
Cross cultural validation of functional autonomy
measurement system (SMAF) into Arabic geriatric
rehab-culture
Albandary Alhadlaq
1
, Saleh Al Oraibi
2
, Fayz S. Al-Shahry
3
, Areej Al-Hawas
4
,
Lamya Al-Qurashi
4
and Mona Al-Otibiy
4
1
Occupational Therapy Student CAMS, KSAU-HS, Riyadh Saudi Arabia
2
Professor
3
Assistant Professor CAMS KSAU HS Consultant Rehabilitation, KSAU-HS, Riyadh Saudi Arabia
4
Occupational Therapy Students, KSAU-HS, Riyadh Saudi Arabia
ABSTRACT
The Functional Autonomy Measurement System (FAMS) measures functional ability in Five domain: mobility, activities of daily liv-
ing, instrumental activities of daily living, mental function and communication. FAMS however was validated into many languages
such are English, Spanish, Japanese and Dutch, but it was not validated into Arabic. So, it may not suit Arabian cultures and society.
Thus, the validation of FAMS into Arabic is vital. The aim therefore was to validate FAMS into Arabic culture. This is a prospective
cross-sectional design. The study was conducted in Riyadh at King Abdul-Aziz Medical city (KAMC), in King Fahad Hospital (KFH)
/in rehabilitation department. The FAMS was translated from original English version into Arabic. Translated Arabic version was
distributed to 30 health professionals who work in rehabilitation department to check it for contents and accordingly FAMS was
modi ed. Then, the nal modi ed version of Arabic FAMS was distributed to 30 Saudis elderly who are 60 years old and above to
test the question applicability and clarity. The results showed a measure of the internal consistency of our study by using Cronbach’s
alpha. The optimal value of this test is 0.7 and above. So, we found the value of our study was more than 0.7. The value was 0.9 for
the 5 domains (ADL, Mobility, Communication, Mental function, IADL) which means it reliable for Arabic patients in Arabic cultures.
The result revealed a new Arabic version of important assessment tool in the eld of rehabilitation for the rst time ever. The internal
consistency of the FAMS assessment tool is in line with other previous similar validation research globally. Conclusion and clini-
cal implications: The new translated Arabic version of FAMS was produced with Arabic cultural modi cations. Further studies are
needed to test this important assessment tools with larger population of Arab patients.
KEY WORDS: SOCIAL FUNCTIONING, FUNCTIONAL AUTONOMY, INSTRUMENTAL ACTIVITIES, OLDER PEOPLE, VALIDITY, ARABIC CULTURE
548
Medical
Communication
Biosci. Biotech. Res. Comm. 11(4): 548-555 (2018)
ARTICLE INFORMATION:
Corresponding Authors: shahryf@hotmail.com
Received 12
th
Oct, 2018
Accepted after revision 19
th
Dec, 2018
BBRC Print ISSN: 0974-6455
Online ISSN: 2321-4007 CODEN: USA BBRCBA
Thomson Reuters ISI ESC / Clarivate Analytics USA
Mono of Clarivate Analytics and Crossref Indexed
Journal Mono of CR
NAAS Journal Score 2018: 4.31 SJIF 2017: 4.196
© A Society of Science and Nature Publication, Bhopal India
2018. All rights reserved.
Online Contents Available at: http//www.bbrc.in/
DOI: 10.21786/bbrc/11.4/3
Albandary Alhadlaq et al.
INTRODUCTION
The Functional Autonomy Measurement System (FAMS)
is a tool which developed in 1984 by a team from the
Community Health Department at Hôtel-Dieu in Lévis to
measure the demands and needs of the elderly handi-
capped (Hébert, Guilbault, Desrosiers, & Dubuc, 2001;
Hébert, Carrier, & Bilodeau, 1988). SMAF quanti es the
functional ability on 29-items scale which developed by
World Health Organization’s classi cation of impair-
ments, handicaps and disabilities (Hébert, Robichaud,
Roy, Bravo, & Voyer, 2001). It measures functional abil-
ity in 5 sectors: mobility [6 items], activities of daily
living (ADL) [7 items], instrumental activities of daily
living (IADL) [8 items], mental functions [5 items] and
communication [3 items] (Hébert, et al, 2001). These
items were standardized using four-level measurement
scale. Level 0: autonomous, Level 1: needs supervision
or stimulation, Level 2: needs help, and Level 3: depend-
ent (Hébert, et al 2001; Hébert et al, 1988; Hébert, et al,
2001). According to the occupational therapy practice
framework: Doman & process, activities of daily living
(ADLs) are activities that are specialized toward taking
care of one’s own body. Which are bathing, shower-
ing, toileting and toilet hygiene, dressing, swallowing/
eating, feeding, functional mobility, personal device
care, personal hygiene and grooming, and sexual activ-
ity (Amini, D. A., Kannenberg, K., Bodison, S., Chang,
P., Colaianni, D., Goodrich, B., & Lieberman, D., 2014).
Not all the ADLs covered in the SMAF. The seven items
included in SMAF are eating, washing, dressing, groom-
ing, urinary continence, facial continence, and toileting
(Hébert, Guilbault et al 2001).
Instrumental activities of daily living (IADLs) as in
occupational therapy practice framework are “activities
to support daily life within the home and community”
(Amini et al, 2014) Care of others, care of pets, child
rearing, communication management, driving and com-
munity mobility, nancial management, health manage-
ment and maintenance, home establishment and man-
agement, meal preparation and cleanup, religious and
spiritual activities and expression, safety and emergency
maintenance, and shopping are all considered IADLs”
(Amini et al, 2014)
IADLs in the SMAF are meal preparation and cleanup,
nancial management, shopping, health management
and maintenance, driving and community mobility,
home establishment and maintenance (cleaning the
house, and doing the laundry), and communication
(Hébert, et al, 2001).
Disability is any restriction or lack (resulting from
an impairment) of ability to perform an activity in the
manner or within the range considered normal for a
human being (World Health Organization,1980) World
Health Organization classi ed the disability into 9 cate-
gories (World Health Organization,1980). The rst one is
behavior disabilities which mention to a person’s aware-
ness of himself, others, their roles and occupations,
places, and time (World Health Organization,1980). The
second one is communication disabilities that refer to
person’s ability to communicate with other such as dis-
ability in speaking, listening, seeing, and writing (World
Health Organization,1980). The third is personal care
disabilities which mean the person’s ability to take care
of himself, his personal hygiene, dressing, feeding, and
getting to bed (World Health Organization,1980). The
fourth is locomotor disabilities which are disability in
the walking, climbing stairs, running, transfer, transport,
and lifting (World Health Organization,1980). The fth
is body disposition disabilities that mean the person’s
ability to carry out his own activities such as prepar-
ing food, cocking, serving food, reaching, and kneeling
(World Health Organization,1980). The sixth is dexterity
disabilities that refer to skill body movement such as
modify the environment, moving and handling objects,
ne motor control, and body control (World Health
Organization,1980).
The seventh is situational disabilities that are disabil-
ity in dependence, endurance, and disability in tolerance
in the temperature, noise, and work stress (World Health
Organization,1980).
The eighth is particular skill disabil-
ities that is disability in behavior such as intelligence,
motivation, perception, learning, orientation, and con-
centration, and disability in achievement the tasks such
as problem solving, adaptability, and accuracy (World
Health Organization,1980). The last one is other activity
restrictions; this section has been developed, in order to
develop some of the categories that were not mentioned in
the previous classi cations (World Health Organization,
1980).
FAMS was validated into many languges such as
English, Spanish, Japanese and Dutch, but it was not
validated into Arabic. So, it may not suit our cultures
and society (Desrosiers et al., 1995). Thus, the validation
of FAMS into Arabic is vital (Desrosiers et al, 1995). It
would help occupational therapists who work with peo-
ple with disabilities and elderly who live in Arab coun-
teries and speak Arabic languges in evaluating the areas
of disability in them (Desrosiers et al, 1995).
Validation and realibility are independent on each
other. A measurement maybe valid but not reliable,
or reliable but not valid. Relibility is the reapition of
ndings (Kimberlin, & Winterstein, (2008). Validity of
a test is that it measure what it is supposed measures
(Kimberlin et al, 2008). We conducted this study to vali-
ate SMAF culturally into Arabic culture. We choose pro-
spective cross-sectional design to insure the willing of
the participants.
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS CROSS CULTURAL VALIDATION OF FUNCTIONAL AUTONOMY MEASUREMENT SYSTEM 549
Albandary Alhadlaq et al.
550 CROSS CULTURAL VALIDATION OF FUNCTIONAL AUTONOMY MEASUREMENT SYSTEM BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
Literature Review
In 2009 Yount and Sibai found that By 2045-2050, the
researchers expected that most (20 of 23) Arab popula-
tions are have at least 10 percent of population aged
60 and older. Hence, the Arabic country which have a
largest number of elderly presently lived in it is Egypt
(Yount & Sibai, 2009). The epidemiological research in
Arab countries has been focused on non–communicable
disorders and mostly on those of the circulatory system
(Yount et al, 2009). The differences in Physical depend-
ence with elderly are noted through out Arab countries
with a high prevealance of ADL, IADL dif culties (Yount
et al, 2009). The highest rates of limitations in ADL were
shown in Tunisia, Egypt, Jordan and Lebanon (those
reported between 25 and 38 percent) these countries fol-
lowed by the UAE and Saudi Arabia which have between
17-19 percent (Yount et al, 2009). The limitations in
ADL and IADL due to disability among women more
than among men. However, there is lacking of measure-
ment tools to assess functional limitations resulting In
over-reporting of disabilities by the persons with dis-
ability (Yount et al, 2009). Based on that the women
have shown higher dif culties in performing physicals
tasks than men in Egypt, Tunisia, Jordan and Lebanon,
but Egypt was reported as highest rates of restriction
in performing physical tasks (PT) by 71 percent in men
and 88 percent in women (Yount et al, 2009). Yount
et al opined that capability to perform physical tasks
(PT) is the most commonly used measurement to evalu-
ate disability among elderly (Yount et al, 2009). “This
measure is presumably independent of one’s physical
and social environment (e.g., cultural and gender roles),
which would increase its validity and reproducibility
and thereby make it preferable to measures of ADL and
IADL disability” (Yount et al, 2009)
In two Canadian’s studies used the SMAF as a meas-
ure using same study designs. Both studies used qusi-
experimental design with elderly group patients aged
75 years. The rst study included 151 elderlies from the
geriatric day hospital and the second study included
1,501 persons identi ed at risk of functional decline
(Tousignant, et al 2003; Hébert, et al 2009).
In another study using FAMS, they nd that this tool
was important tool to reduce elderly functional decline
by identifying functional limitation at early stage, and
Similarly Hébert Brayne, and Spiegelhalter used SMAF
tool to measure functional movement, this helped identify
risk factors of dependency and this helped to reduced the
period of dependency in elderly group (Hébert, R., 1997;
Hébert, R., Brayne, C., & Spiegelhalter, D, 1999).
Other functional studies carried out with elderly
agreed that SMAF is very important tool and instrument
synthesizes and systematizes the various scales proposed
to measure the functioning of the elderly or disabled
(Mercier, et al, 2001; Pinsonnault, et al, 2003; Wales,
et al, 2016). In All previous studies, they recruited simi-
lar age groups of fty- ve to seventy fe years old. All
these studies were helped to evaluate the needs of indi-
viduals (elderly) by measuring the disabilities and the
handicaps with which they are af icted. These studies
indicate that the FAMS is vital tool to measure the func-
tional movement and independency in elderly groups as
well as in people with disabilities. These very important
in occupational therapy practice, make it worth study-
ing it and translated and validated for people from other
cultures rather than only people from western culture.
Additionally, another study aimed to apply the ISO-
SMAF classi cation to funding long-term care facilities
in one area of the Province of Quebec and to compare
the results of this new funding methodology to the for-
mal methodology (Desrosiers, et al, 2004).
FAMS was validated into many languges such are
English, Spanish, Japanese and Dutch, but it was not
validated into Arabic. So, it may not suit our cultures
and society (Desrosiers et al 1995). Thus, the validation
of SMAF into Arabic is vital. The aim of this study is to
valiate SMAF into Arabic culture. It would help occu-
pational therapists who work with people with disabili-
ties and elderly who live in Arab counteries and speak
Arabic languges in evaluating the areas of disability in
the Arabic elderly (Desrosiers et al, 1995). In the future,
when there is an Arabic version, the method of evaluat-
ing elderly will be easy for the specialist and for patients.
Also on the specialists’ side it will be comfortable and
easy for them because they will not make much effort
to explain the point to patients, and it will save a lot of
their time and effort (Desrosiers et al, 1995).
METHODS
The study was about cultural validation of Functional
Autonomy Measurement System (FAMS) into Arabic
culture. The study was conducted in Riyadh at King
Abdulaziz Medical city (KAMC), in King Fahad Hospi-
tal (KFH) speci cally in rehabilitation department. The
capacity of beds in KAMC is 1501 beds. In 2003, the
rehabilitation unite was only for neurological rehabilita-
tion. The neurological rehabilitation unite expanded to
be a rehabilitation department at 2004. Now, the reha-
bilitation department involve occupational and physi-
otherapy unites, In vitro fertilization (IVF), OB, medical
imaging, laboratory, pharmacy, and continues renova-
tion of patients’ wards. (Ngha.med.sa. 2018). The Ara-
bic version of FAMS was administered among 30 health
providers in rehabilitation team including occupational
therapists, physical therapists, physicans, nurses and
30 elderley patients 60 years and over after following
the inclusion and exclusion criteria. The inclosion cri-
Albandary Alhadlaq et al.
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS CROSS CULTURAL VALIDATION OF FUNCTIONAL AUTONOMY MEASUREMENT SYSTEM 551
30 but we found only 19 health pro ssionals in reha-
bilitation team who are Arabic native speaker and for
Saudi elderly clients over 60 years the sample size were
30 also. There is no randomization needed for this study.
Purposeful sampling was used which means to select
people who are willing to participate and available. The
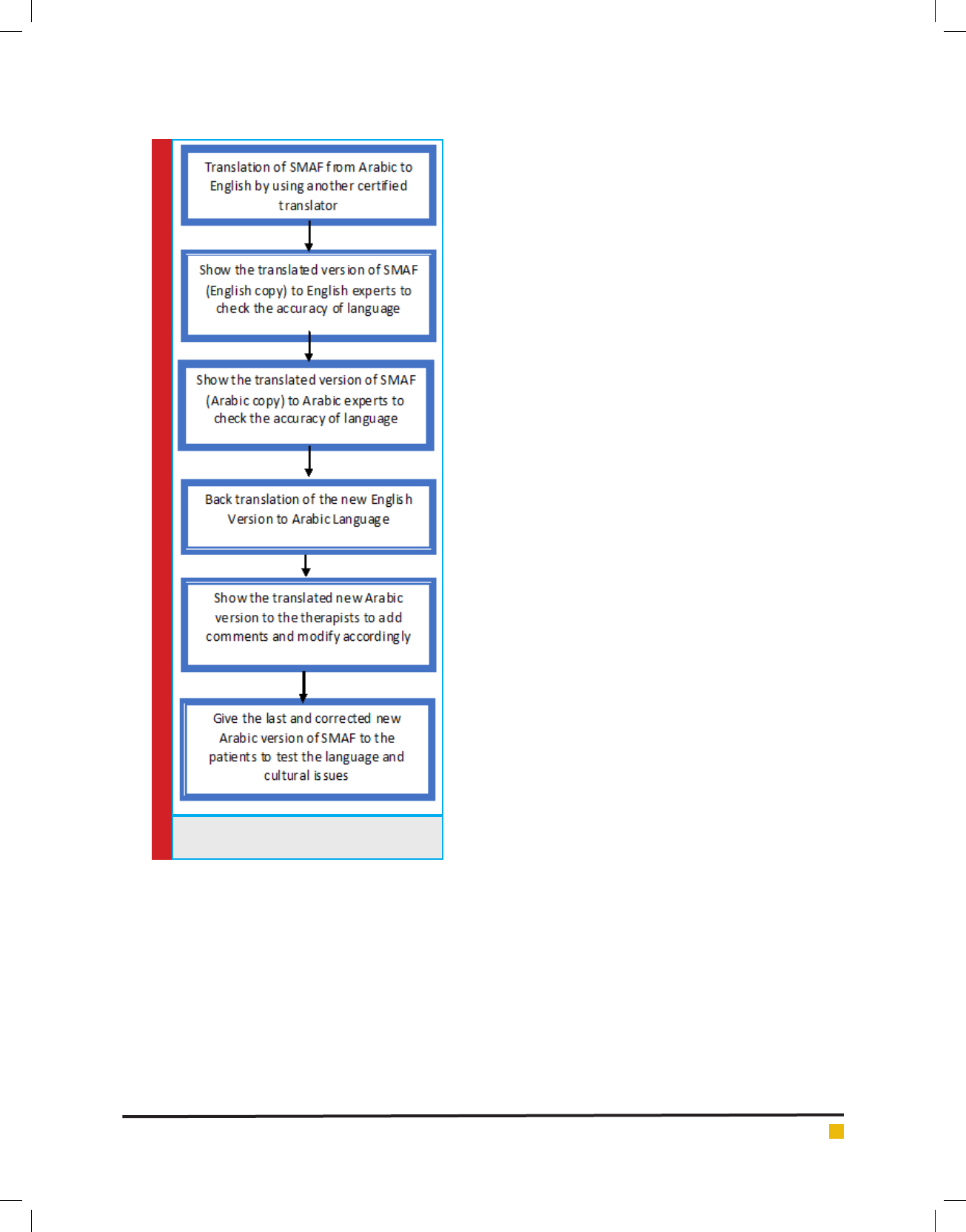
steps involved in the validation of SMAF to Arabic cul-
ture is given in Figure 1 and detailed as below.
Stage I & II: Initial Translation
The rst and second stage in adaptation were the for-
ward translation. Two forward translations were made
by two different certi ed translators. One certi ed trans-
lator was translated from English language into Arabic
language, and then second translator was translated the
tool from the new Arabic version into English language.
Stage III & IV: Synthesis of The Translations
The third stage was to compare between the old English
and the new English version to nd any discrepancies and
modify them. The fourth stage was to give the new Arabic
version to Arabic language expert to check it for errors.
Stage V: Back Translation
The fth stage was to translate the new English into
Arabic language; This is a process of validity checking
to make sure that the translated version is re ecting the
same item content as the original versions.
Stage VI: Expert Committee
The sixth stage was to consult therapists about the new
Arabic version and to receive their comments on it with-
out using survey. Based on the comments from expert
committee, modi cation was done on the Arabic version
of FAMS.
Stage VII: Test of the Pre-Final Version
The nal stage of adaptation process was the pretest.
This eld test of the new questionnaire seeks to use the
pre- nal version in subjects. Ideally, 30 persons were
tested.
Accordingly, the nal Arabic version of FAMS was
edited and nalized and released to be used in upcom-
ing studies.
Ethical consideration and data management/
statistical plan:
Ethical consideration:
Approval from IRB (King Abdullah Medical Research
Center) was sought. An informed consent was completed
prior to data collection. The researchers were safeguard
the con dentiality of participants of the study. Personal
data was stored on a computer with accessibility only to
FIGURE 1. Validation of SMAF to Arab
culture
teria of this stude was the elderly should be 60 year-
old and above, assess both genders and for those who
have loss or limited of function. Howevere, participants
who were below 60 year-old and anyone who have cog-
nitive impairment were excloded from this study. The
design for this study was prospective cross sectional. The
sample size of this study was determined by the previ-
ous validation process in previous studies as listed in
the reference list, (Beaton et al, 2000, Elboim-Gabyzon,
et al 2015).
So, the estimated sample size for health providers
who work in rehabilitation department in KAMC were
Albandary Alhadlaq et al.
552 CROSS CULTURAL VALIDATION OF FUNCTIONAL AUTONOMY MEASUREMENT SYSTEM BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
the researchers. Subject data was coded and names were
not used in any of the documents related to this study.
Data management/ statistical plan:
Data was analyzed using SPSS statistical software,
version 22. Descriptive statistics of means was used.
Response frequencies and means or medians for the
survey items were determined and displayed in tabu-
lar formats. After we completed the pilot study with 30
patients, the reliability of the new questionnaires items
was tested using Cronbach’s alpha.
RESULTS
The rst stage was the distribution of the Arabic version
of FAMS to nineteen native Arabic speakers both female
and male health professionals who work in rehabilita-
tion team to make sure that it is clear and valid for Ara-
bic culture. After two weeks, we received the distributed
FAMS. Following analysis of the data, twelve of them
were satis ed and happy with the objective and iden-
tify that the objective of Arabic version is the same as
the objective of original version. However, some of the
participants suggested that for cultural purpose this tool
needs to be completed by face to face interview instead
of lling the form subjectively. The second step, after
taking the opinions of experts into consideration and
making modi cations for the tables arrangement and
sentence structure, we distributed the Arabic FAMS to
thirty female and male Saudi elderly. The age group of
the validation of FAMS differ from country to another,
in Arabic culture elderly stage starts at sixty which is the
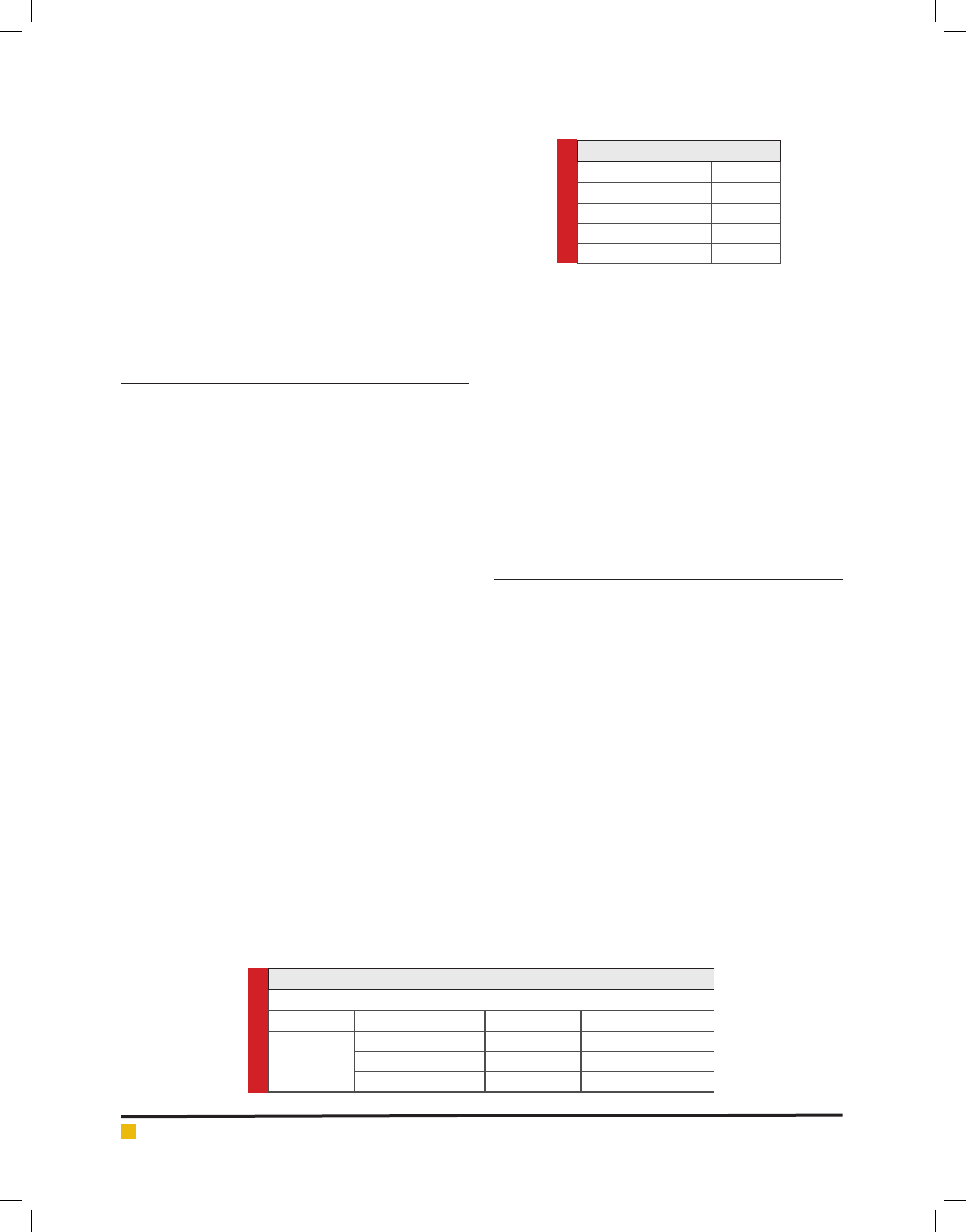
retirement age in Arab countries. The mean of elderly
participants age was 71.6 as seen in table 1.
The participants in this research were representative
for Arabic culture. They have different level of educa-
tion; Master degree, Bachelor degree, high school, mid-
dle school, elementary school, and illiterate. Those par-
ticipants differ in health status, some of them were in
good health, however; others have chronic condition
such as Diabetes, Irritable Bowel Syndrome, Hyperten-
sion, Osteoporosis, and Rheumatoid Arthritis and sever
health conditions such as Hemodialysis, Breast Cancer,
and heart disease. The female participants were twenty-
one and male participants were nine as seen in table 2.
The result of distributing the FAMS to elderly in Arab
culture was clear, simple, and easily understood for the
participants. They satisfyingly answered all the ques-
tions of the Arabic version of FAMS. As a result, the
Arabic version of FAMS is valid to be used with elderly
in all Arab countries.
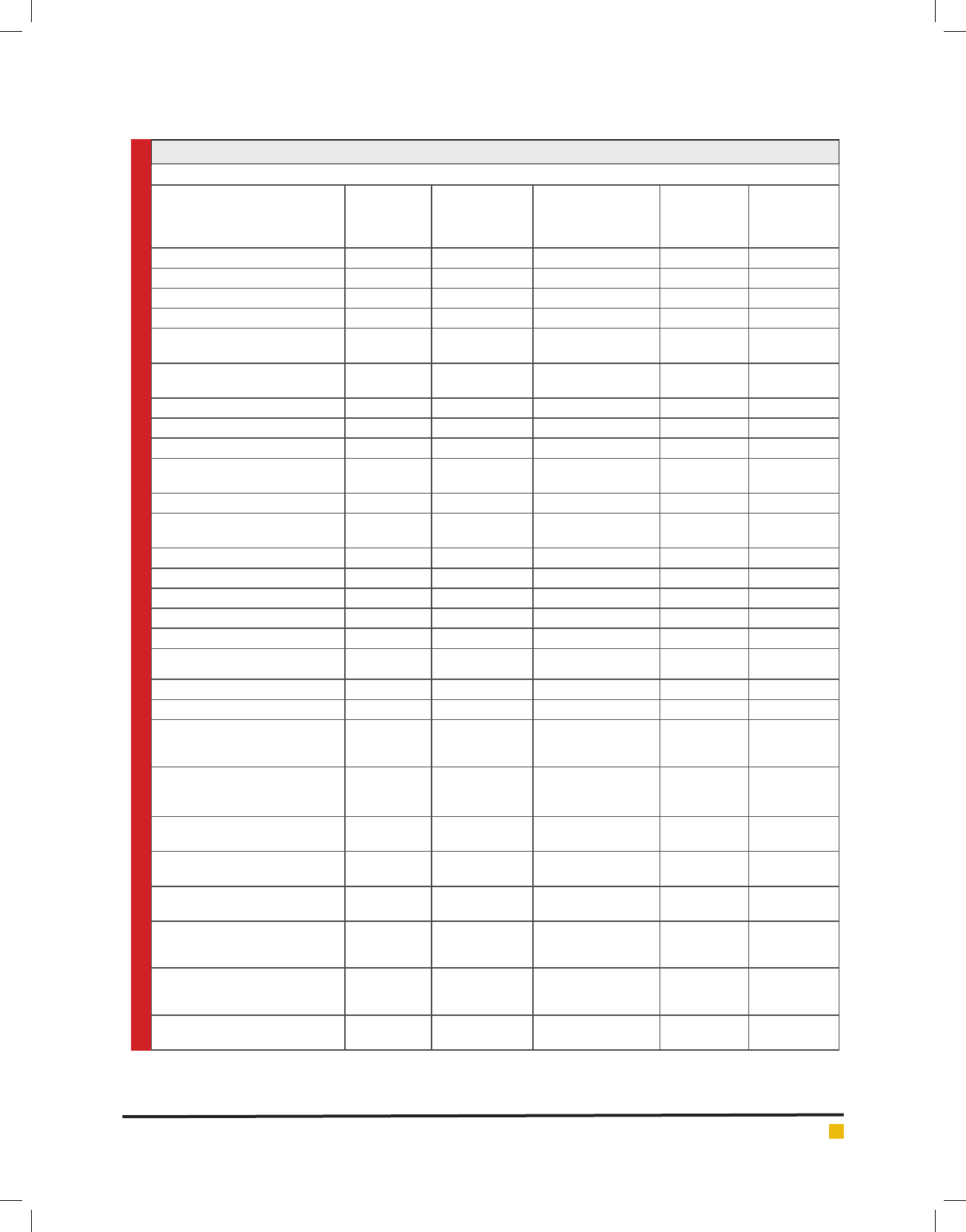
We used Cronbach’s Alpha to measure the validity of
the tool. The value of activity of daily living (ADL) was
0.914. And the value of mobility was 0.914. Also, the
value of communication was 0.918. The value of mental
function was 0.917. The value of instrumental activities
of daily living (IADL) was 0.913. The optimal value of
this test is 0.7 and above. The result that we found for
all items in SMAF was 0.9 as seen in table 3.
DISCUSSION
The suitability of the content of FAMS for elderly people
was reliable and valid and widely used in many coun-
tries. however the application of this scale in other non-
English speaking made the outcomes nonspeci c and
weary. In the Arab countries a notable boundaries were
addressed by patients and families during the applica-
tion of the FAMS in English version. the variation in
the language interpretation and diversity in the meaning
between Arabic and English was a real barrier. therefore
this study was of extreme importance and the optimiza-
tion of interpretation of the FAMS was the real chal-
lenge.
In this study, we validate the Arabic version of the
functional Autonomy measurement system for the
result, we have carried this study through two stages. In
stage one, we distributed the Arabic version of FAMS to
nineteen Arabic health professionals in rehab rehabili-
tation team. They were satis ed about it but they have
some comments regarding the sentence structure. Based
on their comments we modi ed the Arabic version to be
Table 1. mean of elderly age
Statistics
age
N Valid 30
Missing 0
Mean 71.6667
Table 2. number of male and female who are participate in research.
gender
Frequency Percent Valid Percent Cumulative Percent
male
Valid female
Total
9 30.0 30.0 30.0
21 70.0 70.0 100.0
30 100.0 100.0
Albandary Alhadlaq et al.
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS CROSS CULTURAL VALIDATION OF FUNCTIONAL AUTONOMY MEASUREMENT SYSTEM 553
Table 3: shows the value of cronbach’s alpha for ADL, Mobility, Communication, Mental function, IADL.
Item-Total Statistics
Scale Mean
if Item
Deleted
Scale Variance
if Item Deleted
Corrected Item-
Total Correlation
Squared
Multiple
Correlation
Cronbach’s
Alpha if Item
Deleted
activities_of_daily_living_eating 93.6667 929.333 .699 . .915
activities_of_daily_living_bathing 93.6000 916.938 .835 . .914
activities_of_daily_living_dressing 93.6667 922.368 .851 . .914
activities_of_daily_living_grooming 93.7000 916.631 .886 . .913
activities_of_daily_living_urinary_
function
93.9333 935.237 .767 . .915
activities_of_daily_living_bowel_
function
94.1000 954.231 .631 . .917
activities_of_daily_living_toiletting 93.9000 941.610 .604 . .916
Mobility_TRANSFERS 93.8333 934.144 .756 . .915
Mobility_WALKING_INSIDE 93.6667 927.540 .678 . .915
Mobility_PROPELLING_A_
WHEELCHAIR_INSIDE
93.9000 931.059 .760 . .915
Mobility_NEGOTIATING_STAIRS 92.9667 900.930 .810 . .913
Mobiliy_MOVING_AROUND_
OUTSIDE
93.2333 901.151 .760 . .913
communication_vision 93.8667 962.051 .578 . .918
comunication_hearing 94.1333 966.602 .603 . .918
communication_speaking 94.2000 969.407 .569 . .919
mental_function_memory 93.8667 957.844 .687 . .917
mental_function_orientation 94.0667 952.685 .808 . .917
mental_function_COMPREHENSION
94.1333 962.740 .733 . .918
mental_function_JUDGMENT 93.9000 941.128 .749 . .916
mental_function_BEHAVIOUR 94.0333 968.723 .553 . .919
INSTRUMENTAL_ACTIVITIES_OF_
DAILY_LIVING_HOUSEKEEPING
93.0000 898.897 .812 . .913
INSTRUMENTAL_ACTIVITIES_
OF_DAILY_LIVING_MEAL_
PREPARATION
92.6000 902.041 .755 . .913
INSTRUMENTAL_ACTIVITIES_OF_
DAILY_LIVING_SHOPPING
93.0333 894.378 .829 . .912
INSTRUMENTAL_ACTIVITIES_OF_
DAILY_LIVING_LAUNDRY
92.7333 894.616 .769 . .913
INSTRUMENTAL_ACTIVITIES_OF_
DAILY_LIVING_TELEPHONE
93.1667 912.833 .835 . .913
INSTRUMENTAL_ACTIVITIES_OF_
DAILY_LIVING_TRANSPORTATION
93.1667 906.695 .894 . .913
INSTRUMENTAL_ACTIVITIES_OF_
DAILY_LIVING_MEDICATION_USE
93.2333 906.875 .805 . .913
INSTRUMENTAL_ACTIVITIES_OF_
DAILY_LIVING_BUDGETING
93.0667 898.133 .803 . .913
Albandary Alhadlaq et al.
554 CROSS CULTURAL VALIDATION OF FUNCTIONAL AUTONOMY MEASUREMENT SYSTEM BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
more suitable Setubal and understandable for the Arabic
speakers. The second stage, we distributed the modi ed
Arabic version to 30 individuals from a representative
elderly group. They were able to understand and answer
all the questions with no dif culty and help.
This study considered to be the rst study that
validate FAMS to Arabic culture, which is one of the
strength of this cross-sectional study. Another strength
of this study, is that by now this version of FAMS is
available to be used by all Arabic countries with differ-
ent dialects. However, this study have some weakness.
Although, the validation of FAMS into Arabic version
has been completed, the sample size was small. Despite
that we try to make it representative for older people
living in Saudi Arabia in term of social-economic sta-
tus, ethnicity, level of education, age, and health status.
Thus, future research is needed to increase the sample
size and better sampling technique in order to obtain
valid information and to recheck our validity. The inter-
nal consistency for the study is 0.9 which consider a
high consistency. In a study carried out by Desrosiers,
et al., (1995) they used test re-test to measure the intra-
class correlation reliability. While, in our study we used
the Cronbach’s alpha to measure the reliability, despite
this the nding from previous study were similar to the
present study (Desrosiers et al, 1995). In terms of ADL
our present study was in agreement with Desrosiers,
et al (1995) study. For the mobility part, present study
was also in line with both Desrosiers et al. (1995) study
and Desrosiers et al. (2004) study (Desrosiers et al, 1995;
Desrosiers, et al, 2004).
However, for communication part, our study was in
line with Desrosiers, et al. (1995); but was not in agree-
ment with Desrosiers, et al (2004). The possible explana-
tion could be because the 2004 study internal consist-
ency for this part was different from our study which
was range from 0.3 to 0.4 the same as the mental func-
tion. For IADL, our study In line with Desrosiers et al.
(1995) study and Desrosiers et al. (2004) study (Desro-
siers et al, 2004).
By using Cronbach’s alpha, the reliabil-
ity and validity of the Arabic FAMS was measured. The
internal consistency is used to measure the reliability.
Therefore, we found that the Arabic version of FAMS
is valid to be used in Arabic culture. However, further
study to implement SMAF as measurement tools in Arab
culture elderly will strengthen the tools and increase its
reliability.
CONCLUSION
This research revealed that it is possible to validate west-
ern based rehabilitation tool into Arabic culture in order
to use reliable measure. The new Arabic SMAF version is
valid and reliable measure and culturally adapted tool to
test ability of elderly people in Saudi Arabia and widely
in Arab population. For the rst time ever we introduced
rehabilitation specialists with new tool appropriate for
Arab culture and resources.
REFERENCES
Amini, D. A., Kannenberg, K., Bodison, S., Chang, P., Colaianni,
D., Goodrich, B., & Lieberman, D. (2014). Occupational therapy
practice framework: Domain & process 3rd edition.American
Journal of Occupational Therapy,68, S1-S48.
Beaton, D. E., Bombardier, C., Guillemin, F., & Ferraz, M.
B. (2000). Guidelines for the process of cross-cultural adapta-
tion of self-report measures. Spine, 25(24), 3186-3191.
DESROSIERS, J., BRAVO, G., HÉBERT, R., & DUBUC, N.
(1995). Reliability of the revised functional autonomy meas-
urement system (SMAF) for epidemiological research. Age and
ageing, 24(5), 402-406.
Desrosiers, J., Noreau, L., Robichaud, L., Fougeyrollas, P.,
Rochette, A., & Viscogliosi, C. (2004). Validity of the
assessment of life habits in older adults. Journal of Rehabilita-
tion Medicine, 36(4), 177-182.
Elboim-Gabyzon, M., Agmon, M., Azaiza, F., & Laufer, Y.
(2015). Translation and validation of the Arab version of the
Late-Life Function and Disability Instrument: a cross sectional
study.BMC geriatrics,15(1), 51.
Ferraz, M. B. (1997). Cross cultural adaptation of question-
naires: what is it and when should it be performed? The Jour-
nal of rheumatology, 24(11), 2066.
Guillemin, F. (1995). Cross-cultural adaptation and validation
of health status measures. Scandinavian journal of rheumatol-
ogy, 24(2), 61-63.
Hébert, R., Carrier, R., & Bilodeau, A. (1988). The Functional
Autonomy Measurement System (SMAF): description and
validation of an instrument for the measurement of handi-
caps.Age and ageing,17(5), 293-302.
Hébert, R. (1997). Functional decline in old age. Canadian
Medical Association Journal, 157(8), 1037-1045
Hébert, R., Brayne, C., & Spiegelhalter, D. (1999). Factors
associated with functional decline and improvement in a very
elderly community-dwelling population.American Journal of
Epidemiology,150(5), 501-510.
Hébert, R., Guilbault, J., Desrosiers, J., & Dubuc, N. (2001). The
functional autonomy measurement system (SMAF): a clinical-
based instrument for measuring disabilities and handicaps in
older people.Geriatrics Today,4, 141-158.
Hébert, R., Robichaud, L., Roy, P. M., Bravo, G., & Voyer, L.
(2001). Ef cacy of a nurse‐led multidimensional preventive
programme for older people at risk of functional decline. A
randomized controlled trial. Age and Ageing, 30(2), 147-
153.
Hébert, R., Durand, P. J., Dubuc, N., & Tourigny, A. (2003).
PRISMA: a new model of integrated service delivery for the
frail older people in Canada. International journal of inte-
grated care, 3(1).

Albandary Alhadlaq et al.
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS CROSS CULTURAL VALIDATION OF FUNCTIONAL AUTONOMY MEASUREMENT SYSTEM 555
Hébert, R., Raîche, M., Dubois, M. F., Gueye, N. D. R., Dubuc,
N., Tousignant, M., & PRISMA Group. (2009). Impact of
PRISMA, a coordination-type integrated service delivery sys-
tem for frail older people in Quebec (Canada): A quasi-experi-
mental study.Journals of Gerontology Series B: Psychological
Sciences and Social Sciences,65(1), 107-118.
Kimberlin, C. L., & Winterstein, A. G. (2008). Validity and
reliability of measurement instruments used in research.
American Journal of Health-System Pharmacy, 65(23), 2276-
2284.
Mercier, L., Audet, T., Hébert, R., Rochette, A., & Dubois,
M. F. (2001). Impact of motor, cognitive, and perceptual dis-
orders on ability to perform activities of daily living after
stroke.Stroke,32(11), 2602-2608.
Pinsonnault, E., Desrosiers, J., Dubuc, N., Kalfat, H., Colvez, A.,
& Delli-Colli, N. (2003). Functional autonomy measure-
ment system: development of a social subscale. Archives of
gerontology and geriatrics,37(3), 223-233.
Riyadh. (2016). Retrieved from http://ngha.med.sa/English/
MedicalCities/AlRiyadh/Pages/default.aspx
Tousignant, M., Hébert, R., Dubuc, N., Simoneau, F., &
Dieleman, L. (2003). Applicationnof a case‐mix classi cation
based on the functional autonomy of the residents for funding
long‐term care facilities. Age and ageing, 32(1), 60-66.
Tousignant, M., Hébert, R., Desrosiers, J., & Hollander, M.
J. (2003). Economic evaluation of a geriatric day hospital: cost‐
bene t analysis based on functional autonomy changes.Age
and Ageing,32(1), 53-59.