonomic lead to health risk No 1 4 5
Yes 3 19 22 .131ª .718
Total 4 23 27
Education about proper posture
Yes
No 2 7 9
2 16 18 .587ª .444
Total 4 23 27
Implement proper body mechanics No 1 5 6
Yes 1 14 15
Not applicable 2 4 6 2.436ª .296
Total 4 23 27
about proper ergonomics (62%), increasing the number
of sonographers and adding regular stretching exercise
(59%), adding regular short breaks (40%), decreasing the
work hours (25%), and made changes in the workplace
(18%).
3.3. Awareness
Regarding the awareness in Microbiology technician, we
found that 83% who know the meaning of ergonomics,
88% who think poor ergonomics lead to health risk, 50%
who get an education about proper posture and body
mechanics, and 44% who implemented the appropriate
posture and body mechanics. In Ultrasound sonogra-
phers, we found that 85% who know the meaning of
ergonomics, 81% who think poor ergonomics lead to
health risk, 66% who get an education about proper pos-
ture and body mechanics, and 55% who implemented
the proper posture and body mechanics. (see Table 4 for
further information).
The current study ndings showed that there are
signi cantly higher feelings of pain and discomfort in
female compared to male participants. This nding is

Fayz Al Shahry et al.
600 ERGONOMIC EFFECTS ON WORKERS OF SELECTED HEALTHCARE AREAS BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
by what had been previously reported in the literature,
where the current human results concerning sex differ-
ences in experimental pain indicate greater pain sen-
sitivity among females compared with males for most
pain modalities. Additionally, many previous studies
con rmed differences between genders and documented
that women are more likely to experience musculoskel-
etal pain, (Cook et al., 2000, Ranasinghe et al., 2011).
In line with the study of Kaliniene et al. (2016), the
current study showed that low back pain was the high-
est prevalent type of pain among the studied cohort.
Additionally, a similar study conducted in Nigeria, and
the authors found a high preponderance of upper and
lower back pain Kayoed et al. (2013). The predominant
involvement of the back, as observed in the current
study, also is in agreement with reports of studies carried
out in Roma, British Columbia, and United States, (Pike,
et al. 1997, Mirk,et al 1999). Additionally, shoulder pain
was among the most reported pain positions in the cur-
rent study and in that of Kaliniene et al. (2016).
The current study nding highlighted the point that
the lack of attention to ergonomics could lead to dam-
age to the healthcare workers mainly in the form of mus-
culoskeletal pain, stress injuries and eye strain which
can lead to increase the workers’ fatigue and decrease
their productivity, and this is in accordance with what
has been reported in the literature, (Hills et al., 2012). It
has been demonstrated that MSDs are highly relevant
in the context of work and that the current economic
and social implications of these conditions are sizeable
and often underestimated. There are some types of jobs
and speci c sectors including home care and nursing,
represent a heightened risk of developing or aggravating
MSDs. The converse of work environments that aggra-
vate MSDs is that work context can also contribute to
improvements in MSD outcomes mainly through ergo-
nomic design and job duty adjustment, (Summers, et al.,
2015).
In sonography, surveys done among American and
Canadian sonographers in 1997 showed that the inci-
dence of MSDs was 84%; however, this incidence had
increased to 90% (Evans et al., 2009). An ergonomic
workstation in sonography according to Baker and
workers should include an ergonomic task chair, the
chair should be easy to operate and be adjustable from a
settled position, has a different lift, vinyl upholstery that
is antimicrobial, a foot ring, special casters, and detailed
instructions on its use for different types of studies,
however, then they reported that the ergonomic features
of the examination room equipment are only as good as
the workers willingness to use them, (Baker et al., 2015)
.
The effectiveness key of these features is changing
the worker work postures so that they maintain neutral
postures for the majority of each examination. Comfort-
able work postures can make any ultrasound worksta-
tion ergonomic, increase worker comfort, reduce injury
risk, and impact the quality of patient care Baker et al.
(2015). In the Nigerian study published in 2013, the most
signi cant proportion of the participants reported that
the use of chairs of low height and scanning chair both
precipitated and aggravated their symptoms and feeling
with pain, and they recommended the use of chairs and
scanning tables of ideal heights that can decrease risks
to musculoskeletal disorders associated with Ultrasonog-
raphy, (Kayoed et al., 2013). The current study partici-
pants reported that their primary complaint and width.
For ultrasound practitioners, to empower safe working
practices the room should was from the chairs type be of
an adequate size, (Tayyari et al., 1997) with lighting that
does not cause glare on the monitor and heating that is
suitable for the working conditions, (Baker et al., 2015
and Harrison et al., 2015).
This is in line with what the current respondents
reported that narrow space is one of the common fac-
tors of their complaint. Massage and stretching exercises
were the most common techniques and changes that
sonographers in the current study used to decrease the
pain related to work. Harrison and Harris (2015) in their
review concluded that there are many factors involved
in the prevention or the reduction of work-related MSDs
for ultrasound practitioners. These factors include ergo-
nomic issues, management of workload, psychosocial
factors, physical factors and general tness levels. Sun-
ley et al. (2006) highlighted that ergonomics education
for staff is essential to ensure that they are aware of best
practice guidelines, ways of risk reduction to themselves
and others and how to report and monitored pain and
injury to ensure a long and healthy career, (Sunley et al.,
2006). In the current study, results indicated that there is
a shortage in ergonomics education; additionally, a high
percentage of the respondents show their wish to receive
education and training about ergonomics.
As per the results of several studies, the effects of
occupational MSD interventions have been particu-
larly strong when using a multi-branched intervention
approach, combining physical exercise with another
component, like worksite ergonomic changes, (Dawson
et al., 2007, Holtermann et al., 2010). Unfortunately,
none of the participants in the current study tried to
visit occupational therapy clinics to get help and educa-
tion about some techniques and changes that help to
decrease and eliminate pain and injuries related to work.
For healthcare workers, the previous study has shown
that social, environmental factors such as work demands
and social support are related to report MSDs, (Sorensen
et al., 2011), which is almost the same with our study
ndings. Taken together with the evidence from previ-
ous interventions, these ndings support intervention
Fayz Al Shahry et al.
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS ERGONOMIC EFFECTS ON WORKERS OF SELECTED HEALTHCARE AREAS 601
strategies that incorporate targeted changes to the phys-
ical and social work environment along with worker
education.
For tackling MSDs at work, several preventive strate-
gies can be taken. These prevention strategies primar-
ily include risk assessment, and technical/ergonomic,
organizational and person-oriented intervention. The
secondary prevention strategy involves the identi ca-
tion and health monitoring of workers at risks, while the
tertiary prevention strategy comprises a return to work
actions, Mirk et al., 1999, EU-OSHA 2008. Suggestions
of the current study respondents regarding a solution to
decrease and eliminate pain related to work were within
the context of those prevention strategies with adding
regular short breaks being the highest scored sugges-
tion. In line with this nding, a previous study identi ed
that lack of rest breaks and use of facilities that are not
ergonomic were the main contributing factors to work-
related MSDs Kayoed et al. (2013).
Some studies on sonographers have also linked reg-
ular breaks and reduced workload to reduced muscu-
loskeletal symptoms, Schoenfeld et al. (1999). On the
other hand, the work of Schoenfeld et al. (2013) did not
nd reduced scanning frequency to be associated with
reduced symptoms among sonographers. Microbiology
technicians participated in the current study showed
a right awareness level with the term “ergonomics,” a
result which is better compared to the Nigerian research
about awareness and knowledge of ergonomics among
medical laboratory scientists, in which awareness of
ergonomics and knowledge of gains of its right applica-
tion was reduced, Oladeinde et al. (2015).
Additionally, it is better than what recorded elsewhere
among computer users and manufacturing workers, (Loo
et al., 2012, Shantakumari et al., 2012). The strengths
of this study include that the data about ergonomics is
scarce in Saudi Arabia, and to the best of our knowl-
edge, this is the rst study in Saudi Arabia that assesses
the ergonomic effects on workers of selected healthcare
areas. Second, healthcare workers especially those who
participate in interventional procedures such as labo-
ratory and radiology are well known and more prone
to have musculoskeletal pain. Third, the data come
from one of the biggest national hospitals in Riyadh.
This study has some limitations including mainly the
small sample size in microbiology technicians, and the
participants were only from one healthcare institution.
The results of this study may be further enhanced in the
future by increasing the sample size.
CONCLUSION
In conclusion, there is a signi cant effect of ergonomic
on sonographers and the laboratory technicians. The
study showed a good level of knowledge and awareness
about ergonomics; however, still, there is a quite high
percentage of them who did not receive health education
on ergonomics and also a high percentage who aren’t
implementing it. There is a need for educational and
implementation empowerment programs in this regard.
REFERENCES
Agrawal Parul R, Maiya Arun G, Kamath V, Kamath A. (2015)
Musculoskeletal Disorders among Medical Laboratory Profes-
sionals-A Prevalence Study. Journal of Exercise Science and
Physiotherapy. 10(2):77.
Baker JP, Cof n CT. (2013) The importance of an ergonomic
workstation to practicing sonographers. J Ultrasound Med.
Aug; 32(8):1363–75.
Bergische Universität Wuppertal, pp. 72 Available at: www.
dguv.de/content/prevention/campaigns/msd/review/ap_4_e.pdf
Brooks A. (1998) Ergonomic approaches to of ce layout and
space planning. Journal of Facilities.; 16(3/4):73-78.
Cook C, Limerick BR, Chang S. (2000) The prevalence of neck
and upper extremity musculoskeletal symptoms in computer
mouse users. Int J Ind Ergon.; 26:347–56.
Dawson AP, McLennan SN, Schiller SD, Jull GA, Hodges PW,
Stewart S. (2007) Interventions to prevent back pain and back
injury in nurses: a systematic review. Occup Environ Med. Oct;
64(10):642–50.
Estryn-Behar M, Kaminski M, Peigne E, Maillard M, Pelletier
A, Berthier C et al. (1990) Strenuous working conditions and
musculo-skeletal disorders among female hospital workers.
International Archives of Occupational and Environmental
Health; 62(1):47-57.
EU-OSHA - European Agency for Safety and Health and
Work, (2008) Work-related musculoskeletal disorders: pre-
vention report, Publications Of ce of the European Union,
Luxembourg,pp.106.Availableathttps://osha.europa.eu/en/
publications/reports/en_TE8107132ENC.pdf/view.
Goyal N, Jain N, Rachapalli V. (2009) Ergonomics in radiology.
Clinical Radiology.; 64(2):119-126.
Harrison G, Harris A. (2015) Work-related musculoskeletal dis-
orders in ultrasound: Can you reduce risk? Ultrasound. Nov;
23(4):224–30.
Hills DJ, Joyce CM, Humphreys JS. (2012) A national study of
workplace aggression in Australian clinical medical practice.
The Medical Journal of Australia. Sep 17; 197(6):336–40.
Holtermann A, Mortensen OS, Burr H, Søgaard K, Gyntelberg
F, Suadicani P. (2010) Physical work demands, hypertension
status, and risk of ischemic heart disease and all-cause mortal-
ity in the Copenhagen.
Jaffar N. (2011) A Literature Review of Ergonomics Risk Fac-
tors in Construction Industry. Procedia Engineering.; 20:89-97.
Kaliniene G, Ustinaviciene R, Skemiene L, Vaiciulis V, Vasilav-
icius P.(2016) Associations between musculoskeletal pain and
work-related factors among public service sector computer

Fayz Al Shahry et al.
602 ERGONOMIC EFFECTS ON WORKERS OF SELECTED HEALTHCARE AREAS BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
workers in Kaunas County, Lithuania. BMC Musculoskelet Dis-
ord. 07; 17(1):420.
Kayoed I. Oke and A. A. Adeyekun. (2013) Patterns of Work-
related Musculoskeletal Disorders among Sonographers in
selected Health Facilities in Nigeria. Journal of Applied Medi-
cal Sciences, vol. 2, no. 4, 67-76
Kevin Evans, Shawn Roll, Joan Baker .(2009) Work-Related
Musculoskeletal Disorders (WRMSD) Among Registered Diag-
nostic Medical Sonographers and Vascular Technologists: A
Representative Sample. Journal of Diagnostic Medical Sonog-
raphy. Nov 1; 25(6):287–99.
Kuiper J, Burdorf A, Verbeek J, Frings-Dresen M, van der Beek
A, Viikari-Juntura E. (1999) Epidemiologic evidence on man-
ual materials handling as a risk factor for back disorders:a sys-
tematic review. International Journal of Industrial Ergonom-
ics.; 24(4):389-404.
Lee K. (2017) Ergonomics in total quality management: How
can we sell ergonomics to management? Journal of Ergonom-
ics.; 48:5,547-558.
Loo HS, Richardson S, Alam S. (2012) Ergonomics issues in
Malaysia. J Soc Sci. 8:61–5.
Magnavita N, Bevilacqua L, Mirk P, Fileni A, Castellino N.
Work-related musculoskeletal complaints in sonologists. J
Occup Environ Med. 1999 Nov; 41(11):981–8.
Mcatamney L, Corlett E. (2007) Ergonomic workplace assess-
ment in a health care context. Institute for Occupational Ergo-
nomics, University of Nottingham.; 35(9):965-978.
Michaelis, M., IPP-aMSE (2009) Identi cation and prioriti-
sation of relevant prevention issues for work-related mus-
culoskeletal disorders (MSD) - Work package 4 - Prevention
approaches: evidence-based effects and prioritised national
strategies in other countries,
Mirk P, Magnavita N, Masini L, Bazzocchi M, Fileni A. (1999)
Frequency of musculoskeletal symptoms in diagnostic medi-
cal sonographers. Results of a pilot survey]. Radiol Med. Oct;
98(4):236–41.
Mirk, P L. Magnativa, M. Bazzocihi and A. Fileni. (1999) Fre-
quency of musculoskeletal symptoms in diagnostic medical
sonographers. Review of a pilot survey. Radiol. Med., 98(4),
236-41
Oladeinde BH, Ekejindu IM, Omoregie R, Aguh OD. (2015)
Awareness and Knowledge of Ergonomics among Medical
Laboratory Scientists in Nigeria. Ann Med Health Sci Res. Dec;
5(6):423–7.
Pao T, Kleiner B. (2001) New developments concerning
the occupational safety and health act. Managerial Law;
43(1/2):138-146.
Pike, J. Russo, Berkowitz, J.P. Baker and V.A. Lessoway. (1997)
The prevalence of musculoskeletal disorders and related work
and personal factors among diagnostic medical sonographers.
J Diag Medical Sonography, 13(5), 219-227.
Ranasinghe P, Perera YS, Lamabadusuriya DA, Kulatunga S,
Jayawardana N, Rajapakse S, et al. (2011) Work related com-
plaints of neck, shoulder and arm among computer of ce
workers: a cross-sectional evaluation of prevalence and risk
factors in a developing country. Environmental Health.;
10:70.
Ruess L, O’Connor S, Cho K, Hussain F, Houuard W, Slaughti
R et al. (2003) Carpal Tunnel Syndrome and Cubital Tunnel
Syndrome: Work-Related Musculoskeletal Disorders in Four
Symptomatic Radiologists. American Journal of Roentgenol-
ogy.; 181:37-42.
Schoenfeld A, Goverman J, Weiss DM, Meizner I. (1999) Trans-
ducer user syndrome: an occupational hazard of the ultra-
sonographer. Eur J Ultrasound. Sep; 10(1):41–5.
Shantakumari N, Eldeeb RA, Sreedharan J, Gopal K. (2012)
Awareness and practice of computer ergonomics among uni-
versity students. Int J Med Health Sci.; 1:16–20.
Siegal D, Levine D, Siewert B, Lagrotteria D, Affeln D, Denner-
lein J et al. (2010) Repetitive Stress Symptoms Among Radiol-
ogy Technologists: Prevalence and Major Causative Factors.;
7:956-960.
Sorensen G, Stoddard AM, Stoffel S, Buxton O, Sembajwe G,
Hashimoto D. (2011) The role of the work context in multiple
wellness outcomes for hospital patient care workers. J Occup
Environ Med. Aug; 53(8):899–910.
Summers, K., Jinnet, K. & Bevan, S. (2015). Musculoskeletal
disorders, workforce health and productivity in the United
States. The Work Foundation. London, pp 40.
Sunley K. (2006) Prevention of Work-Related Musculoskeletal
Disorders In Sonography. London: Society of Radiographers,
Tayyari F, Smith J .Occupational Ergonomics: principle and
application. London: Chapman & Hall; 1997. P. 4-214.
Yelin E, Trupin L, Sebesta D. (1999) Transitions in employment,
morbidity, and disability among persons ages 51–61 with mus-
culoskeletal and non-musculoskeletal conditions in the US,
1992–1994. Arthritis & Rheumatism.; 42(4):769.