
Biotechnological
Communication
Biosci. Biotech. Res. Comm. 10(3): 557-563 (2017)
Assessment of location of anterior ethmoidal artery using
cone beam computed tomography (CBCT)
Shima Javdan
1
, Roshanak Ghaffari
2*
and Saeed Sohilipour
3
1
Postgraduate Student, Department of Oral Radiology, Dental School, Islamic Azad University, Isfahan
Khorasgan Branch Isfahan Iran
2
Department of Oral and Maxillofacial Radiology, Dental Faculty, Isfahan Khorasgan Branch, Islamic Azad
University
3
Otolaryngology, Isfahan University of Medical Sciences, Isfahan, Iran
ABSTRACT
Anterior ethmoidal artery (AEA) is an important landmark, which may be accidentally injured or traumatized during
surgical procedures. This study aimed to determine the position of AEA on CBCTscans. In this descriptive analytical
study, CBCT scans of 129 patients evaluated. The mean distance from AEA to anterior base of the skull, posterior
frontal sinus wall, nasion, anterior nasal spine (ANS), orbital roof, inferior turbinate and the mean angle between
AEA and ANS were evaluated using SIDEXIS 3D software. Independent and paired t-test and Fisher’s test were used
for statistical analyses with P<0.05 level of signi cance. The mean distance from AEA was 11.60±1.94 mm to orbital
roof, 32.66±4.33 mm to inferior turbinate, 8.96±4.51 to posterior wall of the frontal sinus, 2.09 ±2.18mm to the
anterior base of the skull, 18.01±3.90 mm to the nasion and 58.69±4.24 mm to the ANS. The angle between AEA
and NS was 55.15±4.36°. The distances from AEA to orbital roof, inferior turbinate, nasion and ANS in men were
signi cantly greater than those in women (P<0.05). nasion. ( = 0/05) Surgical procedures in areas close to AEA are
high-risk. Determination of the position of AEA prior to endoscopic surgery of the sinus is highly important. CBCT
can help determine the location of AEA prior to surgery to prevent unwanted surgical complications.
KEY WORDS: CONE-BEAM COMPUTED TOMOGRAPHY; ETHMOID; ARTERY
557
ARTICLE INFORMATION:
*Corresponding Author: Roshanak Ghaffari
Received 23
rd
June, 2017
Accepted after revision 26
th
Sep, 2017
BBRC Print ISSN: 0974-6455
Online ISSN: 2321-4007 CODEN: USA BBRCBA
Thomson Reuters ISI ESC and Crossref Indexed Journal
NAAS Journal Score 2017: 4.31 Cosmos IF: 4.006
© A Society of Science and Nature Publication, 2017. All rights
reserved.
Online Contents Available at:
http//www.bbrc.in/
DOI: 10.21786/bbrc/10.3/33
558 ASSESSMENT OF LOCATION OF ANTERIOR ETHMOIDAL ARTERY USING (CBCT) BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
Javdan, Ghaffari and Sohilipour
INTRODUCTION
In ammatory diseases of paranasal sinuses are a com-
mon serious problem. In the recent decades, functional
endoscopic sinus surgery (FESS) has revolutionized
surgical treatment of paranasal sinuses. In this tech-
nique, due to the proximity of paranasal sinuses to
some important structures such as anterior base of skull,
orbit and ethmoidal artery, unintentional injury to these
anatomical structures may cause serious complications
(Basak et al. 1998). Anterior ethmoidal artery (AEA) is
an important landmark, which may be accidentally trau-
matized or injured during surgical procedure of anterior
ethmoidal sinus. Injury to AEA may cause severe nasal
bleeding, intra-orbital hemorrhage, posterior orbital
hematoma, spinal uid leak and intracranial bleeding in
rare cases (Ding et al. 2012 Eren et al. 2016).
In FESS, superior lateral border of AEA and its infe-
rior border in contact with inferior turbinate are marked
(Rontal et al. 1991). The distance between AEA and the
contact area with the inferior turbinate outlines the safe
area for surgical manipulation. Since in FESS the width
of ethmoid forceps is maximally 10mm when opened, the
surgeon must have adequate knowledge about the space
limitations in this area (Rontal et al. 1991; Basak et al.
1998). Knowledge about the anatomical location of AEA
and its detection on images can help prevent unwanted
complications during surgery (Ding et al. 2012). AEA
is among the most important reference landmarks for
endoscopic surgery since it determines the posterior
location of recess. Its detection in frontoethmoidal
suture determines the location of anterior base of skull
(Monjas-Cánovas et al. 2012; Ko et al. 2014).
Ethmoidal artery originates from the orbital artery.
Some branches of ethmoidal artery originate from
supraclinoid portion of the internal carotid artery and
pass through the optical foramen towards the orbit in
a lateral position. In coronal plane, a conical groove in
the medial orbital wall may be seen, which indicates
the exit point of ethmoidal artery between the superior
oblique muscle and medial rectus muscle. It indicates
anterior ethmoidal foramen and can serve as a refer-
ence anatomical landmark to determine the location of
AEA (Monjas-Cánovas et al. 2012). The location of AEA
relative to the ethmoidal air cells may be variable but it
is often located between the second and third lamellae
next to basal lamella (Ding et al. 2012).
Ko et al, in 2014 evaluated the ef cacy of AEA to
determine the location of frontal sinus in endoscopic
sinus surgery using computed tomography (CT) and
offered a classi cation for the position of AE. Guldner et
al. provided a similar classi cation in 2012 using CBCT
(Guldner et al. 2012). At present, CBCT is increasingly
used for implant imaging and endodontic treatments
and is a new technique in ENT for assessment of sinuses.
It is superior to CT since it has lower cost and lower
patient radiation dose compared to CT. Studies on deter-
mination of location of AEA using CBCT are limited.
Thus, this study has aimed to determine the position of
AEA on CBCT scans.
MATERIALS AND METHODS
This descriptive analytical study was conducted on 129
CBCT scans of patients (70 females and 59 males) over
18 years of age presenting to the Oral and Maxillofacial
Radiology Department of Isfahan University of Medi-
cal Sciences, School of Dentistry. All CBCT scans had
been taken with one CBCT unit (Galileos-Sirona Ben-
sheim, Germany) with the exposure settings of 85 kVp
and 21-35 mAs (depending on the patient’s weight). The
inclusion criterion was age over 18 years. The exclusion
criteria were history of surgery or trauma to parana-
sal sinuses and skull base, congenital facial anomalies,
malignancies or lesions causing opacity of frontal recess
and anterior ethmoidal cells. Multiplanar (coronal, sag-
ittal and oblique sagittal) reconstructed images were
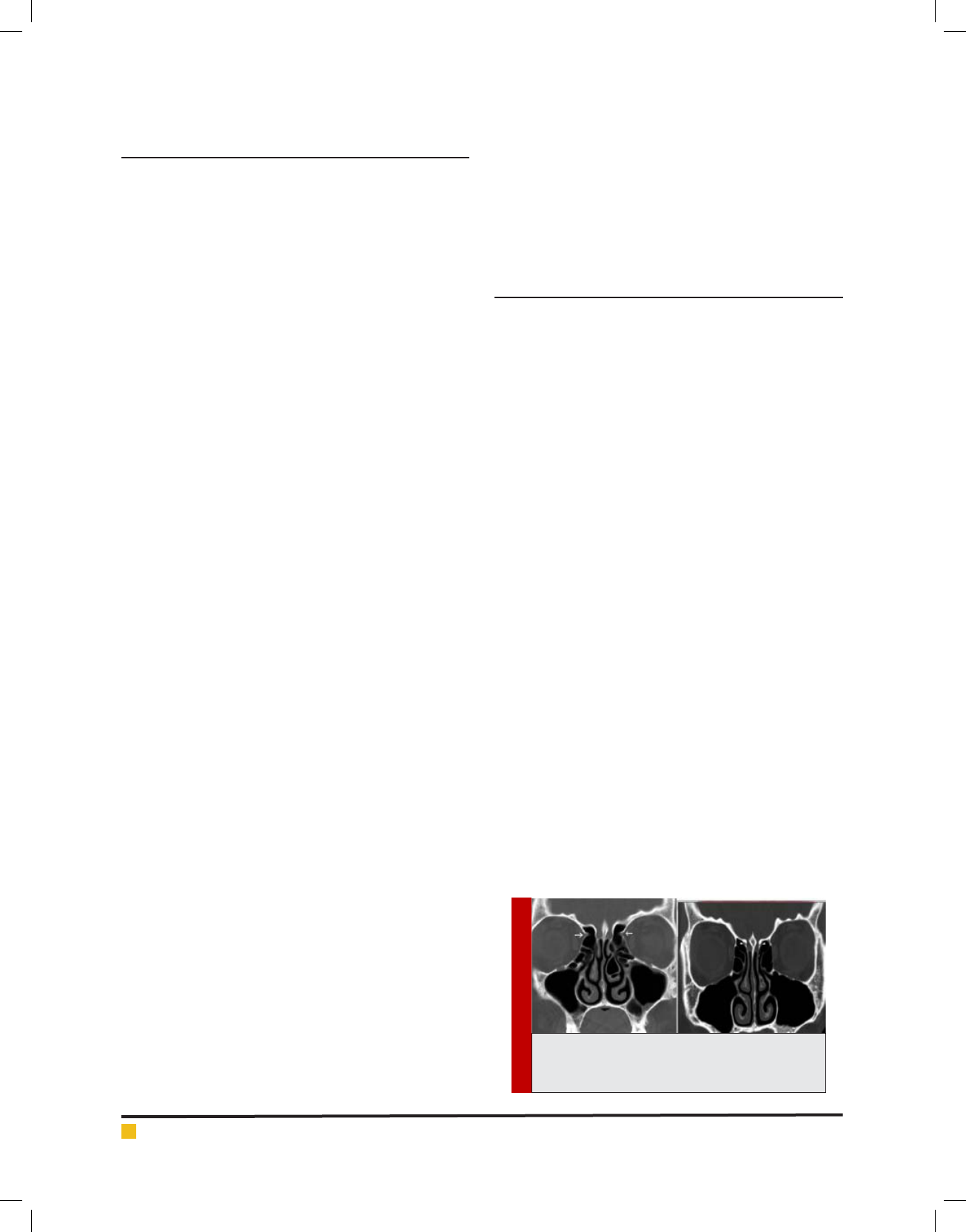
assessed using SIDEXIS 3D software. Next, notch in the
medial orbital wall and bony sulcus of lateral wall of the
olfactory fossa (anterior ethmoidal sulcus) on coronal
sections which indicate the anterior ethmoidal foramen
were used for detection of the AEA (Figure 1).
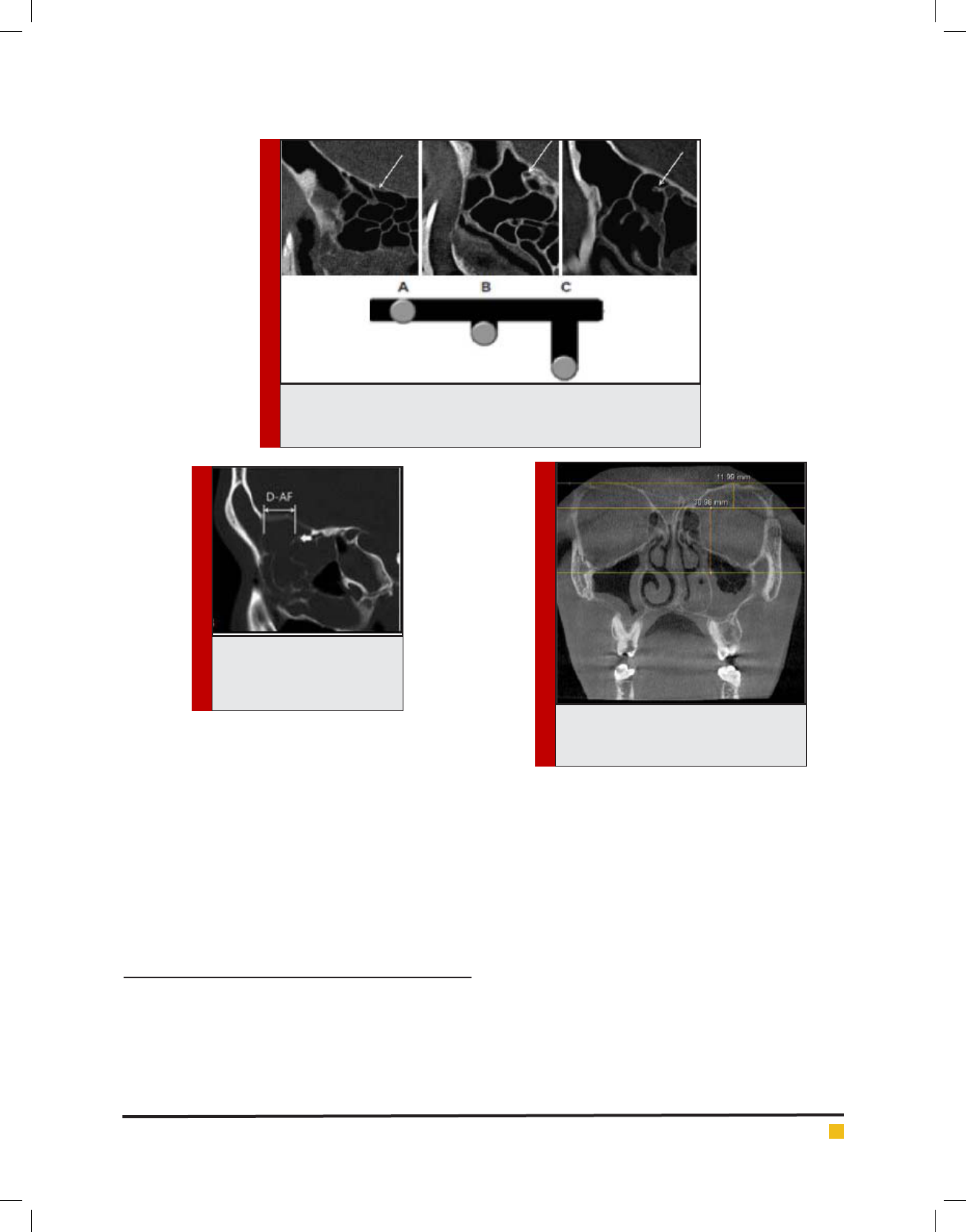
Due to the presence of variations in the path of artery,
distance from the artery to the base of skull was meas-
ured. In type I, the entry point of AEA is adjacent to the
anterior base of the skull. In type II, it has less than 1mm
distance from the base of the skull. In type III, AEA has a
distance equal or more than 1mm from the anterior base
of the skull (Guldner et al. 2012) (Figure 2). To determine
the position of AEA relative to the frontal sinus in the
sagittal plane, distance from the AEA to the posterior
wall of the frontal sinus was measured (Monjas-Cánovas
et al. 2011) (Figure 3). Distance from the AEA to the
orbital roof and inferior turbinate (site of attachment
FIGURE 1. Anterior ethmoidal foramen notch
in the medial orbital wall (arrow) and anterior
ethmoidal sulcus (arrow head)
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS ASSESSMENT OF LOCATION OF ANTERIOR ETHMOIDAL ARTERY USING (CBCT) 559
Javdan, Ghaffari and Sohilipour
FIGURE 2. Location of the AEA on the sagittal plane (up). Schematic
views (down): (A) Attached to the base of skull; (B) distance less than 1
mm; (C) distance of 1 mm or more
FIGURE 3. Distance from the
anterior ethmoidal foramen to
the posterior wall of the frontal
sinus on the sagittal plane
FIGURE 4. Distance from the anterior
ethmoidal foramen to the orbital roof and
inferior turbinate
of bony lamella of inferior concha with medial wall of
the maxillary sinus) in the coronal plane (Figure 4) was
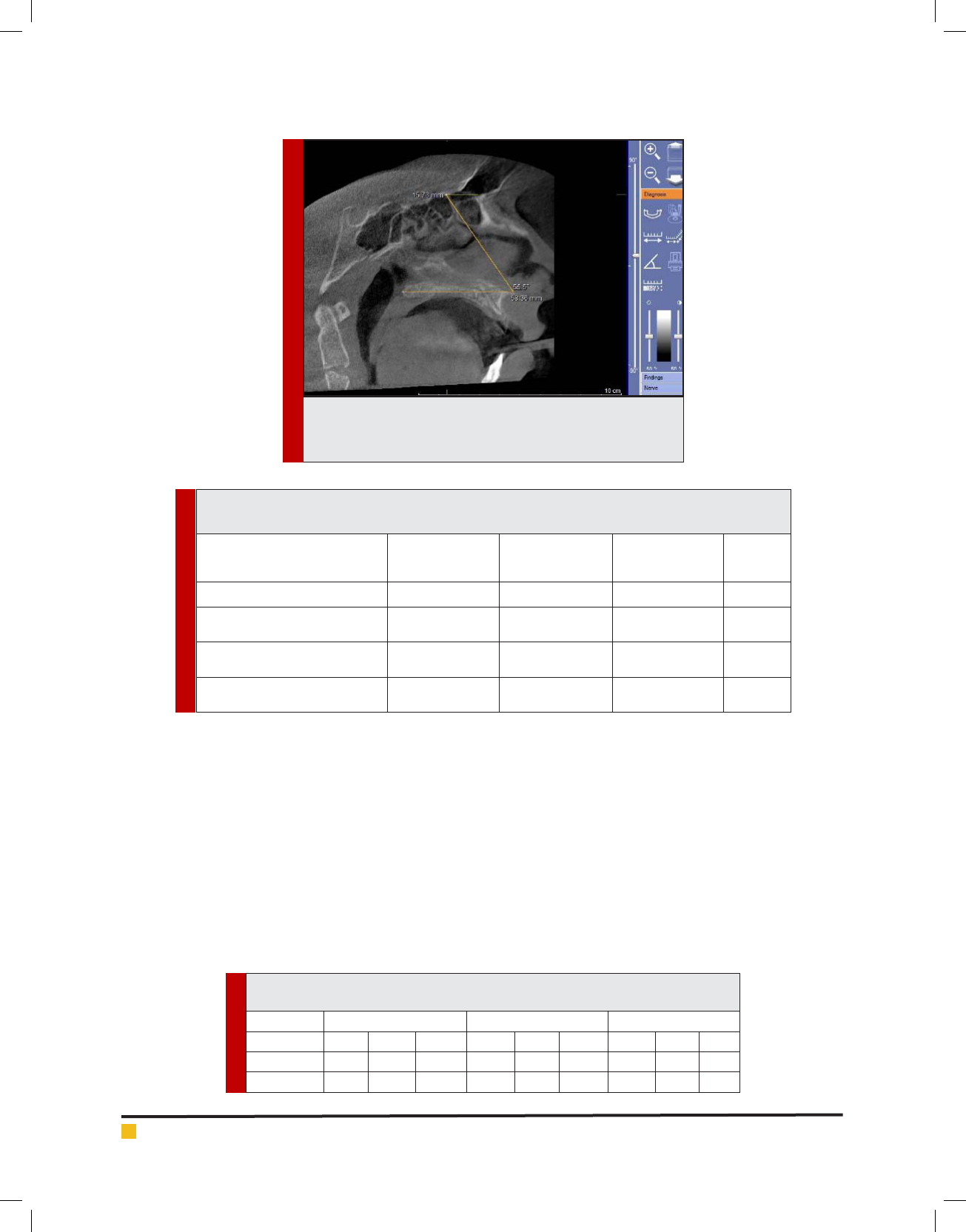
measured. To estimate the distance from the AEA to the
nasion and also the distance from the AEA to the ANS,
the oblique sagittal plane was used. In this plane, the
angle between the hypothetical line connecting the AEA
and ANS and horizontal line passing through the hard
palate and ANS was measured (Monjas-Canovas et al.
2011) (Figure 5). Independent and paired t-test were used
for statistical analyses. P<0.05 was considered statisti-
cally signi cant.
RESULTS AND DISCUSSION
A total of 129 patients (59 males and 70 females) with
a mean age of 41.59 years in males and 38.44 years in
females were evaluated. Both sides were evaluated in
each patient (n=258). Independent t-test showed that the
mean age of males and females was not signi cantly
different (P=0.220). In most cases, the AEA was detect-
able on coronal sections of the anterior ethmoidal fora-
men in the medial wall of the orbit (96.1%) in the form
of a notch and anterior ethmoidal sulcus in the lateral
wall of the olfactory fossa (94.2%). The Fisher’s exact
test showed that the frequency distribution of pres-
ence of the AEA in the medial orbital wall and ante-
rior ethmoidal sulcus was not signi cantly different in
the right and left sides (P>0.05).The mean total distance
from the AEA to the orbital roof on coronal sections was
11.601.94mm. This distance to the inferior turbinate
was 32.664.33mm. As seen in Table 1, t-test showed
no signi cant difference between the distance from the
AEA to the orbital roof and to the inferior turbinate in
the two sides (P>0.05). The mean distance from the AEA
to the posterior frontal sinus wall (8.964.51mm) and
anterior base of the skull (2.092.18mm) on sagittal sec-
tions is shown in Table 1; according to t-test, the differ-
560 ASSESSMENT OF LOCATION OF ANTERIOR ETHMOIDAL ARTERY USING (CBCT) BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
Javdan, Ghaffari and Sohilipour
FIGURE 5. Distance from the AEA to the nasion and ANS; angle
between the AEA and ANS and hard palate plane on oblique sag-
ittal plane
Table 1. Mean distance from the AEA to the orbital roof, inferior turbinate, posterior wall of the frontal
sinus and anterior base of the skull in millimeters
Distances
Right (mean±SD)
mm
Left (mean±SD)
mm
Total (mean±SD)
Mm
P value
Distance from AEA to orbital roof 11.73±2.03 11.48±1.85 11.60±1.94 0.13
Distance from AEA to inferior
turbinate
32.42±4.46 32.90±4.21 32.66±4.33
0.20
Distance from AEA to posterior
wall of frontal sinus
8.66±4.46 9.27±4.56 8.96±4.51
0.11
Distance from AEA to anterior base
of skull
2.10±2.27 2.07±2.09 2.09±2.18
0.81
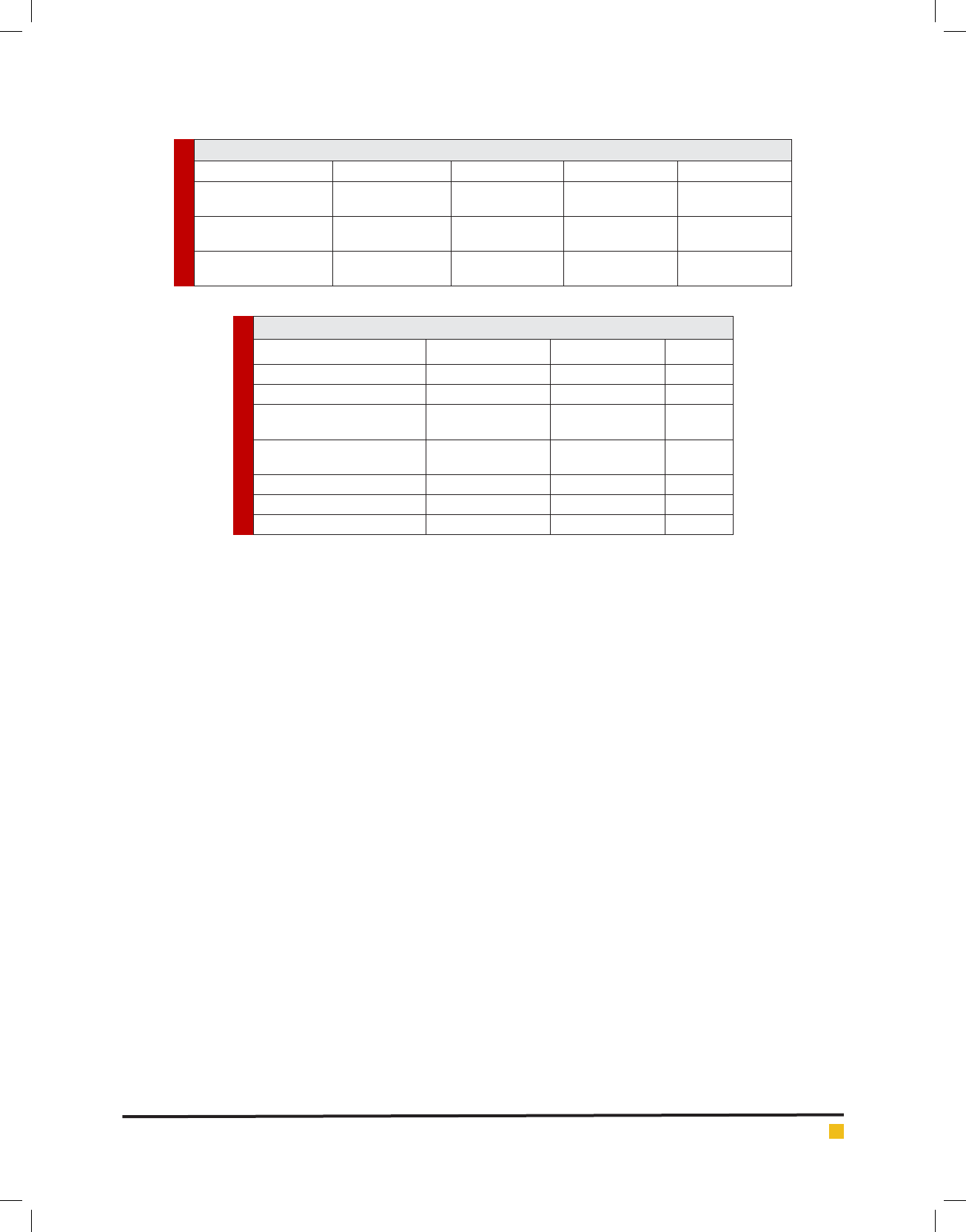
Table 2. Location of AEA relative to the anterior base of the skull on CBCT sagittal
sections in millimeters
Right Left Total
0 <1 ≥1 0 <1 ≥1 0 <1 ≥1
Number 58 1 70 50 2 77 108 3 147
Percentage 45% 8% 54.3% 38.8% 1.6% 59.7% 41.9% 1.2% 57%
ence in the mean distance from the AEA to the posterior
wall of the frontal sinus and anterior base of the skull
was not signi cant (P>0.05).
Table 2 shows the position of the AEA relative to the
anterior base of the skull on sagittal CBCT sections based
on the presented classi cation.
Table 3 shows the mean distance from the AEA rela-
tive to the nasion and ANS and angle of AEA relative
to ANS in oblique sagittal plane. As seen in Table 3,
according to paired t-test, no signi cant difference was
noted in the mean variables in the right and left sides
(P>0.05).
As demonstrated in Table 4, independent t-test
showed that the distance from the AEA to the orbital
roof and inferior turbinate and distance from the AEA to
the nasion and ANS in males were signi cantly greater
than those in females (P<0.05) but no signi cant differ-
ence was noted between males and females in the AEA
and ANS angle (P>0.05).
Many anatomical studies have assessed the location
of the AEA and most of them used endoscopic meas-
urements while some others used CT (Monjas-Canovas
et al. 2012). On the other hand, studies on detection of
AEA on CBCT scans are limited (Guldner et al. 2012).
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS ASSESSMENT OF LOCATION OF ANTERIOR ETHMOIDAL ARTERY USING (CBCT) 561
Javdan, Ghaffari and Sohilipour
Table 3. Mean distance from the AEA to the nasion, ANS and AEA-ANS angle on oblique sagittal plane
Right (mean±SD) Left (mean±SD) Total (mean±SD) P value
Distance between AEA
and nasion
18.04±3.61 mm 17.95±4.17 mm 18.01±3.90 mm 0.78
Distance between AEA
and ANS
58.58±4.09 mm 58.81±4.40 mm 58.69±4.24 mm 0.21
Angle between AEA and
ANS
55.06±4.16 º 55.24±4.56 º 55.15±4.36º 0.53
Table 4. Mean and standard deviation of data based on gender
Distance Female (mean±SD) Male (mean±SD) P value
Distance to orbital Roof 11.97±1.80 mm 11.17±2.01 mm 0.001
Distance to inferior turbinate 31.51±4.27 mm 34.03±4.02 mm 0.000
Distance to anterior base of
skull
2.17±2.12 mm 1.99±2.25 mm 0.50
Distance to inferior wall of
frontal sinus
8.56±3.83 mm 9.44±5.18 mm 0.132
Distance to nasion 17.25±3.28 mm 18.91±4.38 mm 0.01
Distance to ANS 56.46±3.33 mm 61.33±3.66 mm 0.00
Angle between AEA and ANS 55.44±4.06º 54.79±4.69º 0.23
The AEA passes through three cavities namely the orbit,
the ethmoidal labyrinth and the anterior cranial fossa.
The AEA enters into the olfactory fossa from the anterior
cranial base and then enters into the anterior ethmoi-
dal sulcus through the lateral lamella of the cribriform
plate, which is the weakest point of the anterior base of
the skull. At this point, bone is dangerously thin and it
is considered a high-risk area in nasal endoscopic sur-
gery. Thus, the AEA is susceptible to traumatization and
injury during surgical procedures (Stammberger et al.
1990; Bayram et al. 2001; Moon et al. 2001; White et al.
2005; Araujo Filho et al. 2006; Souza et al. 2009).
In most cases in our study, this artery was detect-
able in the medial wall of the orbit (96.1%) and lateral
wall of the olfactory fossa (94.2%). Similarly, Souza et
al. detected AEA in the medial orbital wall (98%) and
lateral wall of the olfactory fossa (100%) and stated that
medial notch of the orbit and medial ethmoidal sulcus
were reliable landmarks for detection of the AEA (Souza
et al. 2009). Gotwald et al, similarly detected the orbital
medial notch on coronal CT scans in 95% and medial
ethmoidal sulcus in 84% of cases (Gotwald et al. 2004).
Ding et al. used CT angiography and detected AEA in
100% of the cases in the notch in the medial orbital
wall and in 98.4% in the ethmoidal sulcus (Ding et al.
2012). Considering the invasiveness of CT angiography
and high dose of CT, low dose CBCT is more suitable for
detection of AEA. In FESS, superior lateral border of the
surgical site is determined based on the location of AEA
and the inferior border is determined by the inferior tur-
binate (Rontal et al. 1991). Distance from the AEA to
the attachment site of the inferior turbinate determines
the suitable location for surgical procedure. Basak et al.
considered the orbit as a xed reference point and based
on this point, they determined the location of AEA.
The mean distance from the AEA to the orbital roof
on CT scans was reported to be 13.7 mm (Basak et al.
1998) while in our study, this distance was found to be
11.601.94 mm. Basak et al. measured the mean distance
from the AEA to the inferior turbinate to be 30.05 mm
(Basak et al. 1998) and Eren et al. found this distance to
be 31.6 mm on CT scans (Eren et al. 2016); these values
were close to our ndings (32.664.33 mm).
The distance from the AEA to the skull base is impor-
tant because when AEA with mesenterium is located
right beneath the skull, it has higher risk of traumatiza-
tion during surgery. Basak et al. evaluated the location
of AEA on coronal CT scans and reported that it was
adjacent to the skull base in 57% of the cases and had
a distance from it in 43%. In cases where AEA has a
distance from the base of skull, risk of traumatization
during FESS is higher (Basak et al. 1998). Moon et al.
assessed both sagittal sections and cadaver dissection
and reported that in 85.7% of cases, AEA was adjacent
to the skull base; in the remaining cases, AEA had 2-3
mm distance from the skull base (Moon et al. 2001).
Guldner et al. (2012) reported similar results. Araujo et
al. reported that AEA was attached to the skull base in
83.3% of the cases (Araujo Filho et al. 2006). Kainz and
Stammberger reported that in most cases, AEA had 5
Javdan, Ghaffari and Sohilipour
562 ASSESSMENT OF LOCATION OF ANTERIOR ETHMOIDAL ARTERY USING (CBCT) BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
mm distance from the skull base. They also stated that
when the roof of ethmoidal sinus is low, anterior ethmoi-
dal canal may be attached to the skull base (Kainz et al.
1988). The same was stated by Becker et al, who deter-
mined the location of foramen in endoscopic sections.
Jang et al. reported this distance to be 1.32 1.51mm
on CT scans (Jang et al. 2014) while in our study, this
distance was 2.09 2.18mm. These differences may be
due to racial differences or surgical technique. It seems
that in patients with larger supraorbital ethmoid cell and
optimal pneumatization of ethmoidal sinus (Jang et al.
2014), AEA is located right beneath the skull base; oth-
erwise, it is at the same level of the skull base (Lisbona
et al. 2010).
Young et al, in their study measured the distance
from the AEA to the base of skull and categorized it in
three groups of no distance [16%], distance less than 1
mm (33.7%) and equal or higher than 1 mm (50.5%) (Ko
et al. 2014). In our study, 41.9% were categorized in no
distance group, 1.2% were categorized in less than 1 mm
group and 57% were categorized in 1 mm and higher
group. In most cases in both studies, the distance from
the AEA to the skull base was equal or more than 1 mm.
Frontal sinus is the most challenging sinus in endo-
scopic surgery due to its anatomical complexity and
variations. Many studies have suggested anatomical
landmarks to help the surgeon in safe conduction of
frontal sinus surgery (McLaughlin et a;. 1997; Lee et al.
1997; Kew et al. 2002). The AEA is known as a typical
classic reference point for the frontal sinus. Some stud-
ies showed that AEA is located right behind the fron-
tal recess and can serve as an anatomical landmark for
frontal sinus surgery (White et al. 2005). Thus, knowl-
edge about the anatomy of this area is important and
must be obtained prior to endoscopic sinus surgery.
Young et al. reported the mean distance from the AEA
to the posterior wall of the frontal sinus to be 8.585.56
mm, which was in line with our result (8.964.51 mm);
whereas, Jang et al. measured the distance from the AEA
to the anterior wall of the frontal sinus to be 17.362.19
mm [19]; this difference was due to the different refer-
ence points selected. Statistically, similar to our study,
Young et al. found no signi cant association between
the distance from the AEA to the frontal sinus and AEA
to the base of skull (Ko et al. 2014).
In endoscopic surgery of the sinus, zero degree ANS
angle complicates the detection of AEA [9]. Donemez et
al. considered ANS as a xed landmark and measured its
distance from the AEA on cadavers using an electronic
caliper, and reported the value to be 553 mm (Donmez
et al. 2005). However, Monjas-Cánovas et al. measured
the distance from the AEA to ANS to be 55.515.52 mm
and measured its angle with the horizontal line passing
through the ANS to be 57.71.78; these values were
close to those of Moon et al.(2001), Lee et al. (2000)
and Araujo et al. (2006). Our study reported this distance
to be 58.694.26 mm and the angle was 55.144.37,
which was in line with previous studies. Araujo et al.
(2014) reported that the distance from the AEA to ANS
was signi cantly greater in males than in females; this
difference was not statistically signi cant in our study
and that of Lee et al. (2000).
Nasion is used as a reference point in CT scan stud-
ies for surgical resection of some tumors or manage-
ment of uncontrollable arterial hemorrhage, which is
endoscopically impossible; although external incision is
made from the canthus and not directly on the nasion.
Monjas-Cánovas et al. measured the mean distance from
the AEA to the nasion to be 29.312.5 mm (2011), which
is similar to the study by Cankal et al. (2004); whereas,
the results of Eren et al. (2014)(17.993.91) were closer
to ours (18.013.90 mm). In our study, a weak but signif-
icant association was noted between the distance from
the AEA to the ANS and the distance from the AEA to
the nasion; whereas, Eren et al. (2014) found a signi -
cant association between the distance from the AEA to
the nasion and the distance from the AEA to the inferior
turbinate (Eren et al. 2014).
CONCLUSION
Inadequate knowledge about the anatomy of surgical
site can cause serious iatrogenic surgical complications.
To decrease these risks, a careful dissection must be done
after thorough assessment of the area on CBCT scans.
Therefore, adequate knowledge about the anatomy of
the area and location of the AEA by use of CBCT can be
helpful prior to FESS.
REFERENCES
Araujo Filho BC, Weber R, Pinheiro Neto CD, Lessa MM,
Voegels RL, Butugan O. (2006) Endoscopic anatomy of the
anterior ethmoidal artery: a cadaveric dissection study. Braz J
Otorhinolaryngol 72(3):303-8.
Basak S, Karaman CZ, Akdilli A, Mutlu C, Odabasi O, Erpek
G. (1998) Evaluation of some important anatomical variations
and dangerous areas of the paranasal sinuses by CT for safer
endonasal surgery. Rhinology 36(4):162-7.
Bayram M, Sirikci A, Bayazit YA. (2001) Important anatomic
variations of the sinonasal anatomy in light of endoscopic sur-
gery: a pictorial review. Eur Radiol 11(10):1991-7.
Becker SP. (1994) Applied anatomy of the paranasal sinuses
with e9mphasis on endoscopic surgery. The Annals of otology,
rhinology & laryngology Supplement 162:3
Cankal F, Apaydin N, Acar HI, Elhan A, Tekdemir I, Yurdakul
M, et al. (2004) Evaluation of the anterior and posterior

Javdan, Ghaffari and Sohilipour
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS ASSESSMENT OF LOCATION OF ANTERIOR ETHMOIDAL ARTERY USING (CBCT) 563
ethmoidal canal by computed tomography. Clinical radiology
59(11):1034-40.
Ding j, Sun G, Lu Y, Yu B-b, Li M, Li L, et al. (2012) Evalua-
tion of Anterior Ethmoidal Artery by 320-Slice CT Angiog-
raphy with Comparison to Three-Dimensional Spin Digital
Subtraction Angiography . Initial Experiences, Korean J Radiol
13(6):667-73.
Donmez BO, Agirdir BV, Sindel MM. (2005) Important anatom-
ical landmarks in the lateral nasal wall. Saudi medical journal
26(9):1403-8.
Eren E, Altay C, Arslanoglu S, Erdogan NK, Uluc ME, Onal K, et
al. (2014) Searching for the cheese: does ethmoid pneumatiza-
tion affect the location of the anterior ethmoid artery? EUFOS :
af liated with the German Society for Oto-Rhino-Laryngology
- Head and Neck Surgery 271(2):281-5.
Gotwald TF, Menzler A, Beauchamp NJ, zur Nedden D, Zinre-
ich SJ. (2003) Paranasal and orbital anatomy revisited: iden-
ti cation of the ethmoid arteries on coronal CT scans. Critical
reviews in computed tomography 44(5):263-78.
Guldner C, P.Zimmermann A, Diogo I, Werner JA, Teymoortash
A. (2012) Age-dependent differences of the anterior skull
base. International Journal of Pediatric Otorhinolaryngology
76:822–8.
Jang DW, Lachanas VA, White LC, Kountakis SE. (2014)
Supraorbital ethmoid cell: a consistent landmark for endo-
scopic identi cation of the anterior ethmoidal artery. Otolar-
yngology-head and neck surgery : of cial journal of Ameri-
can Academy of Otolaryngology-Head and Neck Surgery
151(6):1073-7.
Kainz J, Stammberger H. (1988) The roof of the anterior
ethmoid: a locus minoris resistentiae in the skull base. Laryn-
gologie, Rhinologie, Otologie 67(4):142-9.
Kew J, Rees GL, Close D, Sdralis T, Sebben RA, Wormald
PJ. (2002) Multiplanar reconstructed computed tomography
images improves depiction and understanding of the anatomy
of the frontal sinus and recess. American journal of rhinology
16(2):119-23.
Ko Y-B, Kim M-g, Jung YG. (2014) Anatomical Relationship
between the Anterior Ethmoid Artery, Frontal Sinus, and Inter-
vening Air Cells ; Can the Artery Be Useful Landmark? Korean
J Otorhinolaryngol-Head Neck 57(10):687-91.
Lee D, Brody R, Har-El G. (1997) Frontal sinus out ow anat-
omy. American journal of rhinology 11(4): 283- 5.
Lee WC, Ming Ku PK, van Hasselt CA. (2000) New guidelines
for endoscopic localization of the anterior ethmoidal artery: a
cadaveric study. Laryngoscope 110(7):1173-8.
Lisbona Alquezar MP, Fernandez Liesa R, Lorente Munoz A,
Perez Delgado L, Herrera Tolosana S, Tejero-Garces Galve G,
et al. (2010) Anterior ethmoidal artery at ethmoidal labyrinth:
Bibliographical review of anatomical variants and references
for endoscopic surgery. Acta Otorrinolaringol Esp 61(3):202-8.
McLaughlin RB, Jr., Rehl RM, Lanza DC. (2001) Clinically rel-
evant frontal sinus anatomy and physiology. Otolaryngologic
clinics of North America 34(1):1-22.
Monjas-Canovas I, Garcia-Garrigos E, Arenas-Jimenez JJ,
Abarca-Olivas J, Sanchez-Del Campo F, Gras-Albert JR. (2011)
Radiological anatomy of the ethmoidal arteries: CT cadaver
study. Acta Otorrinolaringol Esp 62(5):367-74.
Monjas-Cánovas I, García-Garrigós E, Arenas-Jiménez JJ,
Abarca-Olivas J, Campo Fs-D, Gras-Alberta JR. Radiological
Anatomy of the Ethmoidal Arteries: CT Cadaver Study. Acta
Otorrinolaringol Esp 2011;62(5):367-74.
Moon HJ, Kim HU, Lee JG, Chung IH, Yoon JH. (2001) Surgi-
cal anatomy of the anterior ethmoidal canal in ethmoid roof.
Laryngoscope 111(5):900-4.
Rontal M, Rontal E. (1991) Studying whole-mounted sections
of the paranasal sinuses to understand the complications of
endoscopic sinus surgery. The Laryngoscope 101(4 Pt 1):361-6.
Rontal M, Rontal E. (1991) Studying whole-mounted sections
of the paranasal sinuses to understand the complications of
endoscopic sinus surgery. The Laryngoscope 101(4 Pt 1):361-6.
Souza SA, Souza MMAd, Gregório LC, Ajzen S. (2009) Anterior
Ethmoidal Artery Evaluation on Coronal CT Scans. . Braz J
Otorhinolaryngol 101-6(1):101-6.
Stammberger H, Posawetz W. (1990) Functional endoscopic
sinus surgery. Concept, indications and results of the Messerk-
linger technique. EUFOS : af liated with the German Society for
Oto-Rhino-Laryngology - Head and Neck Surgery 247(2):63-76.
White DV, Sincoff EH, Abdulrauf SI. (2005) Anterior ethmoidal
artery: microsurgical anatomy and technical considerations.
Neurosurgery 56(2 Suppl):406-1.