
Health Science
Communication
Biosci. Biotech. Res. Comm. 10(1): 114-120 (2017)
Relationship between health literacy and health
promoting behavior in patients with heart failure
referred to clinics of Shahid Beheshti University of
Medical Sciences
Mahrokh Imanian
1
, Meimanat Hosseini
2
*, Tahereh Ashk Torab
3
, Nezhat Shakeri
4
and
Mahsa Matbouei
5
1
Department of Medical Surgical Nursing, Student’s Research Of ce, Shahid Beheshti University of Medical
Sciences, Tehran, Iran
2
PhD in Nursing, Assistant Professor of Community Health Nursing Department, School of Nursing and
Midwifery, Shahid Beheshti University of Medical Sciences, Tehran, Iran
3
PhD in Nursing, Assistant Professor of Nursing Department, School of Nursing and Midwifery, Shahid
Beheshti University of Medical Sciences, Tehran, Iran
4
PhD in Biostatistics, Department of Biostatistics, Faculty of Paramedical Sciences, Shahid Beheshti
University of Medical Sciences, Tehran, Iran
5
Instructor of Nursing (MSc), Dept.of Community Health Nursing, School of Nursing & Midwifery Shahid
Beheshti University of Medical Sciences, Tehran, Iran
ABSTRACT
Patients with heart failure are considered one of the most important groups exposed to the danger of low health
literacy that may affect their health-promotion behaviors and quality of life and increase the load of health-related
costs. Therefore, the present study aimed to determine the relationship between health literacy and health-promoting
behaviors in patients with heart failurewho referred to heart clinics of Shahid Beheshti University of Medical Sci-
ences.This correlational study was conducted on 300 heart failure patients, selected byrandom cluster sampling
method with proportional allocation. Data collection tool was demographic information questionnaire,Health literacy
measurement and Health promoting Lifestyle Pro le 2 (HPLP2). Data analysis was performed using SPSS software
version 19 though statistical tests, includingindependent t-test, Pearson and Spearman correlation coef cient, Mann-
114
ARTICLE INFORMATION:
*Corresponding Author: m_hoseini@sbm
Received 27
th
Nov, 2016
Accepted after revision 12
th
March, 2017
BBRC Print ISSN: 0974-6455
Online ISSN: 2321-4007 CODEN: USA BBRCBA
Thomson Reuters ISI ESC and Crossref Indexed Journal
NAAS Journal Score 2017: 4.31 Cosmos IF : 4.006
© A Society of Science and Nature Publication, 2017. All rights
reserved.
Online Contents Available at: http//www.bbrc.in/

Mahrokh Imanian et al.
Whitney-U test and Kruskal-Wallis. The results showed that mean and standard deviation (SD) score ofhealth literacy
of participants was 3.29±0.6 and meanand SD score of health-promoting behaviors was 2.42±0.29. The Pearson
correlation coef cientshoweddirect and signi cant relationship between health literacy andhealth-promoting behav-
iors (r=0.66, P<0.001). The results of this research showed the statistically signi cant relationship between health
literacy level and health-promoting behavior. Therefore, health literacy should be paid special attention, as a factor
affectinghealth-promoting behaviors,healthy life style and quality of life. According to the results of this study, pro-
grammingeducation and development of health-promoting behaviorsin patients with heart failure suggest that the
health literacy needsmore attention inhealth-promotion plans.
KEY WORDS: HEALTH LITERACY, HEALTH-PROMOTING BEHAVIOR, PATIENT, HEART FAILURE
INTRODUCTION
The prevalence ofchronic diseases is a challenge in the
present century in health and treatment sector (Kar-
baschi et al. 2012). Among chronic diseases, the preva-
lence of congestive heart failure is increasing(Rahnavard
et al, 2006). As in the whole world, 23 million people
are suffering fromheart failure and annually two mil-
lion new casesof heart failureare diagnosed(Shiba and
Shimokawa, 2011). However, inIran,no detailed data
exists from people withheart failure(Rezaee loye et al,
2009). At the same time, with increase in number of
patients suffering from chronic diseases, likeheart fail-
ure, systems presenting health services face numerous
dif culties in long runtoprovide services to these peo-
ple. In other words, chronic diseases need chronic care.
Therefore, many believe that self-care should be per-
formed by patients, in order toorganize these patients
and facilitate their affairs(Mellen, 2002). Based on the
ndings of previous studies, high mortality rate, inap-
propriate use of preventive services, and deterioration
ofheart failureare associated with inadequate health lit-
eracy (Dennison et al, 2011).
Inadequate health literacy is de ned asthe limited
ability of people for acquiring, interpreting, and under-
standing primary information and health services that
are necessary for appropriate decision-making inhealth
areas (Raisi et al, 2013). Among patients with heart fail-
ure, as well,low health literacy is associated with mortal-
ity (Eckman et al, 2015).
According to studies by American Center for Health
Care Strategies,people withlow health literacy are
unlikely tounderstand and practice the written and
oralinformation presented by the specialists(Raisi et al,
2011). Recent reviews have reported poor health literacy
in 33 to 51% of adults discharged from hospitals and
more than60% of referrals to cardiac clinics (Fernan-
dez, 2014); while,heart failuredisease can affect routine
life activities, due to its natural capability. As a result,
these patients become dependent to others for self-
care (Abbasi et al, 2010). Today, health literacy is also
an important concept inwidespread aspects of health
promotion (Kanj and Mitic, 2010).Epidemiologicalstud-
ies have shown that the development of risk factors for
coronary artery disease can be controlled by having a
healthy lifestyle and people can improve their health
through health-promoting behaviors (Mohseni Pouya
et al, 2016).
Pender have suggestedthat health-promoting behav-
iors including exercise, nutrition, stress management,
interpersonal relationship, spiritual growth, and health
responsibilities reduce the risk of disease (Hosseini
et al, 2015). These behaviorsare one of themajor meas-
ures exterminating health that is known as abackground
factor in preventing many diseases (Raisi et al, 2011).
With regard to the importance of two issues ofhealth
literacy and health-promoting behaviorsin patients with
heart failure and regarding the report ofAgency for
Health Care Research and Quality on need for further
researches more on health literacy and the way itaffects
people’s health (Raisi et al., 2013) and consideringthe
fact that until now the relationship between health lit-
eracy andhealthy behaviorsin cardiac patients has not
been studied inIran, the present research evaluated the
relationship between health literacy level and health-
promoting behaviorsin patients with heart failure as one
of the most important vulnerable groups.
MATERIALS AND METHODS
Inthis correlational study, a total of 300 of patients suf-
fering from heart failure referred to cardiac clinics of
hospitals af liated to Shahid Beheshti University of Med-
ical Sciences were selected by random cluster sampling
according to the following inclusion criteria: diagnosis
of heart failure grade 2 and 3 in medical records accord-
ing to doctor’s diagnosis, minimum age of 25 years and
maximum of 65 years, ability to read and write Farsi
texts, passing at least six monthsafter naldiagnosis of
the disease, receivingpharmaceutical treatment for heart
failure (pills and medicinal regimen). Datawas collected
through two questionnaires and a scale that included the
following tools:
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS THE RELATIONSHIP BETWEEN HEALTH LITERACY AND HEALTH PROMOTING BEHAVIOR 115
Mahrokh Imanian et al.
1. Demographic information questionnaire (includ-
ing a total of 7 questions, 5 questions related to
personal information and 2 questions related to
the disease).
2. Health literacy measurement: This tool was de-
signed by Montazeri et al.,in 2014that includes
33 items in 5 domains; 4 of theminclude access,
understanding, assessment, decision-making, and
employing the information, each containing 6, 7,
4, and 12 items, respectively, and the reading skill
contains 4 items with 5-item Likert scale.
3. HPLP2: This scale is used toassesshealth-promoting
behavior, which includes spiritual growth, respon-
sibility, physical activity, nutrition, interpersonal
relationship, and stress management, designed by
Walker et al (1987), containing 52 items and 4-op-
tionLikert scale that wastranslated by Hosseini
et al., in 2010 (Hosseini, 2013).
In the present research, validity of the demographic
questionnaire was determined through qualitativem-
ethod. Also, todetermine the validity, other qualitative
method was used to determinefacevalidity and qualita-
tive and quantitative methods were used for determine
content validity. Content validity index (CVI)was deter-
mined using quantitative methods. For this purpose,
opinion of 10 experts in thenursing eld was used. CVI
of the Health literacy measurement and HPLP2 was
0.92, and 0.94, respectively. To determine the reliabil-
ity of the tools in the present study, internalconsistency
(Cronbach’s alpha) and stability (Interclass Correlation
Coef cient (ICC)) were used. Cronbach’s alpha coef -
cient of the total health literacy tool and HPLP2 was
= 0.78, and 0.87, respectively. Also, total ICC of this
tools was calculated = 0.82, and 0.79, respectively. To
gather data, aftercon rming the proposal of the research
and getting introduction letter and receivingsampling
license, 7 hospitals were purposively selected based on
the list of hospitals with cardiac clinic af liated toSha-
hid Beheshti University of Medical Sciences, Tehran.
Then, one of the researchersselected hospitals randomly
and referred to each clinic (which was assessed by the
researcher before) during working hours. Then, samples
were selected randomly among patients with quali ed
conditions of sampling in the research. Then, while pro-
viding necessary explanation about the research objec-
tives and emphasis on con dentiality of data, written
informed consent letter was obtained from patients and
the research tools were completed orally and by asking
participants.
To analyze data, SPSS software version 19 was used.
To report descriptive data,mean and SD, frequency-
and percentage were used. To analyze data in infer-
ential statistics, Kolmogorov-Smirnov test was used
and when the data distribution was normal,parametric
tests(independent t-test, Pearson correlation coef cient)
and when the data distribution was not normal, non-
parametric tests (Mann-Whitney-U, Kruskal-Wallis and
Spearman correlation coef cient) were used. Finally,
after univariate analysis, to assess the impact of vari-
ables beside each other on the outcome variable (health
promotion behaviors), all variables witha possibility
greater than 0.2 enteredmultiple regression model.
RESULTS AND DISCUSSION
The results showed that men included 51.7% of patients
with heart failure and 86% were married. Mean and
SDof age of participants was 54.83±8.21 and they were
mostly at age range 60 to 65 years. 39.3% of partici-
pants had secondary school education and 98%had no
history of employment inarea of medical sciences. Most
of participants (57.7%) had a monthly income of less
than 250,000 Tomans per family member. Also, 90% of
participants stated a history of hospitalization due to
heart reasons. At the same time, 84% of the participants
claimed no history of education in the form of lea ets,
pamphlets or oral training (Table 1).
Based on the results of the current study,mean and
SD score of health literacy in patients with heart failure
was 3.29±0.6 and 87.7% of participant showed moder-
atehealth literacy. Also, mean and SD of health-promot-
ing behaviors of participant in the study was 2.42±0.29
and 57% of participant had moderate level. Resultsof
Pearson statistical test showeda signi cant positive cor-
relation betweenhealth literacy and health-promoting
behaviors(P<0.001). Therefore, higher level of health lit-
eracy increased the health-promoting behaviors score in
patients with heart failure.
Amongthe subscales of health literacy,mean and SD
scores of total participants in thereading skill was higher
than other skills (3.8±0.87), and in the aspect of evalu-
ation and decision-making,the mean and SD scores of
people was less than other factors (3±0.83). The results
of independent t-test showed no signi cant difference
in scores of overall health literacy between women and
men (P>0.05). Among other demographic variables of
health literacy, marital status and monthly income had
a signi cant relationship (P>0.05). Pearson correlation
test showed signi cantdifference intotal health liter-
acy at different age groups with education (P<0.001).
Table 2 shows the correlation of health literacy with age
and educational status of participants in the research.
Inthe elds of health-promoting behaviors, mean and
SD scores of participantswas higher in interpersonal
relationship thanother subscales (2.8±0.34) and was the
leastin the stress management with a mean and SD of
116 THE RELATIONSHIP BETWEEN HEALTH LITERACY AND HEALTH PROMOTING BEHAVIOR BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
Mahrokh Imanian et al.
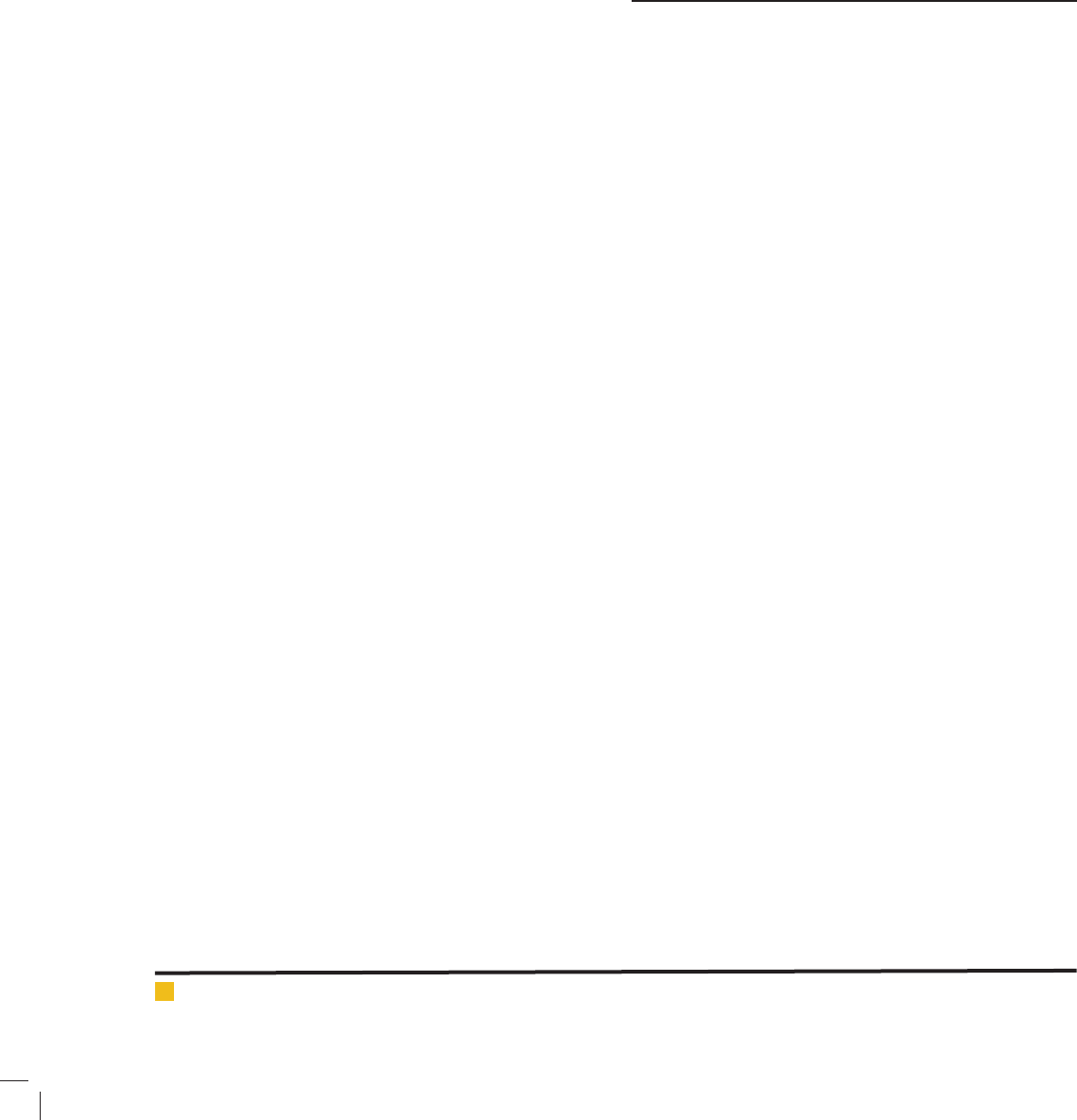
Table 1. Frequency of distribution of demographic characteristics of patients
variable number %
Sex
male 155 51.7
female 144 48.3
Education
primary 81 27
Middle (guidance level) 118 39.3
Secondary 14 4.7
College 43 43
Employment status
Working in medical sciences 4 1.3
Not employed in medical sciences 296 98.7
Marital status
Single 15 5
Married 258 86
Divorced 1 0.3
Widow(er) 26 8.7
Age
25-29 4 1.3
30-34 5 1.7
35-39 6 2
40-44 20 6.7
45-49 20 6.7
50-54 75 25
55-59 51 17
60-65 119 39.7
Monthlyincome
Morethan 250,000 Tomans per family member 32 32
Lessthan 250,000 Tomans per family member 36 36
History of hospitalization
Yes 270 90
No 30 10
Historyof education
Yes 48 16
No 252 84
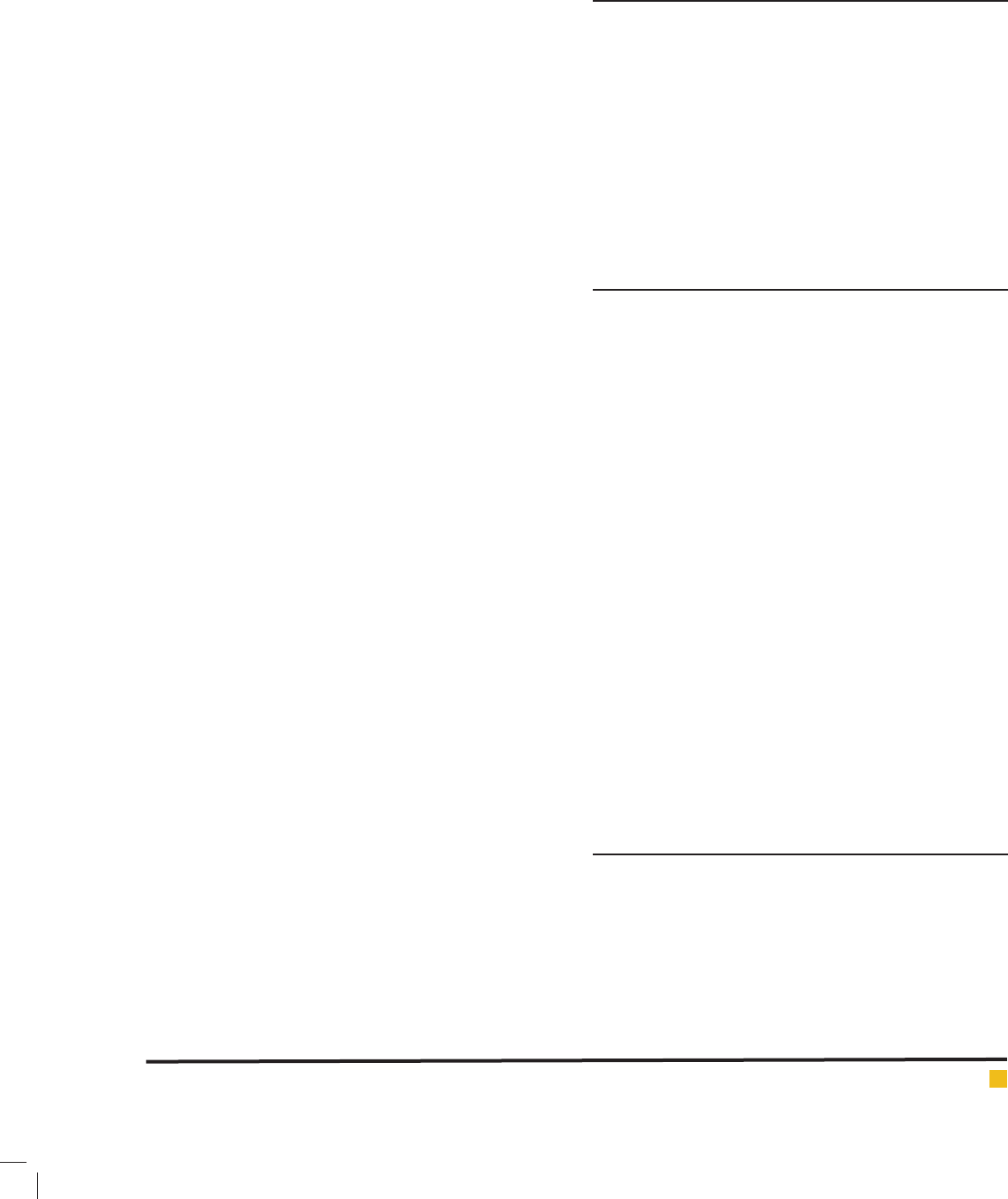
Table 2. correlation between health literacy and health-
promoting behavior with age and educational level
Scale
Age Educationalstatus
r p-value r p-value
Health literacy ** -0.41 <0.001 0.82 <0.001
Health-promoting
behavior**
-0.18 0.002 0.6 <0.001
**Correlationis signi cant at 0.05.
2.21±0.32, had the lowest score. The results of independ-
ent t-test showed signi cant differences in health-pro-
moting behaviors betweenthe studied women and men
(P=0.02) andstudied men were in better condition. Total
health-promoting behaviorswere signi cantly asso-
ciated only with monthly income (P<0.001). Pearson
correlation coef cient showed signi cant differences
in health-promoting behaviors in different age groups
and educational status (P<0.001). The correlation test of
health-promoting behaviors with education level and
age are expressed in table 2. Also, table 3 shows the cor-
relation between health literacy and health-promoting
behaviors subscales in the study subjects.
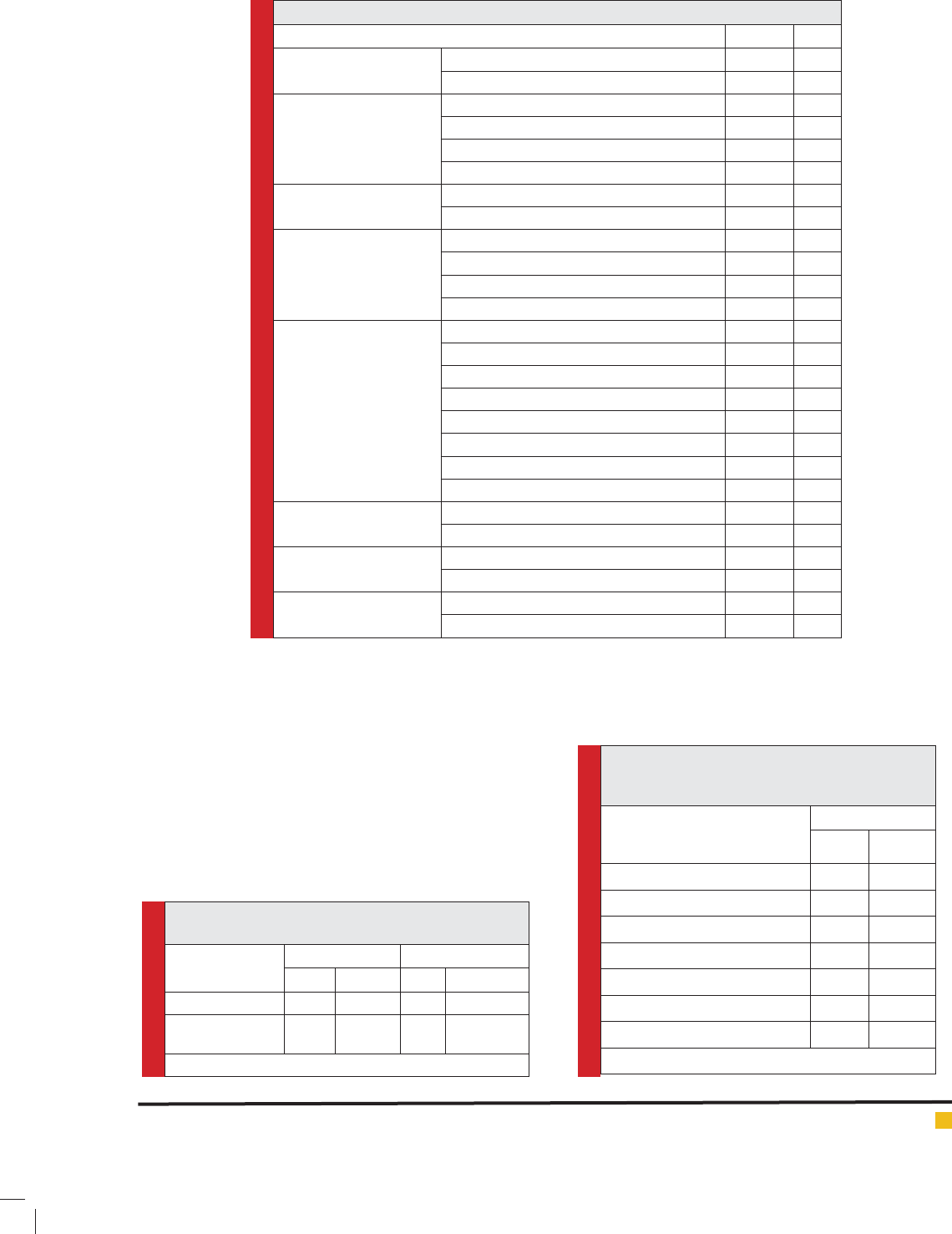
Table 3. Correlation between health literacy and
subscales of health-promoting behaviorsin study
subjects
Subscale of health-promoting
behaviors
Health literacy
r p-value
Nutrition** 0.516 <0.001
Physical activity ** 0.520 <0.001
Interpersonal relationship ** 0.457 <0.001
Health responsibility** 0.547 <0.001
Spiritual growth** 0.607 <0.001
Stress management** 0.544 <0.001
Total health-promotingbehavior 0.66 <0.001
**Correlation is signi cant at 0.05.
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS THE RELATIONSHIP BETWEEN HEALTH LITERACY AND HEALTH PROMOTING BEHAVIOR 117
Mahrokh Imanian et al.
The results of multiple regression models showed that
health literacy, education, age and income status were
effective factors onhealth-promoting behaviors(P>0.05).
Health-promoting behaviors in people with secondary
schooleducation had a0.13 less mean value than people
with college education and each unit increase in age,
increasedmeanHealth-promoting behaviors at 0.005
units.Health-promoting behaviors in people with an
income more than 250,000 Tomans per person had a
mean 0.1 unit increased than people with income less
than 250,000 Tomans per person. Each unit increase
inhealth literacy increased the meanHealth-promot-
ing behaviors0.29 units. Among theabove-mentioned
variables,health literacy had the greatest impact on
health-promoting behavior. The results ofmultiple
regression models are demonstrated in table 4.
DISCUSSION
The results showed that more than two-thirds of heart
failure patients have moderate health literacy. This nd-
ing is consistent with the results of studies byTehrani-
Banihashemiet al., 2007; Raisi et al., 2013; Mollakhalili
et al., 2014; Mo’tamedi et al., 2016; Raisi et al., 2011
inside our country, and abroad researchesby Tung et al.,
2014; Moseret al., 2015; and Jovis_veranes et al., 2011.
Regarding the ndings of the above-mentioned studies,
it should be noted that patients withchronic conditions,
like heart failureare at greater risk o nadequate care and
weak consequences, such as lack of knowledge ofdisease,
poor care, increasednumber of hospitalization and mor-
tality caused by the disease.So, patients need adequate
health literacy to participate in health care systems and
appropriate health decisions (Mollakhalili et al., 2014).
Theresults of the current study showed that health lit-
eracy is an important factor affecting health-promoting
behaviors in heart failure patients. Tsai et al (2014) and
Raisi et al (2013) also found similar results in their study.
In the present study, patients with higher health literacy
had a better condition in all aspects of health promot-
ing behaviors. As increase in patients’health literacy
increased the physical activity levels. Also, these people
had a better nutritional status and sense of responsibil-
ity to their health. In this regard,Mollakhalili et al (2014)
have pointed out that health literacy led to empower-
ment of people to apply information and health-related
commands. Considering the effect of health-promoting
behaviorsin patients with heart failure on advancing
health and quality of life,it decrease health-related costs
to the same proportion, so health literacy should be con-
sideredas a factor that promotes healthbehaviors, cre-
ate healthy life style and nally improves the quality
of life. Meanwhile, the weaker health literacy was more
prevalent among older patients. Higherhealth literacy
in younger patients can be attributed to the fact that
inthe present study,this group with higher level educa-
tion and more information on application of commu-
nicational media, like internet, has fewer problems and
higher mean scores compared to older patients. Also,
the higher physical power and probably lower inci-
dence of comorbidities of heart failure, such as diabe-
tes and hypertension,and lessinvolvement of the joints
cause higher physical activity were observed in younger
patients. Based on the ndings of the present research,
health literacy had no signi cant relationship with
gender of patients (P>0.05). Therefore, the amount and
method of understanding and interpretation of health
information were not different betweenwomen and men
and both groups need attention of the authorities con-
cerned in this regard. But independent t-test showed sig-
ni cant difference between gender andhealth-promoting
life style(P<0.05). According to the results of the current
study, generally, men were more likely to take care of
their health than women. In the study by Tallet al (2014)
and Nuthwer and Stump (2000), there was also a sig-
ni cant relationship betweenhealth-promoting life style
and sex (P<0.001). In the present study, all sub-scales
ofhealth literacy and health-promoting behaviorshad
higher scores among college-educated individuals than
those with lower educational level. Tsai’s study (2014), as
well,showed a signi cant association between education
and health literacy and these people were more likely to
have aneducational level above high school (P<0.001).
Notably,in thepresent study, allparticipants were literate,
who were placed in that 4 educational groupsandhigher
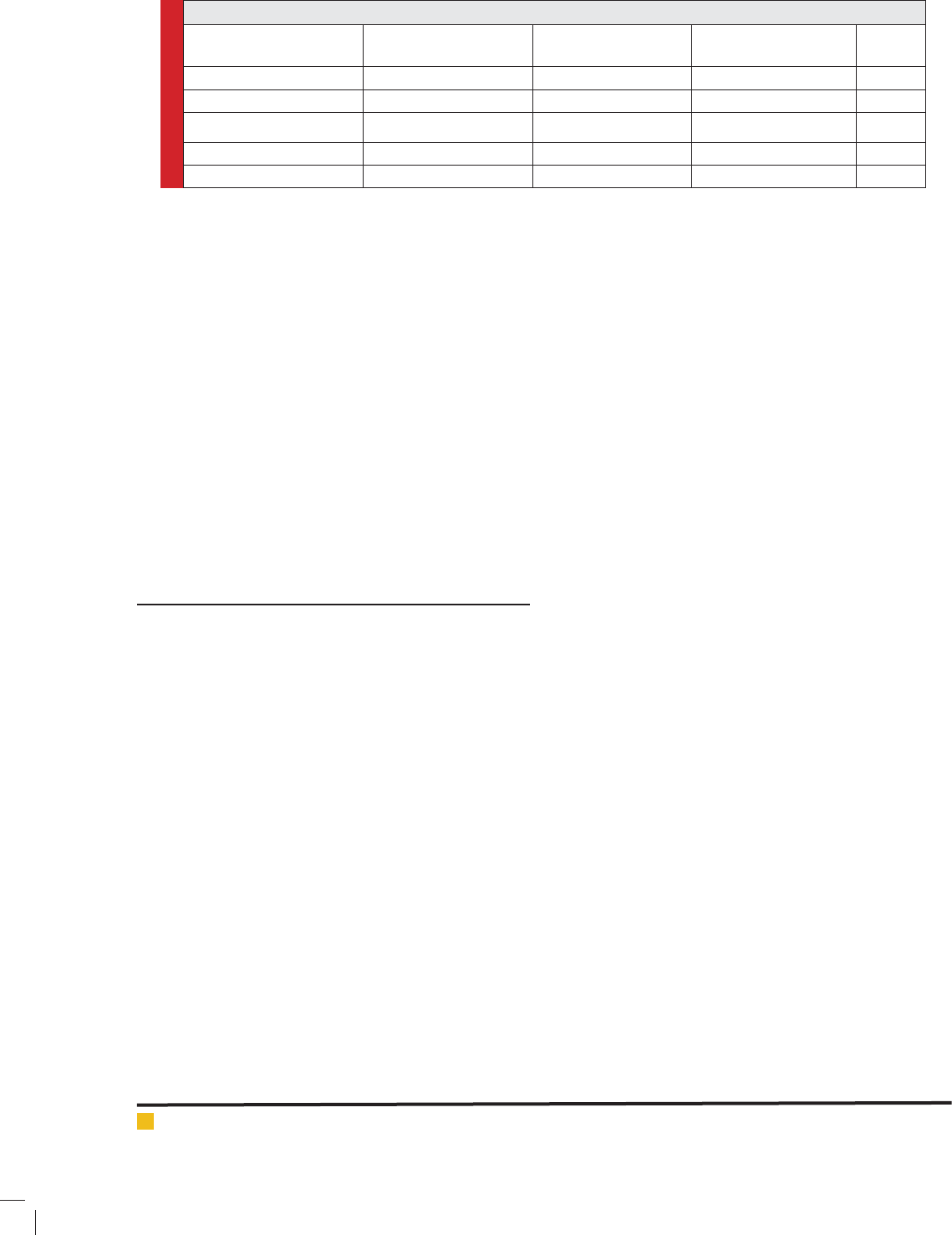
Table 4. The results of multiple regression model tto assess effective factors on health-promoting behaviors
Variable
Non-standardized
regression coef cients
Standard deviation of
regression coef cients
Standardized
regression coef cients
p-value
Intercept 0.53 0.24 0.03
Health literacy 0.29 0.03 0.59 <0.001
Secondary school education -0.15 0.07 -0.26 0.03
Age 0.005 0.002 0.1 0.005
Income status 0.1 029/0 0.17 <0.001
118 THE RELATIONSHIP BETWEEN HEALTH LITERACY AND HEALTH PROMOTING BEHAVIOR BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
Mahrokh Imanian et al.
level of education will possibly improve theirhealth
literacy. But in other studies in this regard, people’s
educational levelwere categorized as literate and illit-
erate that could have animpact on the results of the
study.
Lev and Owen (2000) writesin this regard that knowl-
edge and education increases thepotential ability of the
person against confusion and tension-causing factors
and cause success in self-care behavior. As academic
history of people is directly and meaningfully associated
with health literacy,it is necessary to pay more atten-
tion to education and societyhealth literacy, especially
on health information. Developing appropriate health
programs, providingsimple and understandable training
materials, spendingmore time with patients andslower
interviews by doctors and medical staff are the solu-
tions to help patients with lowhealth literacy to improve
theirliteracy. Inthe present study, the difference between
people with and without a history of work experience
in medical areaswas not signi cant inhealth literacy
(P=0.3) and health-promoting behaviors (P=0.9). This
lack of difference is probably due to the small number
of people employed in medical sciencesparticipating in
the present study that accounted for only 1.3% of them.
Regarding the fact that the majority of participants in
the present study had secondary school education, lack
of high level health and treatment activity seems logi-
cal at this level of education. Another result of the pre-
sent study indicated that except interpersonal relation-
ship (P=0.13) and health responsibility (P=0.9), other
dimensions ofhealth-promoting behaviorshad a signi -
cant relationship with income status (P<0.05), which
can guide us to the fact that higher income does not
necessarily lead to higherhealth responsibility and vice
versa, people fromlow level of society do not take less
care of their health; thus, training programs should be
performed for all classesof the society. But higher mean
scores of people inother dimensions, like nutrition, was
due to higher income and can be justi ed due to better
access to nutrition.
Inthe present study, the mean score of total health
literacy and health-promoting behaviors was higher in
trained people than untrained, but this difference was
only signi cant in health literacy (P<0.001). Health lit-
eracy (P=0.2) and health-promoting behaviors(P=0.6)
had no signi cant relationship with history of hospi-
talization, so that people withno history of hospitaliza-
tion had highermean scores in both variables. It seems
that when the patient has no history of hospitalization
after 6 months from de nite diagnosis of heart failure,
it con rmshigher health literacy and more adherences
tohealth-promoting behaviorsin the patient. Thus, the
results of this research emphasize the importance of
health literacy in the society, especially in hospitalized
patients.
STUDY LIMITATIONS
In general, in this study, high number of questions of
the tools used was one of the limitations, which was
tried to be confronted by the following measurements:
dedicateenough time to samples,answer their questions,
consider a short break during interviews, and change the
order of the research tools to be completed. In addition,
the present study was performed in a cross-sectional
basis, so future research with longer follow-ups can
providea better understanding of the causality relation-
ships between variables.
CONCLUSION
The results of the current research showed that most
of patients had moderate (borderline)health literacy.
Therefore, these patients require more explanations by
medical staff to understand and implement thedoctors’
instruction and other information and it is necessary to
provide more time for relationships with their physicians
and nurse and receivea simpler and more understand-
able information. Also, health managers and caregivers
should pay attention to this issue and spend more time
and give health instructions to this category ofpatients.
In the end, assessinghealth-promoting behaviorsand
understanding the factors affecting it is of great impor-
tance that could improve the quality of life of patients
with heart failure, but it needs policy-making and plan-
ning in this area. Theimportance of health-promoting
behaviorsshould be considered more than before and
be included inhealth care policy-making and programs.
Regarding the vulnerability of heart failure patients and
increasing prevalence in near future and the resulting
associated challenge, planning is essential to face this
challenge and lack of programing and policy-making
in this regard will cause serious social, economic and
health problems for society.
ACKNOWLEDGEMENTS
The present article is the result of master’s thesis and
research project with the Ethics code sbmu2.rec.1394.138
in Shahid Beheshti School of nursing and midwifery.
The researchers express their sincere thanks to all who
helped us in different phases of the study, the respected
of cials of Shahid Beheshti School of nursing and mid-
wifery, patients with heart failure, managers of heart
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS THE RELATIONSHIP BETWEEN HEALTH LITERACY AND HEALTH PROMOTING BEHAVIOR 119

Mahrokh Imanian et al.
clinics in teaching hospitals af liated to Shahid Behesh-
tiUniversity of Medical Sciences.
REFERENCES
Abbasi A, Asayesh H, Hosseini S.A, Ghorbani M, Abdullahi
A.A, Rouhi Gh, Rahmani H. (2010) The relationship between
function and quality of life in patients with heart failure. South
medical journal. 13(1) 31-40.
Dennison CH, Mcentee M, Samuel L, Johnson B, Rotman S,
Kielty A, Russell S.D (2011) Adequate health literacy is associated
with higher heart failure knowledge and self-care con dence in
hospitalized patients. J Cardiovasc Nurs. 26(5): 359-367.
D (2014) Health literacy and related psychosocial factor and
measurement issues: A qualitative study and secondary analy-
sis of the health and retirement study. Dissertation Submitted
in Partial Ful llment of The Requirement For The Degree of
Doctor of Philosophy (Nursing). University of Michigan.
of nursing in Universities of Tehran, behaviorspattern test.
Doctoral thesis for nursing. Shahid Beheshti University of
Medical Sciences.
promoting behaviors and their association with certain demo-
graphic characteristics of nursing students of tehran city in
2013. Global Journal of Health Science; 7(2).
Hosseini M, Ashktorab T, Taghdisi M.H, Esmaeili Vardanjani A,
Ra ei H (2015) Health-promoting behaviors and their associa-
tion with certain demographic characteristics of nursing stu-
dents of tehran city in 2013. Global Journal of Health Science;
7(2).
Hossein Mohsenipouya, Fereshteh Majlessi, Davood Shojaeiza-
deh, Abbas Rahimi Foroushani, Rahman Ghafari, Vali Habibi,
and Azam Sey Makrani (2016) Health-related variables and
predictors of Health-promoting Lifestyle in cardiovascular dis-
ease patients. Electron Physician. 2016 Apr; 8(4): 2274–2280.
population of primary healthcare patients in belgrade, serbia.
Int J Public Health. 56(2):201-207.
Kanj m, mitic w (2010) Health literacy and health promotion,
de nition, concepts and examples in estern mediteranian
region. Who Regional Of ce fot the Estern Mediteranion.
Karbaschi K, Farsi S.A. (2012) Revealing the concept of self-
care and its application for nurses. Journal of nursing Military
School of Republic of Islamic Iran. 12(1). 22. 14-16.
Mollakhalili H, Papi A, Shari rad Gh.R, Zare-Farashbandi F,
Hasanzadeh A (2014) Health literacy in patients hospitalized at
educational hospitals af liated to Isfahan University of Medi-
cal Sciences. Health information management. 11(4). 364-373.
Nothwehr F,Stump T (2000) Health-promoting behaviors
among adults with Type 2 Diabetes. Findings from the Health
and Retirement Study. Preventive Medicine. 30. 407–414.
Lev E.L, Owen S.V (2000), Counseling women with breast can-
cer using principles developed by albert bandura. Perspective
in psychiatric Care; 36(4):131-139.
McNaughton C.D, Cawthon C, Kripalani S, Liu D, Storrow A.B,
Roumie CH.L (2015) Health literacy and mortality: A cohort
study of patients hospitalized for acute heart failure. American
Health Association (J Am Heart Assoc).
Mellen P.B (2008) Deteriorating dietary habits among adults
with hypertention. Archives of Internal Medicine. 168(3). 308-
314.
Moser D.K, Robinson S, Biddle M.J, Pelter M.M, Nesbitt T.S,
Suthard J, Cooper L, Drucup K (2015). Health literacy predicts
morbidity and mortality in rural patients with heart failure.
Journal of Cardiac Failure. 21(8).
Motamedi F, Malekzadeh S, Azami M, Mirzaei M (2016) Health
literacy of cardiovascular patients admitted to private hospi-
tals in Kerman. International Journal of Advanced Biotechnol-
ogy and Research (IJBR). 7(1). 239-247.
Rahnavard Z, Zolfaghari M, Kazemnejad A, Hatamipour Kh.
(2006) Assessing the quality of life and factors affecting it in
patients with congestive heart failure. Journal of School of
nursing and midwifery of Tehran University (Hayat). 12(1)
77-86.
Rezai-Loye H.A, Dalvandi A, Hosseini M.A, Rahgozar M. (2008)
The effect of self-care education on quality of life in patients
with failure of heart. Rehabilitation. 2(10).38
Raisi M, Javadzadeh S.H, Mostafavi F, Tavasoli A, Shari rad
Gh.R (2013) Health literacy and health-promoting behavior-
sin elderly of Isfahan. Journal of health system research. 8(9).
127-836.
Raisi M. Mostafavi F, Hasanzadeh A, Shari rad Gh. (2011) The
relationship betweenhealth literacy andgeneral health status
healthbehaviorsin elderly city of Isfahan. Journal of health
system research. 7(14).
Shiba N, Shimokawa H (2011) Prospective care of heart failure
in Japan: lessons from CHART studies. European Association
for Predictive, Preventive and Personalised Medicine(EPMA
Journal). 2: 425–438.
Tsai M.H, Cheng Ch.Y, Chang Sh.Ch, Yang Y.M, Wang H.H
(2014) Health literacy and health promoting behaviors among
multiethnic groups of women in Taiwan. JOGNN. 43. 117-129.
Tol A, Mohebbi B, Sadeghi R,V Maheri A,B, Eshraghian M.R
(2014) Determinants of Health-Promoting Behaviors among
Type 2 Diabetic Patients: Voice of Iran. Journal of Endocrine
and Metabolic Diseases. 4. 219-224.
Tung H.H, Lu T.M, Chen L.K, Liang Sh.Y Shu-Fang Wu Sh.F,
Chu K.H (2014) Health literacy impact on elderly patients with
heart failure in Taiwan. Journal of Clinical Gerontology &
Geriatrics. 5. 72-76.
120 THE RELATIONSHIP BETWEEN HEALTH LITERACY AND HEALTH PROMOTING BEHAVIOR BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS