
Medical
Communication
Biosci. Biotech. Res. Comm. 10(3): 571-579 (2017)
Area-metric analysis of the quality of obturation of
four different techniques: An ex vivo study
Yazdan Shantiaee
1
, Setareh Rostami
2
, Shiva Shojaeeian
3
and Sanaa Jabbari
4
1
Associate Professor, Dental School of Shahid Beheshti University of Medical Sciences, Tehran, Iran
2
Dentist, Shahid Beheshti University of Medical Scineces, Tehran, Iran
3
Assistant professor, Department of Endodontics, Dental school of Shahid Beheshti University of Medical
Sciences, Tehran, Iran
4
Post Graduate Student, Department of Endodontics, Dental School of Shahid Beheshti University of Medical
Sciences, Tehran, Iran
ABSTRACT
The aim of this study was to compare different obturation techniques in straight canals in term of the percentage of
gutta-percha lled area (PGFA) and percentage of sealer lled area (PSFA) and voids. The obturation time was also
compared. Straight root canals of 40 extracted human premolars were instrumented with Mtwo rotary les and lled
as follows: Control: cold lateral compaction with standard master and accessory cones. CLS group: cold lateral com-
paction with 0.04/35 master cone and standard accessory cones. CLNS group: cold lateral compaction with 0.04/35
master cone and non-standard medium- ne (MF) accessory cones. WLS group: warm lateral compaction with 0.04/35
master cone and standard accessory cones. AH26 sealer was used. The teeth were sectioned horizontally at 3, 6 and
9 mm from the apex. The total area of each section and the PGFA, PSFA and percentage of voids were calculated.
Data were analyzed using repeated measures ANOVA and Kruskal-Wallis test.The CLNS was the fastest method with
a signi cant difference with the control group (P<0.05) while WLS required signi cantly more time than all other
techniques (P<0.05). In the apical and coronal thirds, CLNS yielded signi cantly lower PGFA (P<0.05). In the middle
third, WLS yielded signi cantly higher PGFA than CLNS (P<0.05). Cold lateral compaction using gutta-percha master
cone with 4% taper and MF accessory cones is not ef cient for obturation of canals. Also, warm lateral compaction
has no superiority to cold lateral compaction in straight canals.
KEY WORDS: COLD LATERAL CONDENSATION, SEALER, WARM LATERAL COMPACTION, OBTURATION, GUTTA-PERCHA
571
ARTICLE INFORMATION:
*Corresponding Author: Sanaa_jabbari@yahoo.com
Received 12
th
July, 2017
Accepted after revision 27
th
Sep, 2017
BBRC Print ISSN: 0974-6455
Online ISSN: 2321-4007 CODEN: USA BBRCBA
Thomson Reuters ISI ESC and Crossref Indexed Journal
NAAS Journal Score 2017: 4.31 Cosmos IF: 4.006
© A Society of Science and Nature Publication, 2017. All rights
reserved.
Online Contents Available at:
http//www.bbrc.in/
DOI: 10.21786/bbrc/10.3/35
572 AREA-METRIC ANALYSIS OF THE QUALITY OF OBTURATION OF FOUR DIFFERENT TECHNIQUES BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
Yazdan Shantiaee etal.
INTRODUCTION
Achieving a hermetic apical, lateral and coronal seal is
an important factor to prevent entry of microorganisms
into the canal and periapical tissues, and depends on
proper cleaning and shaping and ef cient obturation
of root canal system (Wu etal. 1993; Mollander etal.
1998; Schafer etal. 2012). Advances in formulations of
root canal irrigating solutions and rotary devices have
greatly enhanced proper cleaning and shaping of root
canal system. Homogenous, three-dimensional lling of
root canal space by gutta-percha and sealer can greatly
increase the success of endodontic treatment (Wu etal.
2002). Gutta-percha cones must be compacted next
to each other with a very thin layer of sealer between
gutta-percha cones and canal wall to minimize voids
(Gordon et al. 2005). Gutta-percha dimensions do not
change over time (Wu etal. 2009) but sealer undergoes
shrinkage and dissolution (Al-Hadlaq etal. 2010; Nica
etal. 2012). Following dissolution of sealer over time,
voids are created in the canal, which can compromise
the seal and enable entry and accumulation of micro-
organisms and subsequent development of periapical
lesions and eventual treatment failure (Jarret etal. 2004;
Schafer etal. 2012).
If the volume of gutta-percha mass compared to that
of sealer increases, less voids will be created over time
and coronal and apical seal will not be compromised.
This would increase success of endodontic treatment
(Kazemi etal. 1993; Kontakiotis etal. 1997; Wu etal.
2009). A systematic review reported that canals lled
with adequate, homogenous gutta-percha mass showed
primary endodontic success (Ng et al. 2008). Another
study reported that homogeneity of gutta-percha mass
had a signi cant positive effect on periapical health and
success of endodontic treatment (Lee etal. 2012).
Root canal lling length should be equal to the work-
ing length to ensure that the entire prepared space is
lled with gutta-percha (Kojima etal. 2004; Schaeffer
etal. 2005). Thus, maximum penetration of master and
accessory gutta-percha cones must be ensured. The taper
of master and accessory gutta-percha cones is an impor-
tant factor affecting the penetration depth of gutta-per-
cha into the canal such that the greater the compatibil-
ity of taper of gutta-percha with that of root canal, the
more homogenous and regular their arrangement would
be in the canal. Some authors believe that using a single
gutta-percha cone that matches the taper and size of
prepared canal would have the best adaptation to canal
walls (Whitworth, 2005; Schafer etal. 2013).
Several methods have been suggested for root canal
obturation such as lateral compaction, vertical con-
densation, single-cone obturation with a gutta-percha
cone that matches the size and taper of prepared canal
(Schafer et al. 2012), use of a solid core covered with
gutta-percha, injection of soft, plasticized gutta-percha
into the canal and use of physically and chemically
modi ed gutta-percha with higher adaptation (Skinner
etal. 1987; Whitworth, 2005; Schafer etal. 2013). Each
of these techniques has its own advantages and disad-
vantages, and no consensus has been reached on the
superiority of one technique over the others (Aqrabawi
etal. 2006; Ng etal. 2007).
Lateral compaction is a commonly used root canal
obturation method due to its simplicity (Cailleteau etal.
2009). This technique can be practiced in most clinical
situations and enables length control during compac-
tion (Gilhooly etal. 2001). However, its main drawback
is that it cannot create a homogenous mono-block of
gutta-percha. Master and accessory gutta-percha cones
are placed next to each other but remain separate and
the space between cones is expected to be lled with
sealer, which undergoes shrinkage and dissolution over
time. In thermoplastic methods such as warm vertical
condensation and warm lateral compaction, heat is used
to cause physical changes in gutta-percha and increase
its plasticity and adaptation to the canal walls. Warm
lateral compaction allows length control and at the same
time, heat results in adherence of gutta-percha cones
to each other and formation of a solid mass (Jacobsen
etal. 1993).
Considering the need for decreasing working time in
dental of ce, gutta-percha cones with 4% and 6% tapers
and non-standard medium ne (MF) and ne- ne gutta-
percha cones were introduced to the market for faster
obturation of root canals. However, deep penetration
of accessory cones with greater taper is dif cult. Stud-
ies on penetration depth of spreader alongside a master
cone with 2% taper and master cones with higher than
2% taper showed greater penetration depth of spreader
next to master cone with 2% taper (Bal etal. 2001; Wil-
son etal. 2003). Thus, complete penetration of accessory
cones to the working length and obtaining an apical seal
with the use of these gutta-percha cones is a matter of
debate. This study has aimed to assess the quality of root
canal lling by measuring the percentage of gutta-percha
(PGFA) and sealer lled areas (PSFA) and voids in use of
four different obturation techniques. Duration of obtura-
tion was also compared among the four methods.
MATERIAL AND METHODS
This in vitro, experimental study was conducted on
40 single-canal maxillary and mandibular premolars
with straight canals. The teeth were randomly divided
into four groups (n=10). The highest mean difference
expected for PGFA among the groups was considered to

BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS AREA-METRIC ANALYSIS OF THE QUALITY OF OBTURATION OF FOUR DIFFERENT TECHNIQUES 573
Yazdan Shantiaee etal.
be 0.13 with a standard deviation of 14% according to a
study by Schafer etal. in 2012. Considering 80% power
of study and type one error of 5%, sample size was cal-
culated to be 10 in each group.
The inclusion criteria were single-rooted premolar
teeth extracted for orthodontic or periodontal reasons
with a straight canal and one apical foramen and no
visible root caries, no fracture or crack and no internal/
external root resorption or calci cation on radiographs.
The teeth had mature apices.
The exclusion criteria were presence of voids after
lling and incorrect working length. Teeth with no api-
cal constriction or fracture during cleaning and shap-
ing were also excluded. After collection, the teeth were
immersed in 3% sodium hypochlorite solution (Rakh-
shan, Tehran, Iran) at room temperature for two days.
Calculus (if any) was removed using a universal curette
(Hu-Friedy, USA) and the teeth were evaluated under a
stereomicroscope (SZX9; Olympus, Tokyo, Japan) at 20
magni cation to ensure absence of root cracks. Paral-
lel periapical radiographs were obtained in mesiodis-
tal and buccolingual dimensions to assess root canal
anatomy. After access cavity preparation using 836 s-
sure and 801 round burs (SWS, Switzerland), a #15 K
le (Mani, Tokyo, Japan) was introduced into the canal
until its tip was visible at the apex. The teeth were then
radiographed and canal curvature was determined. The
selected 40 teeth had straight canals and #20 K le was
the largest initial le compatible with their root canal.
The crowns were then cut at the cementoenamel junc-
tion using a diamond disc (D & Z, Germany).
To determine the working length, a #15 K le (Mani,
Japan) was introduced into the canal such that its tip
was visible at the apex; working length was determined
1mm short of this length. All canals were cleaned using
#15 and #20 K les (Mani, Japan) and then by Mtwo
rotary NiTi les (VDW, Germany) with an endodontic
motor (NSK, Japan) with slow pull and push brushing
motion to the working length as recommended by the
manufacturer in the following order: 0.04/10, 0.05/15,
0.06/20, 0.06/25, 0.05/30, 0.04/35. A #10 K le (Mani,
Japan) was used after each rotary le for patency and
17% EDTA gel (Calasept, Nordiska Dental) was used
as chelator. Root canals were rinsed with 2cc of 1.5%
sodium hypochlorite (Rkhshan, Tehran, Iran). Smear
layer was removed by rinsing the canals with 5cc of
17% EDTA for one minute followed by a nal rinse with
saline. The root canals were dried with paper points (Ari-
adent, Tehran, Iran) and the teeth were randomly divided
into four groups of 10 and lled with AH26 sealer (Dent-
sply DeTrey-Germany) and gutta-percha (Metabiomed,
Korea) as follows:Control group: #35 standard gutta-
percha (2% taper) as master cone and standard accessory
cones were used in cold lateral compaction technique.
CLS groups: #35 standard gutta-percha (4% taper)
as master cone and standard accessory cones were used
in cold lateral compaction technique (cold lateral com-
paction with standard gutta-percha).CLNS group: #35
standard gutta-percha (4% taper) as master cone and
non-standard MF accessory cones were used in cold lat-
eral compaction technique (cold lateral compaction with
non-standard gutta-percha).WLS group: #35 standard
gutta-percha (2% taper) as master cone and standard
accessory cones were used in warm lateral compaction
technique (warm lateral compaction with standard gutta-
percha).Root canal lling with cold lateral compaction
technique was done as follows: Following root canal
preparation and drying, a standard gutta-percha cone
with 2% taper was used in the control group and with
4% taper in the CLS group to the working length. Api-
cal third of master cone was dipped in sealer and placed
into the canal, rotated in counter clockwise fashion and
removed. A proper size spreader was also selected based
on canal taper to reach 1mm of the working length with
master cone in the canal. Accessory cones were placed
and cut at the ori ce. No pressure was applied for verti-
cal condensation.
Cold lateral compaction in CLNS group was the same
as in the control and CLS groups with the exception of
4% taper of master cone and selected spreader. Also, non-
standard MF accessory cones were used. In WLS group,
the same procedures were followed with the exception
that after placement of master cone with 4% taper, the
thinnest tip of Obtura (E & Q Master Meta Biomed-Korea)
that could reach 2-4mm of the apex adjacent to master
cone was chosen and inserted as deep as possible into
the canal. After removal, #25 nger spreader was placed
adjacent to the heated master cone, removed immediately
and replaced with an accessory cone with 2% taper. This
process was repeated until complete obturation. Time
required for obturation of each canal was also calculated
from the time of placement of the rst gutta-percha to
completion of obturation using a chronometer (reported
in minutes). A control radiograph was also obtained from
the mesiodistal direction to ensure complete obturation.
The teeth were incubated at 37C and 100% mois-
ture for 14 days for completion of setting of sealer.
Using an endodontic motor, root surface was marked
at 3, 6 and 9 mm from the apex and the teeth were
xed to IsoMet cutting machine (Buehler IsoMet Low
Speed Saw 11-1180) from the coronal part using glue.
The roots were sectioned horizontally under copious
water. The slices were immersed in sodium hypochlo-
rite solution for one minute to eliminate dentin chips
and were then rinsed with 17% EDTA (Calasept Nord-
iska Dental) for one minute followed by a rinse with
water. The slices were photographed at 40 magni ca-
tion under a stereomicroscope (SZX9; Olympus, Japan).
574 AREA-METRIC ANALYSIS OF THE QUALITY OF OBTURATION OF FOUR DIFFERENT TECHNIQUES BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
Yazdan Shantiaee etal.
Photographs were saved in TIF format and assessed in
Adobe Photoshop CS6 1301.2 software. In this software,
the total surface area of the canal in each section and
the percentage of gutta-percha lled area (PGFA) and
percentage of sealer- lled area (PSFA) were separately
calculated on each image in pixels. The percentage of
void areas [total area of section-(PSFA+PGFA)] was also
calculated. These values were reported for each section.
All measurements were made by an examiner blinded to
the group allocation of teeth (Figure 1). The values were
recorded in Microsoft Excel 2013.
The PGFA and PSFA data in different sections were
analyzed using repeated measures ANOVA. Obturation
time data were analyzed using ANOVA and data of per-
centage of voids were analyzed using the Kruskal Wallis
test. The mean and standard deviation of PGFA, PSFA
and void area were reported. For the comparison of the
mean PGFA and PSFA, repeated measures ANOVA was
used (since data were normally distributed). The Kruskal
Wallis test was used to compare the mean area of voids
in different sections. Data were analyzed using SPSS
version 21 (SPSS Inc., IL, USA).
RESULTS AND DISCUSSION
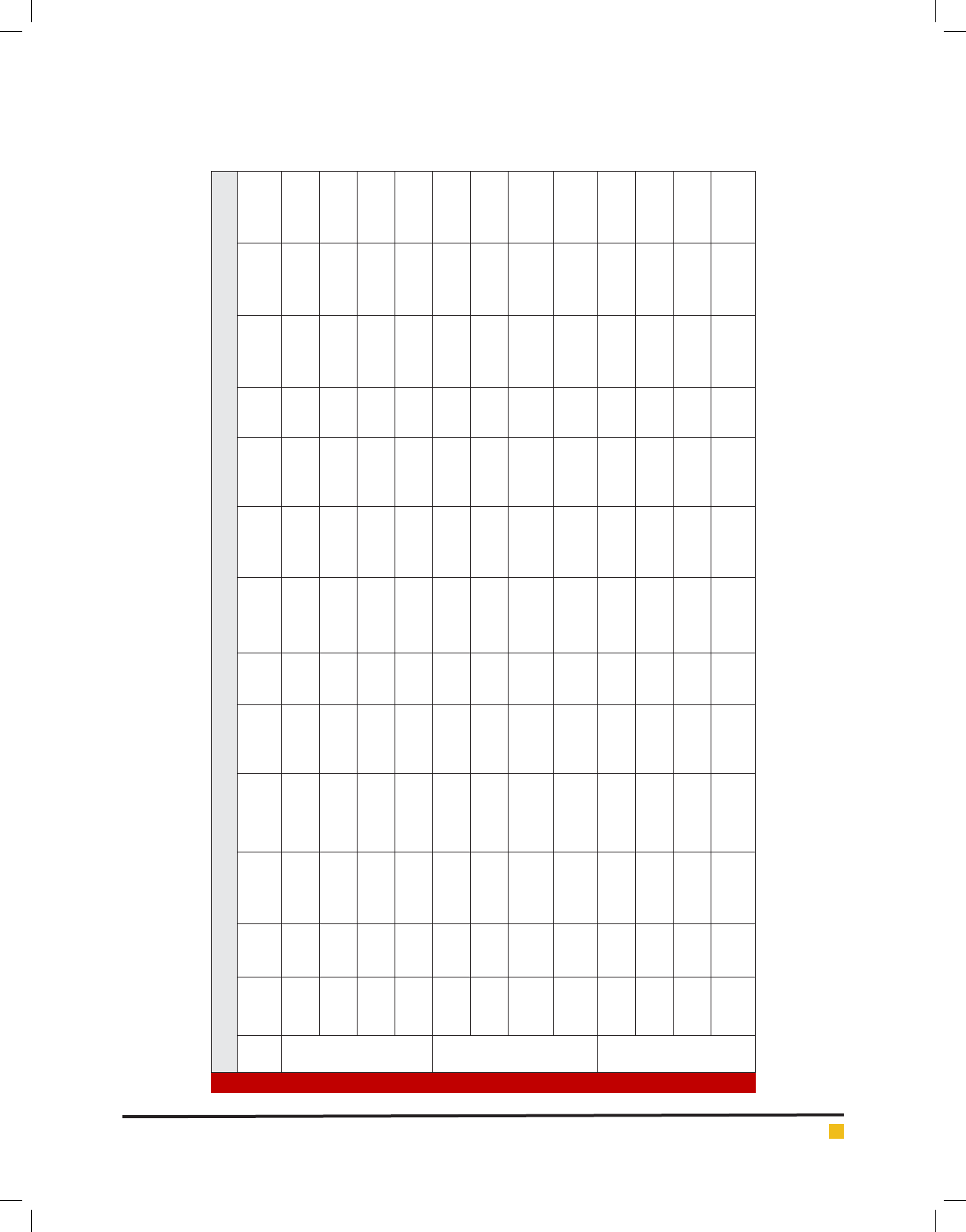
Table 1 shows the mean PSFA, PGFA and void area val-
ues in apical, middle and coronal sections. Table 2 shows
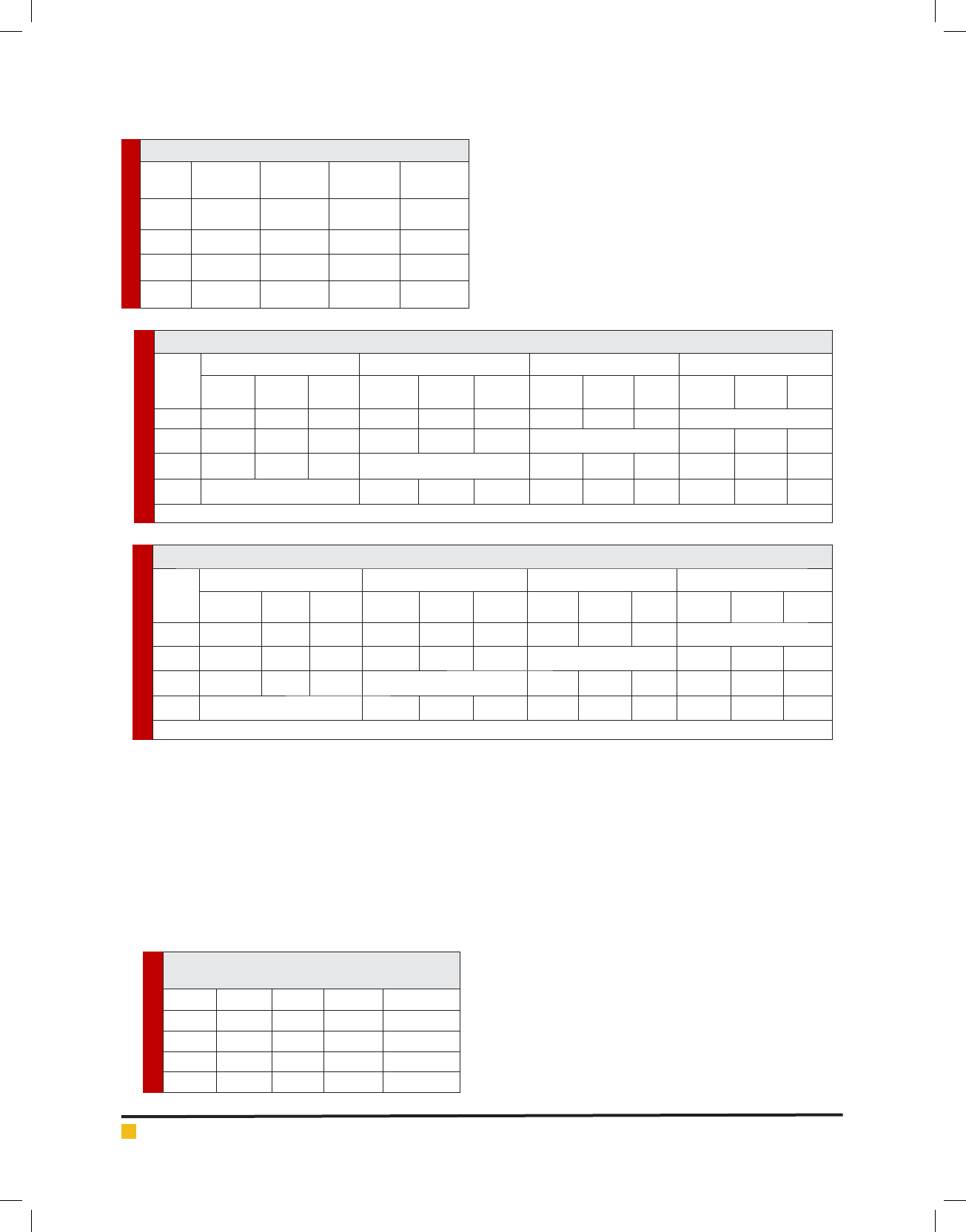
the mean time of obturation in the groups. Table 3 shows
the P values for the comparisons. As seen in Table 3,
in the apical section, CLNS group showed signi cantly
lower PGFA than other groups (P<0.05). PGFA of WLS
group was signi cantly higher than that of other groups
followed by CLS, control and CLNS groups, respec-
tively. The difference of WLS with CLNS was signi -
cant (P<0.05) but its difference with other groups was
not signi cant (P>0.05) in this respect. The CLS group
showed higher PGFA than the control group but this dif-
ference was not signi cant (P>0.05).
In the middle section, WLS showed higher PGFA than
other groups followed by CLS, control and CLNS groups,
respectively but only the difference between WLS and
CLNS was signi cant (P<0.05). The CLNS group showed
lower PGFA than other groups but this difference only
for WLS was signi cant (P<0.05). The CLS showed
higher PGFA than the control group but this difference
was not signi cant (P>0.05).In the coronal section, the
CLNS group showed signi cantly lower PGFA than other
groups (P<0.0001). The PGFA in WLS group was higher
than that in other groups followed by CLS, control and
CLNS groups. The difference between CLNS and WLS
was signi cant (P<0.0001) but other differences were
not signi cant (P>0.05). The CLS group showed higher
PGFA than the control group but this difference was not
signi cant (P>0.05).
As seen in Table 4, in the apical section, the CLNS
group showed signi cantly higher PSFA than other
groups (P<0.05). The PSFA in WLS group was lower than
that in other groups followed by CLS, control and CLNS
groups, respectively. The difference between WLS and
CLNS was signi cant (P<0.0001) but other differences
were not statistically signi cant (P>0.05). The CLS group
showed lower PSFA than the control group but this dif-
ference was not signi cant (P>0.05). In the middle sec-
tion, WLS group showed lower PSFA than other groups
followed by CLS, control and CLNS groups, respectively.
Only the difference between the WLS and CLNS groups
was signi cant (P<0.05). The CLNS group showed higher
PSFA than other groups but this difference only with
WLS was signi cant (P<0.05). The CLS group showed
lower PSFA than the control group but this difference
was not signi cant (P>0.05).
In the coronal section, the CLNS group showed sig-
ni cantly higher PSFA than other groups (P<0.0001).
PSFA of WLS group was lower than that of other groups
followed by CLS, control and CLNS groups, respec-
tively. The difference of WLS and CLNS was signi cant
(P<0.0001) but the difference with other groups was not
statistically signi cant (P>0.05). In general, in all sec-
tions, the WLS group showed higher PGFA and lower
PSFA than other groups followed by CLS, control and
CLNS groups, respectively. The difference between WLS
and CLNS in terms of PGFA and PSFA only in the mid-
dle third was statistically signi cant (P<0.05). The CLNS
group in all sections showed lower PGFA and higher
PSFA than other groups and this difference in the api-
cal and coronal section was statistically signi cant. The
CLS group compared to the control group showed higher
PGFA and lower PSFA in all sections but these differ-
ences were not statistically signi cant (P>0.05).
No signi cant difference was noted in apical, middle
and coronal sections of the four groups in terms of voids
(P>0.05).
As seen in Table 5, the mean time required for root
canal obturation in WLS group was signi cantly longer
than that in other groups (P<0.0001) followed by the con-
trol, CLS and CLNS groups, respectively. The mean time
required for root canal obturation in CLNS group was sig-
ni cantly shorter than that in the control group (P<0.05).
Three-dimensional obturation of root canal system is
necessary to prevent bacterial reentry and ensure long-
term success of endodontic treatment (Raina etal. 2007;
Michaud etal. 2008). Finding an ef cient technique with
the greatest ability to provide a hermetic seal is impor-
tant to guarantee the success of endodontic treatment
(Haikei etal. 2006). This study compared the quality of
obturation of straight root canals prepared with Mtwo
rotary les and lled with four obturation techniques by
measuring the surface area lled with gutta-percha and
Yazdan Shantiaee etal.
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS AREA-METRIC ANALYSIS OF THE QUALITY OF OBTURATION OF FOUR DIFFERENT TECHNIQUES 575
Table 1. Mean PSFA, PGFA and void area in the apical, middle and coronal sections of the four groups
Mean
(%)
Standard
deviation
Maximum Minimum
Mean
(%)
Standard
deviation
Maximum Minimum
Mean
(%)
Standard
deviation
Maximum Minimum
Apical
control 6.08 2.37 9.67 2.61 92.85 2.18 96.36 89.33 0.06 0.18 0.6 0
CLS 6.09 2.25 9.62 2.56 93.90 2.25 97.42 90.39 0 0 0 0
CLNS 16.79 9.92 20.31 13.26 83.20 9.92 79.69 86.72 0 0 0 0
WLS 5.03 3.44 8.55 1.50 94.96 3.44 98.48 91.45 0 0 0 0
Middle
control 4.43 2.33 7.07 2.73 95.09 2.33 97.27 92.91 0.47 0.84 2.20 0
CLS 3.96 3.17 6.36 2.02 95.80 3.17 97.98 93.62 0.50 1.59 5.05 0
CLNS 7.78 4.98 10.42 6.07 91.75 5.01 93.92 89.57 0.46 1.45 4.60 0
WLS 3.95 2.33 6.12 1.77 96.04 2.33 98.22 93.86 0 0 0 0
Coronal
control 5.29 4.69 9.20 2.23 94.28 4.69 97.75 90.81 0.42 0.90 2.50 0
CLS 5.23 3.59 9.11 2.15 94.46 3.48 97.93 90.99 0.40 0.81 2.50 0
CLNS 19.2 8.54 24.13 17.16 79.35 8.54 82.82 75.88 1.44 1.84 4.56 0
WLS 4.39 3.14 8.21 1.24 95.26 3.14 98.73 91.79 0.34 0.83 2.68 0
Yazdan Shantiaee etal.
576 AREA-METRIC ANALYSIS OF THE QUALITY OF OBTURATION OF FOUR DIFFERENT TECHNIQUES BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
Table 2. Obturation time in the four groups
MinimumMaximumStandard
deviation
Mean
(minutes)
Group
5.207.600.606.41Control
4.506.900.825.66CLS
3.906.200.825.03CLNS
6.5010.301.188.43WLS
Table 3. P values for the comparison of PGFA in the apical, middle and coronal sections of the four groups
WLS CLNS CLS Control
Coronal Middle apical coronal Middle apical coronal middle apical Coronal Middle Apical
Control 1 1 1 <0.0001* 0.203 0.001* 1 1 1
CLS 1 1 1 <0.0001* 0.067 0.001* 1 1 1
CLNS <0.0001* 0.045* <0.0001* <0.0001* 0.067 0.001* <0.0001* 0.203 0.001*
WLS <0.0001* 0.045* <0.0001* 1 1 1 1 1 1
*Signi cant.
Table 4. P values for the comparison of PSFA in the apical, middle and coronal sections of the four groups
WLS CLNS CLS Control
Coronal middle apical coronal Middle apical coronal middle apical Coronal Middle Apical
control 1 1 1 <0.0001* 0.206 0.002* 1 1 1
CLS 1 1 1 <0.0001* 0.068 0.001* 1 1 1
CLNS <0.0001* 0.046* <0.0001* <0.0001* 0.068 0.001* <0.0001* 0.206 0.002*
WLS <0.0001* 0.046* <0.0001* 1 1 1 1 1 1
*Signi cant.
Table 5. P values for the comparison of obturation
time in the four groups
ControlCLSCLNSWLSGroup
-0.280.01<0.0001Control
0.28-0.43<0.0001CLS
0.010.43-<0.0001CLNS
<0.0001<0.0001<0.0001-WLS
sealer using area-metric analysis. The results showed
that root canal obturation with non-standard accessory
cones and a master cone with 4% taper decreased the
gutta-percha mass and increased the sealer area. Use
of a master cone with 4% taper had no positive effect
on quality of obturation or working time. Warm lateral
compaction in straight canals had no superiority over
cold lateral compaction and took longer to accomplish.
In our study, root canals were prepared using Mtwo
rotary system since Schafer etal. (2016) in 2016 showed
that root canals lled with gutta-percha of Mtwo rotary
system had higher quality of obturation compared to
those lled with gutta-percha of Reciproc and WaveOne
systems. Also, we wanted to compare the percentage
of area lled with gutta-percha in case of using gutta-
percha with 4% taper. Thus, Mtwo was a suitable choice
for this purpose since #35 gutta-percha in Mtwo system
has 4% taper. Although master cone in our study was
#35 with 4% taper (matched single cone of Mtwo sys-
tem), not all the prepared canals follow the shape and
taper of nal le after preparation with the nal rotary
le, so we designed a group in which we placed acces-
sory gutta-percha cones between single cone and canal
walls to assess the possibility of improving the qual-
ity of obturation. Apical seal is an important param-
eter in success of endodontic treatment and improper
apical seal results in development of periapical lesions.
The results of our study showed that in the apical third,
use of non-standard gutta-percha alongside the master
cone with 4% taper signi cantly decreased the apical
seal and quality of obturation and decreased PGFA and
increased PSFA. Also, our results showed that use of
standard gutta-percha with 2% and 4% taper along with
2% accessory cones did not cause a signi cant change
in quality of obturation in the apical third. Although
PGFA in 4% gutta-percha group was higher and PSFA
was lower than that in other groups, these differences
were not signi cant and no difference in voids was
noted either. Based on our results, warm lateral com-
Yazdan Shantiaee etal.
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS AREA-METRIC ANALYSIS OF THE QUALITY OF OBTURATION OF FOUR DIFFERENT TECHNIQUES 577
paction had no superiority over cold lateral compaction
since no difference was noted between the two groups in
any of the assessed parameters.
Comparison of the mean time of obturation among the
groups showed that the mean time of obturation was sig-
ni cantly longer in WLS group compared to other groups.
This time in CLNS group was signi cantly shorter than
that in the control group. The CLS and control groups
were not signi cantly different in this regard. Schafer
etal. in 2012 compared the quality of root canal obtura-
tion with 2% and 4% taper gutta-percha cones by micro-
scopic area-metric analysis and found no signi cant dif-
ference between the two types in the apical region. None
of them provided a better apical seal. Romina etal.(2009)
performed area-metric analysis of root lling and showed
equal apical seal in use of gutta-percha cones with 2%
and 4% taper. Our results were in agreement with those of
the afore-mentioned studies.
We found no signi cant difference in time of obtu-
ration between the use of gutta-percha cones with 2%
and 4% taper, which was in agreement with the results
of Schafer etal.(2012). Our results regarding the use of
non-standard MF gutta-percha cones in comparison
with the use of standard gutta-percha showed that use
of non-standard cones along with a master cone with
4% taper decreased PGFA and increased PSFA in all sec-
tions and this difference in the apical and coronal thirds
was signi cant. Thus, use of MF accessory cones along
with 4% gutta-percha does not provide suitable apical
seal. In contrast to our results, VanGheluwe and Wilcox
in 1996 found no signi cant difference in apical seal of
standard and non-standard gutta-percha cones. Differ-
ence in the results of the two studies may be due to the
use of curved roots in their study. Use of warm lateral
compaction method in our study increased PGFA and
decreased PSFA in all sections, although insigni cantly.
No difference was noted in terms of voids. No signi cant
difference between warm and cold lateral compaction
techniques in our study may be due to our small sam-
ple size and use of straight canals because cold lateral
compaction in straight canals is much easier and yields
better results than in curved canals.
Thus, future studies with larger sample sizes are required
to compare these two methods in curved canals. Collins
etal. (2006) compared warm and cold lateral compaction
and warm vertical condensation and concluded that warm
lateral compaction signi cantly increases the volume of
gutta-percha mass in the canal compared to cold lateral
compaction. Difference between our results and theirs
may be due to different methodology since we performed
area-metric analysis while they used replication of canal
irregularity. Moreover, they used D11T spreader in their
study, which is very ne and made of stainless steel, and
can penetrate to 1mm of the working length while we used
nger spreader penetrated to 2mm of the working length.
Moreover, they used non-standard MF gutta-percha while
we used standard cones with 2% taper.
Several methods are available for assessment of the
quality of root canal lling such as dye penetration
(McRobert etal. 997), microbial leakage models, repli-
cation of canal irregularity (Jacobson etal. 2008) and
three-dimensional analysis by micro-computed tomog-
raphy (CT) (Hammad etal. 2009). These methods have
advantages and limitations. Dye penetration and micro-
bial leakage are more commonly used due to simplic-
ity and acceptable accuracy; however, smaller size of
dye particles than some bacteria (Nielsen et al. 1995)
and complexity and time consuming nature of microbial
leakage (Sequeira etal. 2000) are among the drawbacks
of these techniques.
Area-metric analysis has been used by many research-
ers for assessment of the success of endodontic treat-
ment in vitro. Thus, this method was used in our study.
The limitations of this method include two-dimensional
analysis of the root canal lling and lower accuracy
than micro-CT. Moreover, dentin chips and smear layer
created during sectioning in this method may decrease
the quality of images and cause erroneous determina-
tion of borders between gutta-percha, sealer and voids.
To overcome this limitation, we immersed the slices in
sodium hypochlorite solution for one minute after sec-
tioning followed by one minute in 17% EDTA and then
rinsed them to eliminate the smear layer and dentin
chips. Considering the higher accuracy of micro-CT for
three-dimensional assessment of quality of obturation,
further studies with the use of micro-CT on both straight
and curved canals are required to obtain more accurate
information on this topic.
CONCLUSION
Root canal obturation with non-standard accessory
cones and a master cone with 4% taper decreases the
gutta-percha mass and increases the sealer area and
therefore, compromises the quality of root canal lling.
Use of a master cone with 4% taper has no positive effect
on quality of obturation or working time. Warm lateral
compaction in straight canals has no superiority over
cold lateral compaction and takes longer to accomplish.
REFERENCES
Al-Hadlaq SM, Al-Jamhan A, Alsaeed T. (2010) Comparison of
the single cone and lateral compaction techniques in sealing
0.04 taper root canal preparation. Gen Dent 58:219-22.
Aqrabawi JA. (2006) Outcome of endodontic treatment of teeth
lled using lateral condensation versus vertical compaction. J
Contempt Dent Pract 7:17.

Yazdan Shantiaee etal.
578 AREA-METRIC ANALYSIS OF THE QUALITY OF OBTURATION OF FOUR DIFFERENT TECHNIQUES BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
Bal AS, Hicks ML, Barnett F. (2001) Comparison of laterally
condensed 0.06 and 0.02 tapered gutta-percha and sealer in
vitro. J Endod 27:786-8.
Cailleteau JG, Mullaney TP. (1997) Prevalence of teaching api-
cal patency and various instrumentation and obturation tech-
niques in united states dental schools. J Endod 23:394.
Collins J, Walker MP, Kulild J, Lee C.A comparison of three
gutta-percha obturation techniques to replicate canal irregu-
larities. J Endod 2006;8:762-5.
Gilhooly RM, Hayes SJ, Bryant ST, Dummer PM. (2001) Com-
pacted of lateral condensation and thermomechanically com-
pacted warm alpha-phase gutta-percha with a single cone for
obturating curved root canals. Oral Surg Oral Med Oral Pathol
Oral Radiol Oral Endod 91:89.
Gordon MPJ, Love R, Chandler NP. (2005) An evaluation of
0.06 tapered gutta-percha cones for lling of 0.06 taper pre-
pared curved root canals. Int Endod J38:87-96.
Haikei Y, Freymann M, Fanti V, Claisse A, Poumier F, Wat-
son M. (2006) Apical microleakage of radiolabeled lysozyme
over time in three techniques of root canal obturation. J Endod
26:148-52.
Hammad M, Qualtrough A, Silikas N. (2009) Evaluation of root
canal obturation: a three dimensional in vitro study. J Endod
35:541-4.
Jacobsen EL, Begole EA.( 1992) A Comparison of four canal
obturation methods employing gutta-percha: a computerized
analysis of the internal structure. Endod Dent Traumatol 8:206.
Jacobson HLJ, Xia T, Mini-Kai W, Paul RW. (2008) Sealing
ability of a new polydimethylsiloxane-based root canal lling
materials. J Endod 34:204-7.
Jarret IS, Marx D, Covey D, Karmazin M, Lavin M, Gound T.
(2004) Percentage of canals lled in apical cross sections. Int
Endod J 37:392-8.
Kazemi RB, Safavi KE, Spangberg LSW. (1993) Dimensional
changes of endodontic sealers. Oral Surg Oral Med Oral Pathol
76:766-71.
Kojima K, Inamoto K, Nagamatsu K. (2004) Success rate of
endodontic treatment of teeth with vital and non-vital pulps:
a meta-analysis. Oral Surg Oral Med Oral Pathol Oral Radiol
Oral Endod 97:5-9.
Kontakiotis EG, Wu MK, Wesselink PR.( 1997) Effect of sealer
thickness on long-term sealing ability: a 2-year following
study. Int Endod J 30:307-12.
Lee AH, Cheung GS, Wong MC. (2012) Long term outcome
of primery non-surgical root canal treatment. Clin Oral Invest
16:1607-17.
McRobert AS, Lumley PJ. An in vitro investigation of coronal
leakage with three gutta-percha back lling techniques. Int
Endod J 1997;30:413-7.
Michaud R, Burgess J, Bar eld R, Cakir D, McNeal S, Eleazer P.
(2008) Volumetric expansion of gutta-percha in contact with
eugenol. J Endod 34:1528-32.
Mollander A, Reit C, Dahlen G, Kvist T. (1998) Microbiological
status of root- lled teeth with apical periodontitis. Int Endod
J31:1-7
Ng YL, Mann V, Rahbaran S. (2008) Outcome of primery root
canal treatment: systematic review of the literature. Int Endod
J 41:6-31.
Ng YL, Mnn V, Rahbaran S, Lewsey J, Gulabivala K. (2007)
Outcome of primery root canal treatment: systematic review of
the literature. Int Endod J 40:921.
Nica LM, Didilescu A, Rusu D, Bacila A, Stratul SI. (2012) Pho-
tomicrographic evaluation of the apical sealing capacity of
three types of gutta-percha master cones: an in vitro study.
Odontology 100:54-60.
Nielsen RB, Alyassin AM, Peters DD. (1995) Micro computed
tomography: an advanced system for detailed endodontic
research. J Endod 21:561.
Raina R, Loushine RJ, Weller RN, Tay FR, Pashley DH. (2007)
Evaluation of the quality of the apical seal in Resilon/Epiph-
any and gutta-percha/AH plus- lled root canal by using uid
ltration approach. J Endod 33:944-7.
Romina C, Beltes P, Boutsionkis C, Dandakis C. (2009) Ex-vivo
area-metric analysis of root canal obturation using gutta-per-
cha cones of different tapers. Int Endod J 42:491-8.
Schaeffer MA, White RR, Walton RE. (2005) Determining the
optimal obturation length: a meta-analysis of literature. J
Endod 31:271-4.
Schafer E, Koster M, Burklein S. (2013) Percentage of gutta-
percha lled areas in canals instrumented with NiTi sys-
tems and obturated with matching single cones. J Endod 39:
924-4.
Schafer E, Neilus B, Burklein S. (2012P) A comparative evalua-
tion of gutta-percha lled area in curved root canals obturated
with different techniques. Clin Oral Invest 16:225-30.
Schafer E, Schrenker C, Zupanc J, Burklein S. (2016) Percent-
age of gutta-percha lledarea in canals obturated with cross-
linked gutta-percha core-carrier systems, single-cone and lat-
eral compaction technique. J Endod 2:294-8.
Sequeira JF, Rocas IN, Favieri A, Amad EC, Castro AJR, Gahyva
SM. (2000) Bacterial leakage in coronaly unsealed root canals
obturated with 3 different techniques. Oral Surg Oral Med Oral
Pathol 90:647-50.
Skinner RL, Himel VT. (1987) The sealing ability of injection-
modeled thermoplasticized gutta-percha with and without the
use of sealers. J Endod 13:315.
VanGheluwe J, Wilcox LR. (1996) Lateral condensation of
small curved root canals root canals: comparison of two types
of accessory cones. J Endod 22:540-42.
Whitworth J. Methods of lling root canals: principles and
practices. Endod Topics. 2005;12:2-24.
Wilson J, Baumgartner JC. (2003) Comparison of spreader
penetration during lateral compaction of 0.04 and 0.02 gutta-
percha. J Endod 29:828-31.

Yazdan Shantiaee etal.
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS AREA-METRIC ANALYSIS OF THE QUALITY OF OBTURATION OF FOUR DIFFERENT TECHNIQUES 579
Wu MK, Bud MG, Wesselink PR. (2009) The quality of single
cone and laterally compacted gutta-percha llings in small
and curved root canals as evidenced by bidirectional radio-
graphs and uid transport measurements. Oral Surg Oral Med
Oral Pathol Oral Radiol Endod 108:946-51.
Wu MK, Kast Akora A, Wesselink PR. (2002) Quality of cold
and warm gutta-percha llings in oval canals in mandibular
premolars. Int Endod J34: 485-91.
Wu MK, Wesselink PR. (1993) Endodontic leakage studies recon-
sidered methodology, application and relevance. Int Endod J26:37.