
Medical
Communication
Biosci. Biotech. Res. Comm. 11(2): 285-290 (2018)
The accelerating epidemic of type-2 diabetes in
children and adolescents
Manju Dewan
Post Graduate Department of Zoology, DAV College, Sector 10, Chandigarh
ABSTRACT
The occurrence of type- 2 diabetes in youth has increased dramatically over the past 20 years. Adolescents and young
adults are fastly entering into the domain of the disease. The emergence of type 2 diabetes mellitus in children in
Indian population presents a new challenge. 2048 children had undergone questionnaire and dietary survey and
health examination. The scrutiny of the subjects for blood sugar levels along with various other parameters involved
in this study revealed that 1.12% subjects were diabetics as compared to 1.56% with impaired glucose level. This
shows a total ignorance on the part of parents about their children’s’ health status.The study brought forth a hard
fact that periodic health checkup is necessary to prevent the agony of this disease. It is further pointed out that such
surveys are very rare particularly in the underdeveloped and developing countries. It is worthwhile to conduct sur-
veys to detect such cases so that timely remedy can be provided.
KEY WORDS: TYPE 2 DIABETES, CHILDREN, ADOLESCENTS, HEALTH, DISEASE
285
ARTICLE INFORMATION:
*Corresponding Author: manjudewan72@gmail.com
Received 21
st
March, 2018
Accepted after revision 12
th
June, 2018
BBRC Print ISSN: 0974-6455
Online ISSN: 2321-4007 CODEN: USA BBRCBA
Thomson Reuters ISI ESC / Clarivate Analytics USA and
Crossref Indexed Journal
NAAS Journal Score 2018: 4.31 SJIF 2017: 4.196
© A Society of Science and Nature Publication, Bhopal India
2018. All rights reserved.
Online Contents Available at: http//www.bbrc.in/
DOI: 10.21786/bbrc/11.1/14
INTRODUCTION
Type 2 diabetes is rising rapidly amongst children and
adolescents worldwide. The incidence of type 2 diabe-
tes in youth has increased dramatically over the past
20 years. Type-2 diabetes is a signi cant and increasing
burden in adolescents and young adults. Overweight is,
at present, the most common health problem faced by
the children in both develop and developing countries
which leads to the development of Type-2 diabetes (Han
et al., 2010). This has been attributed to the fact, that the
prevalence of obesity is not increasing but the degree
of obesity also increases in affected children and ado-
lescents (May et al., 2012). Type-2 diabetes mellitus is a
complex metabolic disorder of heterogeneous etiology
with social, behavioral, and environmental risk factors
286 THE ACCELERATING EPIDEMIC OF TYPE-2 DIABETES IN CHILDREN AND ADOLESCENTS BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
Manju Dewan et al.
unmasking the effects of genetic susceptibility (Kiess,
2003). Clear strategies for research, prevention and treat-
ment of the disease in these vulnerable patients are the
need of the hour. Understanding the unique pathophysi-
ology of type-2 diabetes in youth, as well as the risk of
complications and the psychosocial impact, will enable
industry, academia, funding agencies, advocacy groups
and regulators to collectively evaluate both current and
future research, treatment and prevention approaches.
Type-2 diabetes mellitus is still rare in childhood and
adolescence, but recent reports indicate an increasing
prevalence around the world possibly due to increas-
ing prevalence of obesity in children and adolescents
(Thomas, 2013, Kristen et al, 2016).
MATERIALS AND METHODS
2048 children had undergone questionnaire and dietary
survey and health examination. Out of these, 1017 were
from urban population and 1031 from rural population.
Children and adolescents aged 10-19 years were selected
randomly for questioning regarding the different aspects
of epidemiology and their health examination was done.
The permission from parents of the children, undergoing
examination and questionnaire survey was also taken
on the self-designed consent form. The Centers for Dis-
ease Control and Prevention (CDC) suggests two levels
of concern for children based on the BMI-for-age charts.
At the 85th percentile and above, children are “at risk
for overweight”. At the 95th percentile or above, they
are “overweight”. The cutoff for underweight of less than
the 5th percentile is based on recommendations by the
World Health Organization Expert Committee on Physi-
cal Status 1998. The diagnostic criteria for diabetes mel-
litus have been modi ed from those previously recom-
mended by WHO (1985). The revised criteria of report
of the Expert Committee on the Diagnosis and Classi-
cation of Diabetes Mellitus (2003) for the diagnosis of
diabetes was used.
RESULTS AND DISCUSSION
The emergence of type-2 diabetes mellitus in children in
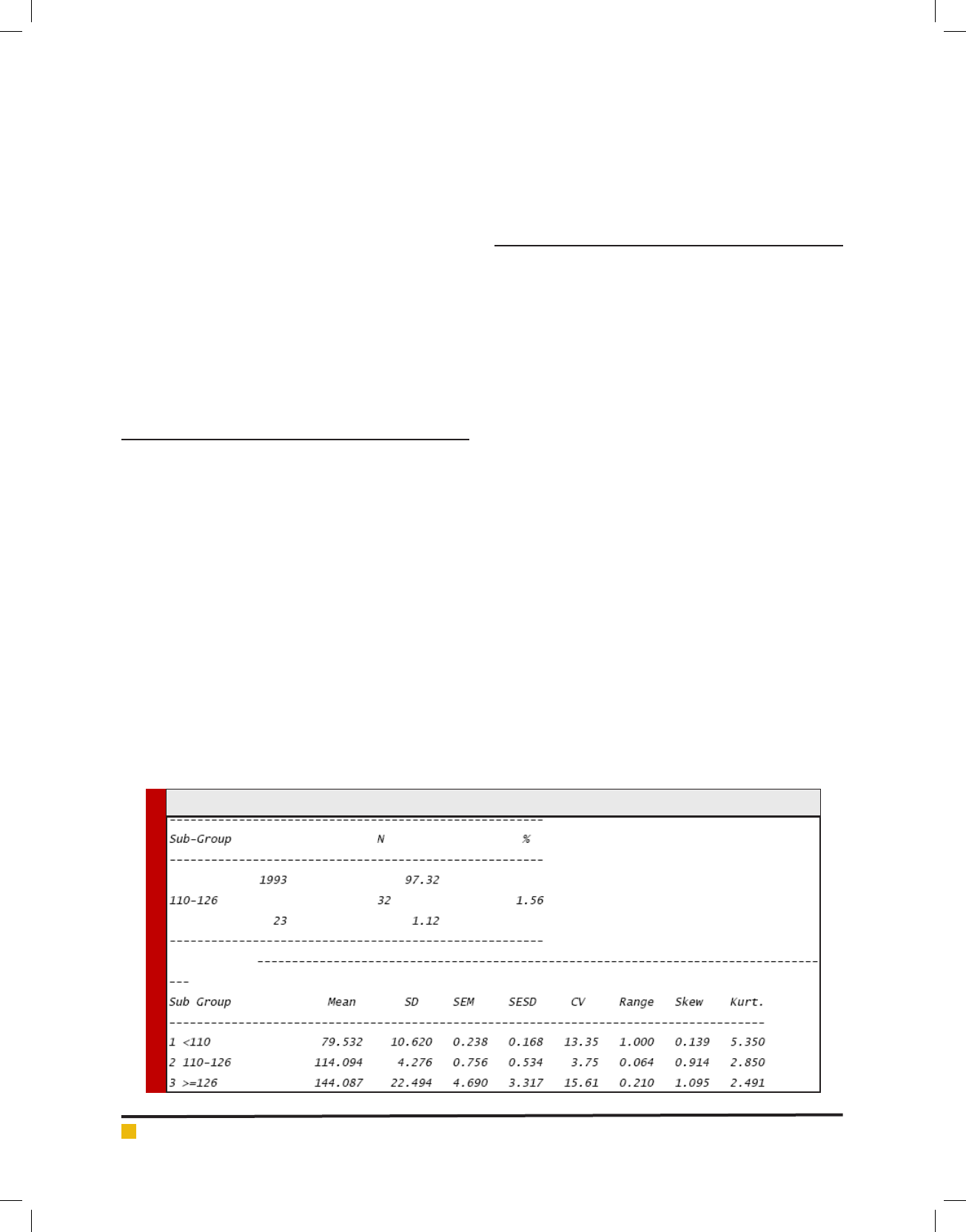
Indian population presents a new challenge. The scru-
tiny of the subjects for blood sugar levels along with
various other parameters involved in this study revealed
that 1.12% subjects were diabetics as compared to 1.56%
with impaired glucose level from the already mentioned
area. Such children, along with impaired glucose level
and diabetic cases were totally ignorant about their
health status viz a viz this disease.
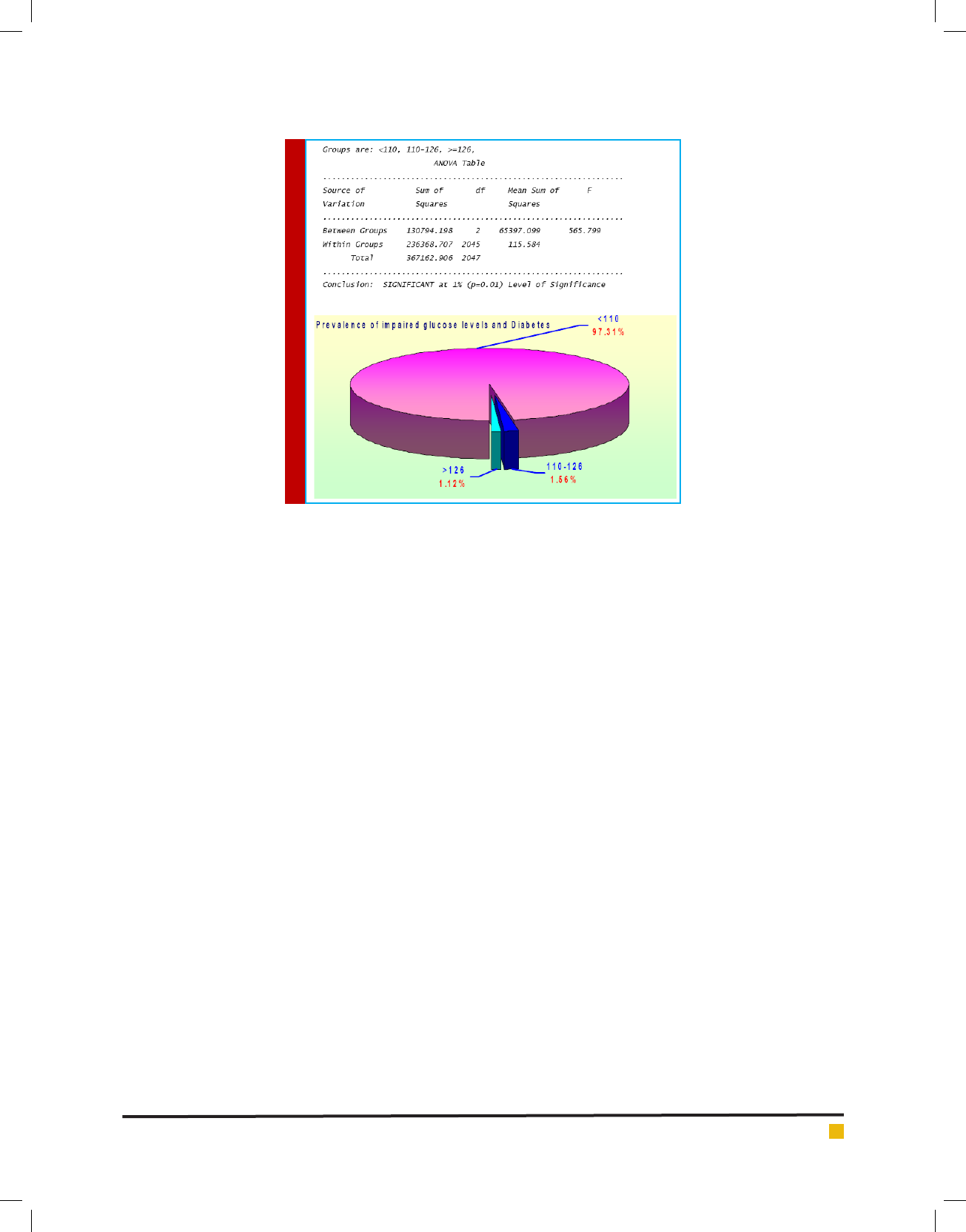
Analysis of Variance (ANOVA)
By subjecting the various observations to statistical
analysis, certain factors became quite apparent when
comparisons between normal subjects and those having
different status of diabetes mellitus were made. When
all inter-group comparisons were attempted in order to
obtain a clear picture of the status of children among
themselves, signi cant results have been obtained.
The observations given above embodied quite reveal-
ing information from 2048 subjects studied. This shows
a total ignorance on the part of parents about their chil-
drens’ health status. The study brought forth the fact
that periodic health checkup is necessary to avoid the
agony of this disease. It is further pointed out that such
surveys are very rare particularly in the underdeveloped
and developing countries. It is worthwhile to conduct
surveys to detect such cases so that timely help can be
provided. The present work is the rst of this nature
from Chandigarh in Northern India.
Table 9. Prevalence of impaired glucose levels and diabetes in total population
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS THE ACCELERATING EPIDEMIC OF TYPE-2 DIABETES IN CHILDREN AND ADOLESCENTS 287
Manju Dewan et al.
In India, the incidence of diabetes mellitus is increas-
ing because of intake of high carbohydrate rich food
by the children and adolescents. It is therefore neces-
sary to make the general population aware about their
health status by conducting periodic health checkups.
Such incidents are not restricted to Punjab or other parts
of India but are global. It had been noticed that half of
the 16 million Americans with diabetes are undiagnosed
as had been studied by Harris et al., 1987, Harris, 1993,
U.S. Department of Health and Human Services, 1993.
Four million Americans with known diagnosis of dia-
betes are hospitalized annually in this country (Levetan
et al., 1998). In the U.S., estimates are as high as 5,000
new cases are added per year (Lawrence et al, 2014).
Prevalence increases with age, tripling from age
10–14 years to 15–18 years (Dabeleaet al, 2014). Diag-
nosis of type-2 diabetes is estimated to be delayed by
an average of 10 years after the actual onset of disease.
The present study corroborate very well with this obser-
vation as 1.56% subjects are having impaired glucose
levels which are likely to become diabetics and 1.12%
subjects were diabetics. In fact, this group is one which
needs an immediate attention of the subject himself,
parents and the health authorities. An early study in
1991 of rural areas in Delhi indicated that the prevalence
rate for type-2 diabetes ranged from 0.4-1.5% (Ahuja
et al. 1991).
This study had not included impaired glucose levels
and subjects were only from rural area. Data regard-
ing type-2 diabetes in children and adolescents is very
scarce in this area. Over the last decade, it has become
apparent that type-2 diabetes extends its wings not
only into the young adult population but is also found
in adolescents and even, occasionally, in children. The
limited data, that is currently available, present a rather
uncertain picture, with a rather wide range of preva-
lence and incidences of type 2 diabetes in children and
adolescents. The transition from prediabetes to type-2
diabetes in adults is usually a gradual phenomenon that
occurs over 5–10 years (Weiss et al, 2005). Therefore,
the early presentation of type-2 diabetes in youth raises
the possibility of an accelerated process in pediatric age
compared with adults, thus shortening the transition
time between IGT and type-2 diabetes. In fact, an inter-
esting report by Gungor and Arslanian (2004) suggested
that despite a relatively robust initial insulin secretion,
the deterioration in -cell function in youth with type-2
diabetes is more accelerated than that was observed in
adults.
Type-2 diabetes mellitus was reported in children
and adolescents from the United States, Canada, Japan,
Hong Kong, Singapore, Bangladesh, Libya, the United
Kingdom, Australia and New Zealand. The prevalence
of type-2 diabetes in children and adolescents ranges
from 4.1 per 1000 amongst 12-19 year olds in the United
States to 50.9 per 1000 15-19 year old Pima Indians in
Arizona. Between 8% and 45% of recently diagnosed
cases of diabetes in children and adolescents in the
United States were type-2 diabetics (Fagot et al, 2000
and 2001). The emergence of type-2 diabetes coincides
with worldwide trends of rising prevalence in over-
weight and sedentary lifestyle (Troiano et al 1995).
India is poised to be among the world’s top four
economies by 2020 (Abdul Kalam, 1998) and is under-

Manju Dewan et al.
288 THE ACCELERATING EPIDEMIC OF TYPE-2 DIABETES IN CHILDREN AND ADOLESCENTS BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
going a rapid epidemiological transition: the burden
of chronic diseases is overtaking the burden of infec-
tious diseases (Fall and Barker, 1995, and Nath et al,
1998). India already has the highest number of adult
diabetes cases (20 million) worldwide and this number is
expected to rise to 57 million by 2020 (King et al, 1998
and Narayan et al, 2000). There is only few data avail-
able on type-2 diabetes in children and adolescents in
India. The prevalence of obesity (body mass index [BMI]
exceeding the 95th percentile) among US children and
adolescents aged 6−19 years has jumped from approxi-
mately 4% in 1963 to 15% in 2000. In some regions in
the United States, type 2 diabetes mellitus is as frequent
as type-1 diabetes mellitus in adolescents (Arslanian,
2002 and Zeitler, 2015).
Rapid urbanization and economic growth creates
social dynamics that promote diabetes risk factors.
These include over-weight, decrease in physical activity,
increase in sedentary activities such as television view-
ing, and high fat and high-energy diet among adults and
children. Other factors may also make Indian children
and young adults more vulnerable to diabetes. These
include prenatal factors (e.g., low birth weight, maternal
under-nutrition), biological propensity to central obesity
and insulin resistance, low lean mass, diabetes during
pregnancy, impaired glucose tolerance, and urban stress
(Ramachandran et al 1992, 1994, 1997, 1999 and Yajnik
2001).
Type-2 diabetes in children is being increasingly
reported from other Asian countries. In Japan, the inci-
dence of type-2 diabetes in children increased over a
20-year period (6-12 years: 0.2/100,000/year in 1976 and
2.0/100,000/year in 1995; 12-15 years: 7.3/100,000/year
in 1976 and 13.9/100,000/year in 1995. This increase
in incidence correlated with increased reported intake
of animal protein and fat( Kitagawa ,1998 and Fagot
et al 2000). Type-2 diabetes is being reported in children
of Indian origin living in countries such as the United
Kingdom (Ehtisham et al 2000). There is an urban-rural
gradient in adult diabetes risk in India and when the
data are standardized for age and sex differences, the
prevalence of diabetes in urban Indians is similar to that
of Indians abroad (Ramachandran et al, 1997). This nd-
ing suggests that type-2 diabetes in children of Indian
origin living abroad may be an early indication of things
to come to India.
The biggest challenge India is likely to face in the
future is tackling diabetes among children and adoles-
cents. The number of children falling prey to type-2 dia-
betes has increased manifold over the past two decades.
Rapid urbanization and economic growth have pro-
moted risk factors for diabetes such as obesity, sedentary
lifestyle, high fat and high energy diet among adults and
children. Unfortunately, no systematic survey has been
conducted so far to know the trends in India. Untreated
children and adolescents with type-2 diabetes are at
much higher risk of cardiovascular disease, kidney fail-
ure and vision loss. New health initiatives targeting chil-
dren and adolescents which are aimed to raise awareness
and check the rapidly increasing cases of obesity and
diabetes.
Type-2 diabetes in children is probably under-diag-
nosed because it can exist without symptoms. It may
also be under-reported and part of the reason for this
may be misclassi cation (Fagot et al, 2000, 2001 and
American Diabetes Association 2000)). The prevalence
of childhood diabetes among those younger than 15
years in the early 1990s in an urban population in south
India was 0.26/1000 (Ramachandran 1992) and the inci-
dence was 10.5/100,000/year. There are two important
implications of the potential emergence of type-2 dia-
betes in children in India. Obesity and type-2 diabetes
in children may be at the epicenter of a much larger
diabetes epidemic in India than currently predicted and
compulsion to act against the potential diabetes epi-
demic in an organized and systematic manner. Most of
the children having impaired glucose levels and diabetes
were ignorant about their status at the time of diagnosis.
The thrifty genotype hypothesis was advanced over
40 years ago
to explain the modern emergence of obe-
sity and type-2 diabetes
(Neel, 1962). This hypothesis
postulates that humans survived by the
genetic selection
of those whose metabolic storage capabilities
permitted
survival during periods of famine by taking advantage
of episodic periods of plenty in a feast and famine exist-
ence.
Continuous feasting with an abundance of calorie-
rich foods
results in fat deposition without the concomi-
tant period of
fasting to maintain a normal body weight.
Historically, only
the prosperous met this condition, but
modern food production
and marketing have led to low-
cost abundance, with obesity now
disproportionately
affecting those at the less prosperous end
of the eco-
nomic scale.
Perhaps the most important reason for increasing
prevalence of diabetes, obesity and type-2 diabetes is
the rapidly changing imbalanced dietary habits, both
in rural and urban areas, due to several factors–easy
availability of convenience foods, frequent snacking on
energy dense fast foods, high consumption of packaged
food in place of traditional home made food, etc. This
transition has resulted in excess consumption of calo-
ries, saturated fats, trans fatty acids, simple sugars, salt
and a low ber intake. It is high time to prepare to com-
bat this menace and curb its spread. Indians are geneti-
cally more prone to diabetes. On top of this, a rapid shift
in our dietary habits and life styles is resulting in a rapid
rise in obesity, diabetes, metabolic syndrome and heart
disease. Hence, a proper and healthy diet remains the

Manju Dewan et al.
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS THE ACCELERATING EPIDEMIC OF TYPE-2 DIABETES IN CHILDREN AND ADOLESCENTS 289
keystone for the prevention and management of type-2
diabetes.
ACKNOWLEDGEMENT
The author is highly thankful to UGC for providing grant
for undertaking the research award.
REFERENCES
Abdul Kalam APJ, Rajan YS. India 2020: A vision for the New
Millenium. New Delhi, Penguin Books, 1998.
Ahuja MMS. Recent contributions to the epidemiology of dia-
betes mellitus in India. International Journal of Diabetes in
Developing Countries, 1991, 11:5–9.
American Diabetes Association: Type 2 Diabetes in children
and adolescents. Pediatrics 2000; 105:671–680.
Arslanian SA. Type 2 diabetes mellitus in children: pathophys-
iology and risk factors.J Pediatr Endocrinol Metab.2000;13
Suppl 6:1385–1394.
Center for Disease Control (CDC). Body mass Index: BMI for
children and teens.2000.apps.nccd.cdc.gov/dnpabmi.
Centers for Disease Control and Prevention: National Diabe-
tes Fact Sheet: General Information and National Estimates on
Diabetes in the United States, 2003.Rev.ed.
Dabelea D,Mayer-Davis EJ, Saydah S, et al.; SEARCH for
Diabetes in Youth Study Prevalence of type 1 and type
2 diabetes among children and adolescents from 2001 to
2009.JAMA2014;311:1778–1786.
Ehtisham S, Barrett TG, Shaw NJ. Type 2 diabetes mellitus in
UK children: an emerging problem. Diabetic medicine, 2000,
17:867–71.
Fagot-Campagna A, Narayan KMV, Imperatore G. Type 2 dia-
betes in children: Exempli es the growing problem of chronic
diseases. BMJ 2001; 322: 377-378.
Fagot-Campagna A, Petitt DJ, Engelgau MM, Burrows NR,
Geiss LS, Valdez R, Beckles GLA, Saaddine J, Gregg W, Wil-
liamson DF, Narayan V: Type 2 diabetes among North Ameri-
can children and adolescents: an epidemiologic review and a
public health perspective. J Pediatr 2000;136:664 -672.
Fagot-Campagna A, Pettitt DJ, Engelgau MM, Rios Burrows N,
Geiss LS, Valdez R, et al. Type 2 diabetes among North Ameri-
can children and adolescents: An epidemiological review and a
public health perspective. J Pediatr 2000; 136: 664-672.
Fagot-Campagna A, Saaddine JB, Flegal KM & Beckles GL.
Diabetes, impaired fasting glucose, and elevated HbA1c in US
adolescents: the Third National Health and Nutrition Examina-
tion Survey. Diabetes Care 2001 ; 24 834–837.
Fall CHD, Barker DJP. The fetal origins of coronary heart dis-
ease and non-insulin dependent diabetes in India. Indian Pedi-
atr 1997; 34: 5-8.
GungorN,ArslanianS.Progressive beta cell failure in type 2
diabetes mellitus of youth.J Pediatr2004;44:656–659.
Han JC, Lawlor DA, Kimm SY. Childhood obesity. Lan-
cet.2010;375:1737–1748
Harris, M.I. Undiagnosed NIDDM: Clinical a not public health
issue. Diabetes Care, 1993; 16: 642-652.
Harris, M.I., Hadden, W.C., Knowler, W.C. and Bennett, P.H.
Prevalence of diabetes and impaired glucose tolerance and
plasma glucose levels in U.S. Population aged 20-74 years.
Diabetes, 1987; 36: 523-534.
Kiess W, Böttner A, Raile K, Kapellen T, Müller G, Galler A,
Paschke R, Wabitsch M. Type 2 diabetes mellitus in children
and adolescents: a review from a European perspective.Horm
Res.2003;59 Suppl 1:77–84.
King H, Aubert RE, Herman WH. Global burden of diabetes,
1995-2025: Prevalence, numerical estimation, and projections.
Diabetes Care 1998; 21: 1414-1431.
Kitagawa T, Owada M, Urakami T, Yamauchi K. Increased
incidence of non-insulin dependent diabetes mellitus among
Japanese school children correlates with an increased intake of
animal protein and fat. Clin Pediatr 1998; 37: 111-115.
Kristen J. Nadeau, Barbara J. Anderson, Erika G. Berg, Jane
L. Chiang,Hubert Chou,Kenneth C. opeland,Tamara S. Han-
non,Terry T.-K. Huang,Jane L. Lynch,Jeff Powell,Elizabeth
Sellers,William V. TamborlaneandPhilip Zeitler . Youth-Onset
Type 2 Diabetes Consensus Report: Current Status, Challenges,
and PrioritiesDiabetes Care2016 Sep;39(9):1635-642.https://doi.
org/10.2337/dc16-1066
LawrenceJM,ImperatoreG,PettittDJ,et al.Incidence of diabe-
tes in United States youth by diabetes type, race/ethnicity, and
age, 2008–2009 (Abstract). Diabetes2014;63(Suppl. 1):A407
Levetan, S. Claresa, Passaro Maureen, Jablonski Kathleen, Kass
Mary, Ratner E. Robert Unrecognized Diabetes among hospi-
talized patients. Diabetes Care, 1998.; 21 (2) : 246-249.
May AL, Kuklina EV, Yoon PW. Prevalence of cardiovascular
disease risk factors among US adolescents, 1999-2008.Pediat-
rics.2012;129:1035–1041.
Narayan KMV, Gregg EW, Fagot-Campagna A, Engelgau MM,
Vinicor F. Diabetes – A common, serious, costly, and poten-
tially preventable public health problem. Diabetes Res Clin
Pract 2000; 50 (Suppl 2): 77-84.
Nath I, Reddy KS, Dinshaw KA, Bhisey AN, Krishnaswami
K, Bhan MK, et al. Country pro le: India. Lancet 1998; 351:
1265-1275.
Neel, J.V. Diabetes Mellitus: a thrifty genotype rendered detri-
mental by progress ? Am. J. Genet., 1962;14 : 353-362.
Ramachandran A, Snehalatha C, Abdul Khader OMS, Joseph
TA, Viswanathan M. Prevalence of childhood diabetes in an
urban population in south India. Diabetes Res Clin Pract 1992;
17: 227-231.
Ramachandran A, Snehalatha C, Latha E, Vijay V, Viswana-
than M: Rising prevalence of NIDDM in urban population in
India. Diabetologia 1997; 40:232–237.
Ramachandran A, Snehalatha C, Satyavani K, Sivasankari S,
Vijay V: GAD65 antibodies in classi cation of Asian Indian

Manju Dewan et al.
290 THE ACCELERATING EPIDEMIC OF TYPE-2 DIABETES IN CHILDREN AND ADOLESCENTS BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
diabetic subjects with onset between 20 and 40 years. Diabetes
Care 1999; 22:175–176.
Ramachandran A, Snehalatha C, Shyamala P, Vijay V, Viswa-
nathan M. Prevalence of diabetes in pregnant women – A study
from southern India. Diabetes Res Clin Pract 1994; 25: 71-
74.
The Expert Committee on the Diagnosis and Classi cation
of Diabetes Mellitus from the American Diabetes Association,
Alexandria, Virginia Diabetes Care 2003; 26:S5-S20,
Thomas Reinehr. Type 2 diabetes mellitus in children and ado-
lescentsWorld J Diabetes. 2013 ; 4(6): 270–281.
Troiano RP, Flegal KM, Kuczmarski RJ, Campbell SM, John-
son CL. Overweight prevalence and trends for children and
adolescents. The National Health and Nutrition Examination
Surveys, 1963 to 1991. Arch Pediatr Adolesc Med 1995; 149:
1085-1091.
U.S. Department of Health and Human Services: Diabetes in
the United States : A strategy for prevention. U.S. department
of health and human services, Public Health Service Centres
for disease control and National Center for chronic disease pre-
vention and Health promotion. Divisoin of Diabetes Transla-
tion, 1993.
WeissR,TaksaliSE,TamborlaneWV, BurgertTS,SavoyeM,Cap-
rioS. Predictors of changes in glucose tolerance status in obese
youth.Diabetes Care 2005; 28:902–909 pmid:15793193
World Health Organization Study Group on Diabetes Mellitus
Technical Report Series, 727, WHO Geneva,1985.
World Health Organization.Obesity: preventing and managing
the global epidemic. Report of a WHO consultation on Obesity,
Geneva, 3–5, June 1997. World Health Organization: Geneva;
1998.
Yajnik CS. The insulin resistance epidemic in India: Fetal ori-
gins, later lifestyle, or both? Nutr Rev 2001; 59: 1-9.
ZeitlerP,ChouHS,CopelandKC,GeffnerM.Clinical trials in
youth-onset type 2 diabetes: needs, barriers, and options.Curr
Diab Rep2015;15:28.