
Medical
Communication
Biosci. Biotech. Res. Comm. 10(3): 542-550 (2017)
Perceived challenges by the Iranian baccalaureate
surgical technology students in their clinical education:
A qualitative study
H. Karimi Moonaghi
1
, R. Zardosht
2
*, M. Etezad Razavi
3
and S. Ahmady
4
1
Ph.D Nursing Education, Associate Professor, Evidence-Based Caring Research Center, Department of
Medical-Surgical Nursing, School of Nursing and Midwifery, Department of Medical Education, School of
Medicine, Mashhad University of Medical Sciences, Mashhad, Iran
2
Student Research Committee, School of Nursing and Midwifery, Mashhad University of Medical sciences,
Mashhad, Iran
3
Eye Research Center, Khatam-al-Anbia Hospital, Faculty of Medicine, Mashhad University of Medical
Sciences, Mashhad, Iran
4
Faculty of Medical Education, Shahid Beheshti University of Medical Sciences, Tehran, Iran
ABSTRACT
The operating room eld in Iran is a branch of medical sciences during this period, students became become familiar
with the new principles of the operation room and modern surgical techniques in specialized and super specialized
surgeries and they train the care and assistance to the patient’s administration before, during and after operation. The
purpose of this qualitative study is to investigate how the students are taught, the effective factors and possible chal-
lenges related to educational issues in the operating room. This is a qualitative content analysis which was performed
in 2014-2015. The participants consisted of 35 bene ciaries in the operating room eld, namely, students of different
academic terms, matrons, educators (instructors), surgeons and operating room personnel in different academic cent-
ers in Khorasan Razavi province who were rich in information and had a tendency to comment on their experience.
In this study, sampling was rst carried out in a targeted way and then was continued with theoretical sampling
and sampling was continued until data saturation. All interviews were recorded and then handwritten and analyzed
using continuous comparative method and qualitative content analysis. The profound and deep descriptions of the
participants led to the emergence of 13 subcategories and 3 main categories of the “unconventional educational
atmosphere”, “the challenge of student admission to the surgical team,” the “operating room culture” and, nally,
542
ARTICLE INFORMATION:
*Corresponding Author:
Received 21
st
June, 2017
Accepted after revision 27
th
Sep, 2017
BBRC Print ISSN: 0974-6455
Online ISSN: 2321-4007 CODEN: USA BBRCBA
Thomson Reuters ISI ESC and Crossref Indexed Journal
NAAS Journal Score 2017: 4.31 Cosmos IF: 4.006
© A Society of Science and Nature Publication, 2017. All rights
reserved.
Online Contents Available at: http//www.bbrc.in/
DOI: 10.21786/bbrc/10.3/31
H. Karimi Moonaghi et al.
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS PERCEIVED CHALLENGES BY THE IRANIAN BACCALAUREATE SURGICAL TECHNOLOGY STUDENTS 543
one main theme of the “dynamic nature of the operating room”.The special educational environment in the operat-
ing room environment, lack of acceptance of students in the surgical team as a training member and hierarchical
culture of the operating room, has created problems for the training of these students. In fact, the clinical training of
operating room students is based on teamwork and the members of the surgical team are, in some cases, instructors
in the shade. Given the dynamic nature of the operating room, collaboration and participation between educational
and clinical institutions can help improve the learning environment, acceptance students in the surgical team as a
training member, and creating a dynamic, collaborative and exible culture.
KEY WORDS: PERCEIVED CHALLENGES IRANIAN BACCALAUREATE SURGICAL TECHNOLOGY STUDENTS
INTRODUCTION
Bachelor of Science in surgical technology in Iran is a
branch of medical science during which the students
become familiar with new principles of surgical tech-
nologies in specialty and subspecialty surgeries and they
learn how to care and help the patients before, during
and after surgery (Operating Room and Anesthesia,2017).
Training programs of operating rooms are offered in
two ways worldwide: in the rst case, nursing gradu-
ates (after achieving a bachelor’s degree) are trained in
a period of 1-2 years to enter the operating room. In the
second case, surgical technicians, after general training
of the operating room, are prepared to act as a mobile
and scrubs and then, if desired, they are prepared as the
rst help of the surgeons in a period of 1/5 to 2/5 years.
Standards of patient care in the community of operat-
ing room nurses in America also show that students of
operating room technician can pursue their education
in specialized courses in higher education. The people
of each period have their own duties and the role of
these specialized people is different from the operating
room technician. Operating room is a complex system
that coordinates the individual, technology, and patients
in a physical environment to achieve favorable out-
comes in patients (Islamic Republic of Iran Ministry of
Health and Treatment and Medical Education Supreme
Council for Planning of Medical Sciences, 2007). Oper-
ating room is considered as high-risk environment for
patients, because in spite of the small number of cases,
some potential problems of patients after the surgery are
due to the mistakes of the operating room personnel that
can lead to the death of the patients (Deyoung 2009).
In Iran, students of surgical technology are admitted
directly based on the exam and with no relation to nurs-
ing. This eld, in different colleges between the years
1987 to 2001 and it was launched at the undergraduate
across the country, was launched in the associate degree
level in 2009 (Operating Room and Anesthesia, 2017).
Due to the fact that now in Iran there is no training
courses in doctoral degree (Ph.D.) for surgical technol-
ogy and its MA was launched only two years ago, MS
nurses in internal injuries (with work experience in the
operating room or an associate degree in surgical tech-
nology) take the responsibility of the practical and theo-
retical training of this group of students in educational
centers. Given that the eld is new and considering the
volume increasing of training centers for students, it is
not considered the required infrastructures such as spe-
cialist human resources in clinical training and educa-
tional facilities in proportion to the number of students.
There is not enough number of teachers in the eld,
so in many centers teaching this group, traditionally,
is given to the supervisors and operating room person-
nel. Subsequently, due to lack of necessary knowledge of
educational affairs, students have faced with problems
in their training (Bahrami et al 2014).
The purpose of the training is the optimal and effec-
tive care of patients before, during and after the sur-
gery especially in the specialized surgeries, control and
prevention of nosocomial infections as well as creating
the perfect mental conditions for patients and proper
maintenance of devices and medical equipment (Islamic
Republic of Iran Ministry of Health and Treatment
and Medical Education Supreme Council for Planning
of Medical Sciences 2007). However, some items such
as technical approach to the eld, high expectation of
the graduates in this eld to help surgeons, and sepa-
ration from nursing have caused the graduates to not
have enough knowledge of nursing care of patients
before and after surgery as well as communication with
patients. So, they have just learned the technical skills
during the surgery (Bailey 2010).
Foreign countries’ researches have reported about
training in the operating room which is connected with
the collaboration (Silen-Lipponen et al., 2004) stress,
communication failures (Laur et al., 2012), the effect of
stress on other members and students (Kenton 2006) and
to the development of the group of Skoczyl et al. (2005).
The difference in the education of graduates of the sur-
gical technology in Iran and other countries has caused
the results of the studies in the eld to be inapplicable
in the country. Unfortunately, there is not extensive and
ef cient research in the surgical technology in the coun-
try. Conducted researches are quantitative and investi-
gate certain aspects of education in surgical study. So,
H. Karimi Moonaghi et al.
544 PERCEIVED CHALLENGES BY THE IRANIAN BACCALAUREATE SURGICAL TECHNOLOGY STUDENTS BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
they are not able to analyze all aspects of education in
the surgical technology (Bahrami et al., 2014; Khazaei
et al., 2014, Tazakori et al., 2016).
However, qualitative approaches have holistic
approach to the phenomenon and gain precious informa-
tion about the training in the clinical environment. The
aim of this qualitative content analysis is the evaluation
of teaching the students, their required skills, effective
factors and potential challenges associated with educa-
tional issues in the operating room. Planning to elimi-
nate the defects of the eld improves the knowledge and
skills of students in this eld, provides better care for
patients, and ultimately improves the health system.
MATERIAL AND METHODS
The study is a qualitative content analysis study (part
of a larger study). It was conducted in 2014-2016 to
reveal the problems and challenges of education in the
eld of surgical technology in Iran. The environment
includes all the operating rooms of educational hospi-
tals of Khorasan Razavi (Mashhad, Nishabur, Torbat Hei-
darieh and Gonabad). The interview was done in places
that are accessible to participants or places they desired.
The participants were 35 of bene ciaries of education
in surgical technology such as the students of differ-
ent academic semesters, head nurses, teachers, surgeons
and operating room personnel at various universities in
Khorasan Razavi province. They have precious informa-
tion and they were willing to recount their experiences.
Sampling was done by using purposive sampling and
continued by theoretical sampling. Some of the charac-
teristics of the participants are as follows: willingness
to participate in research and express their experiences,
students who had spent at least one training courses,
educators who had at least a year of training in the oper-
ating room, and operating room personnel who had at
least one year of work experience in the room.
Data were collected by using semi-structured indi-
vidual interviews. The interview was started by general
questions regarding the interview directory and was
guided by the responses of participants. After explaining
the objectives of the plan to participants and obtaining
informed consent, data collection was began. The main
question were as follows: what makes you to call a day
of the training as good and useful? Or feel the training
is not of enough interest today? Mention a good expe-
rience and a bad experience from your training in the
operating room? What are the facilitating and impeding
factors in your clinical training?
A total of 37 interviews was carried out (35 initial
interview and two follow-up interviews). The study
continued from Tir 93 to Azar 95 (Iranian year). The
researchers tried to consider the maximum variation in
the sampling; (14 students, 6 Operation room person-
nel with associated degree or BS in surgical technology
or BS in nursing, 4 operating room heads, 6 training
teacher, one Dean of the Faculty, 3 surgical assistants
and one surgical staff). Educational centers of Khorasan
Razavi included Mashhad, Torbat Heydarieh, Gonabad
and Nishabur. Data were analyzed according to conven-
tional content analysis.
The data analysis was based on Graneheim and Lun-
dman in seven steps (Graneheim and Lundman 2004).
In the rst step, all interviews were recorded and tran-
scribed. Then, the decision made about the analysis unit
and before starting the coding process, text of interviews
was read several times as the unit of analysis. Mean-
ing Units were also read and reviewed several times and
unrelated statements were deleted. First, some units were
de ned and relevant codes of each Meaning unit were
written and then the codes were classi ed inductively
and based on common sense and meaning.
The process of data reduction was continued in all
units of analysis and primary and secondary classes. In
other words, subclasses with similar events are grouped
together as classes and then primary classes formed
and this trend continued up to the theme. It should be
noted that during the analysis the necessary changes
were done in the name of the classes which must show
the content of the class. The analysis was continually
conducted by adding up each interview and the classes
were modi ed. To simplify the process of data analysis,
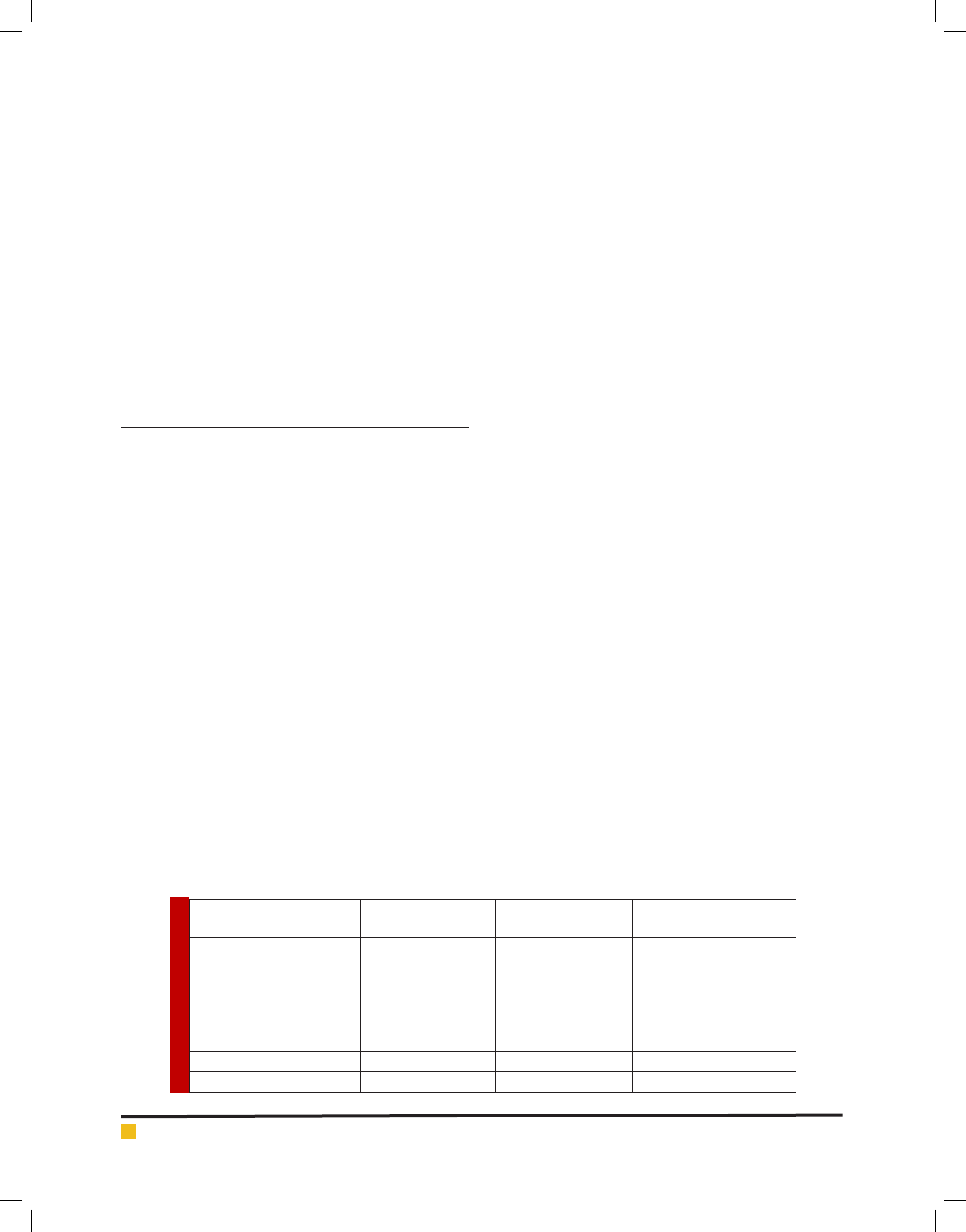
ParticipantsNumberAgeGender
Work experience in the
operation room
Student1422-2011 females/3 malesSemester 4 to 8
Training teacher648-355 females/1 male3-20 years
Operating room personnel655-325 females/1 male8-25 years
Dean of the Faculty152Male-
Assistant348-32
Chanbge this year to
English Calender Male
4-5 years
Staff153Male17 years
Operating room head455-32Male15- 29 years
H. Karimi Moonaghi et al.
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS PERCEIVED CHALLENGES BY THE IRANIAN BACCALAUREATE SURGICAL TECHNOLOGY STUDENTS 545
coding, cataloging and classi cation, comparing various
data frequently and retrieving quotes, we used software
MAXQDA 10 (Mayring 2000).
To increase the reliability and validity of the results,
we used the methods used by Cuba and Lincoln that
were quoted by Polit and Hungler. The two research-
ers consider the four criteria of con rm ability, cred-
ibility, dependability and transferability as necessary for
the consistency and strength of qualitative data (Burn
and Grove 2007). Therefore, researchers have helped to
validate data with continuous involvement with data,
data veri cation by the participants, allocation of suf-
cient time to the study and open communication and
empathy with the participants. In order to determine the
dependability, two separate research teams coded the
Interviews that there was a high degree of agreement
(85%) between the comments. Also, great care was done
in the collection, implementation and recording of data
and allocating of enough time to collect the data. As
for the transferability, manuscripts, interviews and units
of analysis with extracted initial codes were provided
to participants and the necessary corrections made and
the proposed points were considered. In addition, three
expert in the eld of qualitative research monitored the
study. Using a combination of methods (interviews and
eld notes) as well as sampling with maximum diversity
(interviews with students of different academic semesters
from different training centers, faculty-member educa-
tors, non-faculty member educators, and surgeons with
different expertise) have increased the con rm ability
and transferability of the data. In addition, describing
the studied background, providing necessary explana-
tions about the participants and using of their direct
quotations was also done in this regard.
Ethical considerations in this study include: obtain-
ing ethical permits from Committee for Medical Research
Ethics of Medical Sciences of Mashhad (ethical code
940548), explaining the purpose of the study and the use
of tape recorder, explaining the way of collecting data
for the participants and satisfying them to cooperate,
obtaining consent in writing for conscious participation
and paying attention to the basics including the research
explanation, identifying the purpose of the study, stat-
ing the criteria for sample selection, the bene ts of
participation in the research, ensuring the anonymity,
answering questions, the right to refuse to continue the
research, providing adequate information and assuring
the participants to put the interviews in a safe place.
RESULTS AND DISCUSSION
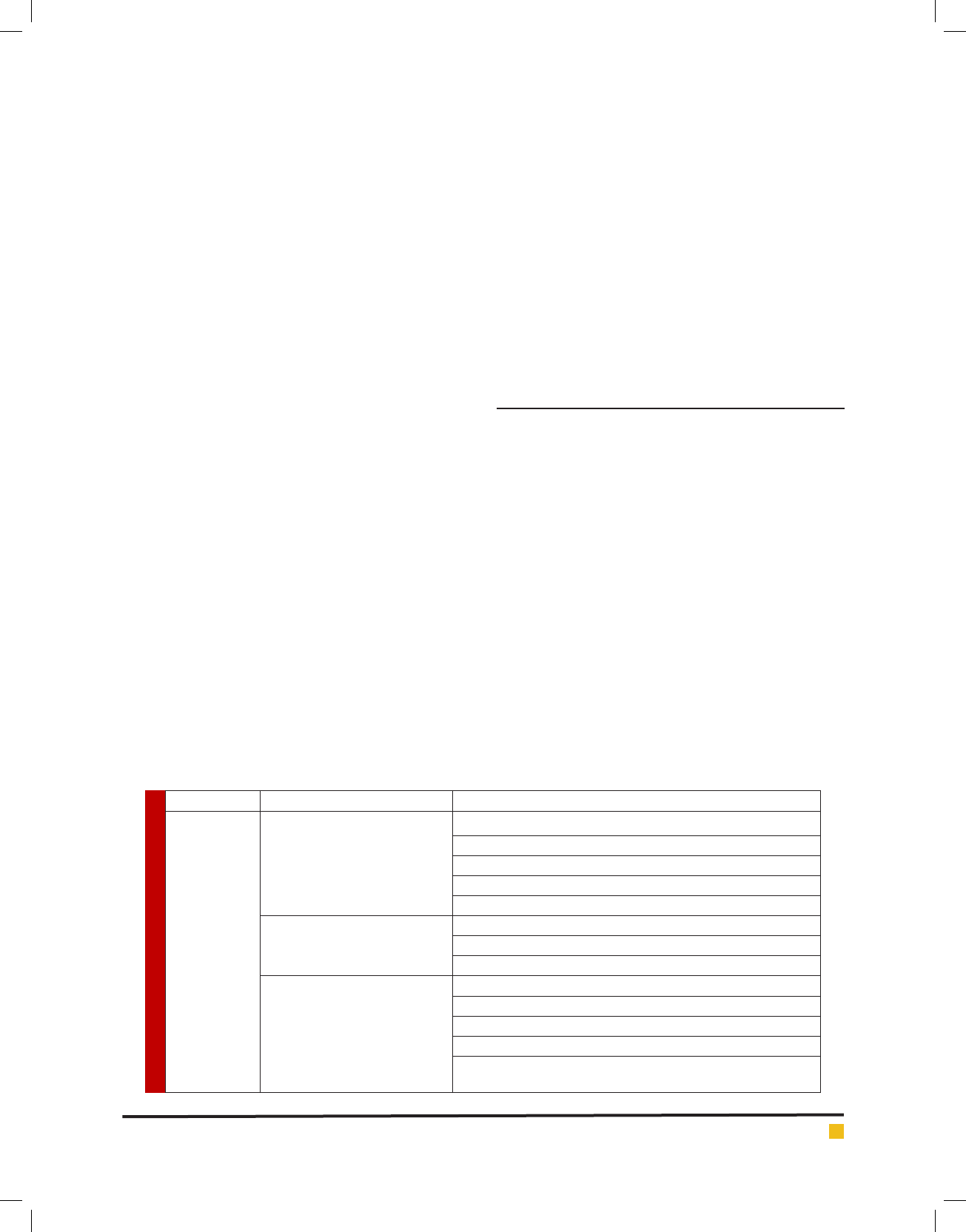
Data analysis of participants’ statements and notes in
the eld lead to the emergence of 12 subcategories and
3 main categories and eventually one main theme.
Main category: unconventional educational atmosphere
This category includes the following subcategories: lack
of facilities and trainers, lack of balance between train-
ings and goals, red lines, safety and sterility principals,
the confrontation of the caring and technical roles of stu-
dents and the simultaneous presence of other students.
Lack of facilities and teachers: learning environment
has been considered as a key environment for education
and training of students and for helping to link theory
with the practice in the clinical setting. The data in this
study showed that the participants are not satis ed with
their learning environment. A training teacher with sev-
eral years of experience in the operating room, says:
”In the classroom sometimes it is required to explain
or draw a part of something and there is no whiteboard
and facilities there. There is no place for equipment and
SubcategoryMain categoryMain theme
Lack of facilities and teachers
Unconventional educational
environment
The dynamic nature of operating room
Lack of balance between training and goals
Red lines, safety and sterility principals
The confrontation of caring and technical roles of students
The simultaneous presence of other students
Annoying students and reduction of team speed
Challenge to admit students to the
surgical team
Lack of required knowledge and skills
The absence of the trainer and humiliation of the students
Teamwork
Operating room culture
Gender discrimination
Hierarchical structure (physicians governorship)
Paradox of Professional interactions and inappropriate interactions
Duality of behaviors and the absence of legalism
H. Karimi Moonaghi et al.
546 PERCEIVED CHALLENGES BY THE IRANIAN BACCALAUREATE SURGICAL TECHNOLOGY STUDENTS BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
relaxation of students and it seems as though they do
not have facilities for us”. The conversion of associate
degree to bachelor and the increase of the number of
students regardless of the required infrastructure have
created problems. The operating room head who has
been in charge of training courses says: “The teacher
cannot afford to train the students due to the increas-
ing number of students as well as the presence of stu-
dents from semester 4, 6, 8,”. A student says:” teachers
cannot teach us everything and do not have time to do
so”.In educational centers of cities other than Tehran,
students actually cannot see thoracic and cardiac sur-
geries, advanced neurological and eye surgery. “Due to
the low number of operating rooms and lack of variety
in surgeries, the trainings in the cities are the same and
students see the same surgeries in the semester 8 that
had seen in semester 2”
Lack of trainers: it is hard to understand the routine
and special procedures of hospitals for educators who
temporarily go to the hospital with students. Absence
of the trainer or the use of non-professional teachers or
staff have affected the clinical training of surgical tech-
nology students. A student says: “When we do not have
any trainers, the only thing is the attendance. Then, they
told us to go to the rooms and it is not important to
learn or not to learn”. In multiple studies, students’ con-
fusion and uncertainty in the absence of the trainer has
been reported as factors causing problems.
“Of course, depending on the hospital, when we do
not have trainer and the nurse is responsible for check-
ing, there is no problem if we are late. I do not remember
any washing. Because we do not have xed trainer, they
do not have us to do morning washing.
Mismatch between educational objectives and
training objectives: Data analysis showed that the stu-
dents complain about the aimless trainings and they
consider the lack of transparency in goals and evaluat-
ing the training as a major problem. A senior student
says: the lesson plan is originally for apprenticeship and
they should it to students to understand what they do.
In fact, I mean that we should be given a sheet based on
which they evaluate us. I have not seen anything and
most professors evaluate us based on scrub “Students
considered as useless some training courses including
recovery or management trainings. A student says: “We
have weaknesses in le writing and recording of HIS
and I personally cannot do this. At least they should
include this in training courses. “A student told about
the lack of training in Laparoscopy: “I went to the room
for laparoscopic surgery and it was cholecystectomy. I
did not know anything about laparoscopy even the the-
ory. The personnel came and taught me quickly.
Red lines, safety and sterility principals: the operat-
ing room is a complex system in which an individual
coordinates the technology and patients in a physical
environment to achieve optimal outcomes in patients.
Data analysis showed that the majority of operating
room personnel are sensitive to safety and sterility prin-
cipals of patients. A personnel says:
“If we told them to cover your hair, they would think
it is because of Hijab but it is not and if the hair go to
the sterile eld, it can cause infection and problems for
patients. Although we notify them, they hate. The health
is important here and you can be as you will out of
here. And you have to comply with the rules and stand-
ards here.” On the other hand, surgeons also have their
own reasons for patient safety: “The patient has trusted
the surgeon about his life and the decision maker is the
surgery team. Survival is not interchangeable with any-
thing. It is not acceptable to put the life of the patient
in danger.”
Confrontation of caring roles and technical roles of
students: in the operating room environment, compared
to the other sectors, a speci c aspect of care is mostly
emphasized that is technical. One of the participants
says:”If we look at it as a scienti c discipline, we must
go beyond the skills and consider it as theory-based
thing. The problem here is that it seems most of the
duties designated for the graduates of this eld is practi-
cal, but this eld is subdivision of the Nursing Science.
The thing that now is happening is the technical look at
the graduates of the eld. So, they are expected to know
the equipment and to help the surgeons in the surgery.
Simultaneous presence of students from other
disciplines: the difference in the type of training and
simultaneous activity of surgical technology and other
students and operating team make the operating room
training more different and dif cult than other parts
of the hospital. Faculty member trainer with 14 years
of experience in training in the operating room says:
“Simultaneous presence of students with different lev-
els of training from freshmen to residents and even the
professor himself in a place leads to different clinical
experience in the place and the students cannot keep up
with the situation and it is dif cult to them.
Second category: the challenge of admitting the
students in the surgical team
This category includes annoying students and the reduc-
tion of the team speed, lack of the required knowledge
and skills of students, the absence of the trainer and the
humiliation of students. Data analysis showed that the
surgeon believes in the priority of patient safety and the
life rather than the training and he/she seeks a surgery
with minimal side effects for the patient.
Annoying students and the reduction of the team
speed: an operating room personnel in this regard
says:”The students are beginners and annoying. The

H. Karimi Moonaghi et al.
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS PERCEIVED CHALLENGES BY THE IRANIAN BACCALAUREATE SURGICAL TECHNOLOGY STUDENTS 547
personnel’s works are rapid and easy, but it is not the
same for students. They stand there without doing any-
thing even when the assistant wants to move to the
other place. Another trainer says:”Students in the oper-
ating room are uninvited guests and physicians and sur-
geons are sensitive to the students. Unfortunately, I’m
concerned about the students and I permanently turn
around in their room and it leads to sore feet because
there is no place to sit.
Lack of required knowledge and skills of students:
Interview with operating room assistants showed that
admitting the students in the surgery team causes some
problems.”We had a student that knew no equipment. In
the middle of the surgery we had to change him because
it was a two hour surgery and we were just cutting the
area without doing anything. He had lowered our speed
and we had to change him.
Absence of the trainer and the humiliation of students:
a student says:
“When we did not have the trainer, the personnel took
the responsibility and the only important thing was the
attendance. Then we were told to go to the rooms and it
was up to us to learn or not to learn. “I thought that I am
a useless creature that gets humiliated and the students
were blamed for any mistakes.”
Or another student talks about the impact of every
single person on the admission of the student in the
team: “The surgery began and we wanted to go to the
room, but the surgeon did not allow. As I said it depends
on the surgeon and other factors and all of these are
effective in our training.
Third category: The operating room culture
This category includes teamwork, gender discrimination,
hierarchical structure (surgeon as the governor), paradox
of professional interactions and inappropriate interac-
tions, behavior duality and lack of rule of law.
Teamwork: Since the operating room environment is
of interactive and dynamic nature, to make the surgery
team more cooperative and to eliminate the confusion of
the students in the room, the clinical education program
of the students should be transparent for the operating
room personnel. Some operating room personnel do not
consider the participation in the training as a part of
their duties and even disappoint the students and the
trainers with inappropriate behavior and create an unfa-
vorable atmosphere. However, some staff play the role of
the trainer for the students. “Most guys say that the edu-
cator plays an important role in the training. However,
I say some personnel are the trainers of the students
and they explain for you the techniques step by step in
the operating room. Faculty member instructor with 14
years of work experience in training says: “See! It is a
teamwork and each and every member of the operating
room can have clinical effect. Perhaps the least role is
for the head nurse and the personnel in the room have
the greatest role in training students.
Gender discrimination: One of the known causes of
stress in operating room environment for students is the
others’ behavior.”A senior student says: unfortunately,
some personnel or male surgeons work with female stu-
dents. I like justice not discrimination. It is not fair to dis-
miss the female students earlier than males. If the female
students cry, the personnel and the surgeon will change.
Hierarchical structure (doctor as the governor)
researchers believe: a good clinical setting has non-hier-
archical structure in which the works are done in teams
or groups and there is good communication. A trainer
says:”Look! When you have a pretentious assistant who
does not know his work well and says I’m very good and
am in a hurry, he does not let the students use the equip-
ment correctly. He watches the student carefully. How-
ever, a patient assistant says take your time we are not in
hurry and even tells anesthesiologist that we need more
time. Unfortunately, we don’t have many of this surgeons
and you have to have a chance to work with them.
Paradox of professional interactions and inappro-
priate interactions: To make a team work so ef cient,
team members should be familiar with their capabilities.
This leads to appropriate interactions between them and
coordinates them. The trainer says:”Even students work
more with good communicators. He might not be well in
the knowledge, but he is good at communication. When
he graduates, he is better than a good student with weak
relationship and this is important. One of the operating
room personnel in connection with the close interaction
in the environment of operating rooms says: “some stu-
dents abuse this open communication and some of them
do not have the capacity of such communication.
Studies have shown that in a good clinical setting
the interactions are not top-down and the work is done
interactively. Data analysis and statements from stu-
dents and educators in this study shows that surgeons
have a top-down look to surgery team especially sur-
gical technology students. This behavior is not in the
framework of the operating room rules.”Unfortunately,
in Iran the higher the education, the higher the immo-
rality and higher education leads to higher immorality.
Behavior duality and lack of rule of law: in the status
quo operating room personnel do not consider the coop-
eration in training as their duty. And they do not have
necessary cooperation with the trainer for providing
the required facilities to students and transferring their
experiences in the absence of the trainer.”The student is
of no position and is blamed for everything wrong even
it is the fault of the personnel. Another trainer about
the ignorance of some surgeons says:”According to the

H. Karimi Moonaghi et al.
548 PERCEIVED CHALLENGES BY THE IRANIAN BACCALAUREATE SURGICAL TECHNOLOGY STUDENTS BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
rules of the school we took a male student to the women
operating room. The gynecologist of the room began
to quarrel and said to force the student out. Another
trainer in connection with the operation room atmos-
phere says:”There is no law here. If there is a law, they
can be persecuted. However, doctors are the governors
and we cannot blame them.
Results of the study show that the challenges of clini-
cal education in the operating room in Iran, due to the
complex and dynamic nature of operating room, are
as follows: special educational environment, problems
of admission of the students as a member of the surgi-
cal team in operating room, and different culture of the
operating room. By comparing these, we can say that the
certain circumstances, difference of the operating room,
a shortage of faculty member in the department, and less
control of the trainer in the clinical environment of the
operating room have affected the training opportunities
of students in this eld.
Operating room (OR) clinical practice involves special
contextual elements related to the preoperative nursing
process, practical OR nursing skills and teamwork in dif-
ferent patient care situations. However, the OR is one of
most inaccessible places in a hospital where the use of
space is highly regulated. Areas of space are divided into
unrestricted, semi restricted and restricted sections, and
the physical activities performed within each of these
designated areas are differentiated (Riley and Manias
2002). Working conditions for graduates of surgical
technology is different than those of other nurses. He is
forced to comply with a variety of procedures and high
workload quickly and carefully. Due to the quick entry
and exit of patients, his work is not expectable and in
many cases he is faced with acute and emergency situ-
ations and concurrent interactions with members of the
surgical team. It can harden the clinical education of the
students (Farneya et al 2013).
Because of the special atmosphere of the operating
room compared to other sectors, it seems that there is
more emphasis on the students of the eld in techni-
cal skills and speci c approaches of the care. In Khaz-
ayi’s study (2015) about the clinical education of sur-
gical technology, the students gave the highest points
to the learning opportunities and the lowest points to
the performance of educators and educational facilities
(Khazaei et al 2014). The high point to learning oppor-
tunities is due to the favorable reception in parts that
were faced with shortage of human resources and the
students played the role of assistance in these sectors.
In the study of Ghorbanian et al.(2014), the most impor-
tant weaknesses of clinical education of operating room
are as follows lack of using teaching aids, inadequate
number of patients for learning, lack of knowledge of
students of clinical evaluation system, lack of adequate
oversight on the clinical education and lack of decision-
making power of the student in planning the care of
patients (Ghorbanian et al., 2014).
These are consistent with the contents obtained in
our research. In the study of Dehqani et al (2007), the
absence of proper scienti c grounds, lack of interest in
the students, confusion and uncertainty of the students
in the absence of the trainer were mentioned as factors
causing problem for training process (Dehghani et al.,
2005). Omidvar et al in Babol University of Medical Sci-
ences also considered the problems of clinical education
related to health centers’ personnel and their knowledge
(Omidvar et al. 2005).
In a similar study by Hadizadeh et al., it was found that
the understanding and cooperation of the health centers
staff is important in the educational process (Hadizadeh
et al., 2005). Providing diverse learning opportunities,
receiving proper feedback from trainers as well as clinical
environment are the important and effective factors of
clinical training in the other country’s studies (Andrews
et al., 2006 and O’Driscoll et al., 2010). The results of this
study showed that due to the special circumstances of the
operating room, the admission of the students as a surgi-
cal team member has faced with dif culties.
Qualitative research of Lingard et al (2002) showed
that the communication models in the operating room are
complex and socially-motivated. The predominant themes
include, time, security, sterilization, resources, roles and
conditions. Often, every procedure had 1 to 4 stressful
incidents and the stress transferred to other team mem-
bers or the environment. In response to the tensions, the
trainee of the operation was separated from the surgical
team or began to mock. Both of these reactions are nega-
tive indicators for the team communications. The results
are consistent with the study of Lingard et al (2002).
Tanner and Timmons (2000) emphasized that behav-
ior in the OR is different from that in other hospital areas,
and that the OR could be described as a ‘backstage’ area.
In a backstage area interaction includes joking, talking
about aspects of private life and behaving in a famil-
iar manner. It also includes gossiping and disrespectful
talking, even about patients during narcosis, which was
also mentioned in this study. Frontstage behavior is the
absence or opposite of this and occurs in the or when
the patients are conscious before anesthesia or in the
recovery unit (Tanner and Timmons 2000).Perhaps this
antagonism between backstage and frontstage behaviors
explains the students’ excitement and frustration in the
OR. Usually, before their OR placement period, students
have spent time in frontstage areas, have dealt with staff
more formally and have had closer caring relationships
with patients. In addition, some nursing students have
previous experience of patient care before enrolling in
H. Karimi Moonaghi et al.
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS PERCEIVED CHALLENGES BY THE IRANIAN BACCALAUREATE SURGICAL TECHNOLOGY STUDENTS 549
the programme (Manninen 1998 (which probably makes
their views about nursing more frontstage-oriented
In this study, participants have considered the admis-
sion to the surgical team as a gateway to opportunities
for learning clinical skills and using experience of team
members. However, the admission has its own problems.
In the study of Tazkori et al (2015), issues related to
clinical education in the operating room are as follows,
the lack of proper planning for training period, lack of
trust in teachers, lack of exibility in the face of criti-
cism and non-compliance with professional ethics and
lack of taking time for clinical and educational consul-
tation, lack of learning opportunities in hospitals, lack
of familiarity with the described tasks of the students. In
Liponen’s study (2004) which was conducted as descrip-
tive phenomenology associated with the clinical set-
ting of operation room, three types of teamwork were
reported from the point of view of students:
Three types of teamwork emerged based on the stu-
dents’ perceptions: functional manifestation of OR
teamwork, gaining OR team membership and technical
orientation of OR teamwork. The ndings are discussed
in relation to OR practice, education and research on
ways to improve teamwork while maintaining a satis-
factory OR learning context and stimulating interest in
perioperative nursing). (Silen-Lipponen, et al 2004) The
implications of this study is consistent with the nd-
ings of our study. In another study that was conducted
in Bushehr University of Medical Sciences, the results
showed that the students consider the lack of learning
opportunities as one of the educational barriers (Abidi
and Motamed 2011).
Although working in the operating room is a team-
work and it needs participatory culture, the results of
our study showed the hierarchical culture in the clini-
cal setting of the operating room and the surgeon is
the commander and decision maker and sometimes he/
she loses the students’ learning opportunities. Sadeghi
et al (2011) believe that a weak and in exible culture
in the organizational environments causes employees
not to tend to the innovation, change and creating new
ideas and they fear from knowledge sharing. However, a
dynamic, collaborative, and exible culture reacts well
to changes and leads to the progress (Sadeghi,,2011).
As studies show, participation and support from
staff increase the learning opportunities for students
(Heshmati et al2012). The results of another qualitative
research (2004) showed that about 30 percent of the
team transactions are faced with communication failure
and cause problems. One-third of the cases associated
with increased cognitive load (information processing in
short-term and activated memory), interrupting the pro-
cedure, increased tensions and jeopardizing the safety of
the patients (Zeighami et al 2004). However, Heshmatis
study showed that nursing instructors use strategies like
skills, realism, responsibility, determination, humility
and using the experiences of nurses to attract the col-
laboration of clinical staff in providing clinical trainings
(Heshmati 2012). However, other studies in our country
showed that the nursing teachers have problems in play-
ing their educational role (Heshmati et al 2010).
As stated by participants in this study, despite the
difference and stressfulness of the clinical setting and
its effect on clinical education of the students, participa-
tion and cooperation of every member of the surgical
team can enhance the quality of the clinical skills of
the students and this cannot be achieved unless in envi-
ronments with supportive and participatory culture.This
qualitative study was part of a larger study considering
restriction of the studies with qualitative methodology;
Such as: the subjective nature, eld-based and their low
level of generalizability. Despite these limitations, the
results of this study provide deep understanding about
the nature of clinical environment of the operating room
and the problems related to clinical education of stu-
dents of surgical technology.
CONCLUSION
According to the ndings of this study, the unconven-
tional educational environment in operating room, non-
admission of the student in the surgical team as an edu-
cational member, and hierarchical culture of operating
room have caused problems for these students. Since the
work in the operating room is collaborative and con-
current, control of this clinical learning environment is
dif cult. In fact, clinical education of the surgical tech-
nology students is team-based and all members of the
surgical team are, somehow, trainers in the shadow. Due
to the dynamic nature of the operating room, coopera-
tion of educational and clinical institutions can improve
educational environment, admission of the student as an
educational member in the surgical team, and creating a
dynamic, collaborative and exible culture.
ACKNOWLEDGEMENT
This study is part of a larger study and extracted from
a doctoral dissertation. Writers appreciate all the great
professors who provide the research facilities as well as
Deputy Minister for Research and Technology of Mash-
had University of Medical Sciences for nancial support.
REFERENCES
Abidi N, Motamed N. (2011). School of Allied Health and Nurs-
ing students’ and teachers on the Bushehr University of Medi-
cal Sciences and Clinical Education. Strides Dev Med Educ;
8(1): 88-93. (Persian)

H. Karimi Moonaghi et al.
550 PERCEIVED CHALLENGES BY THE IRANIAN BACCALAUREATE SURGICAL TECHNOLOGY STUDENTS BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
Andrews GJ, Brodie DA, Andrews JP, Hillan E, Thomas BG,
Wong J, Rixon L. (2006). Professional roles and communica-
tions in clinical placements: a qualitative study of nursing stu-
dents’ perceptions and some models for practice. International
Journal Nurs Study; 43 (7):861-874.
Bahrami, T. Sadat, L. E. Mahmoudi. Golgini. E. (2014). Evalua-
tion of the clinical training of students’ views in the operating
room and anesthesia Alborz. University of medical scienes and
health .Journal of Alborz University of Medical Sciences. Vol-
ume 1, Number 3, summer 143-150, 139. [In Persian]
Bailey L. (2010). Strategies for decreasing patient anxiety in
the perioperative setting. AORN J; 92(4): 445-57
Burns, N; Grove, SK.(2007). Understanding nursing research,
building an evidence-based practice. 4th edition. St. Louis:
Saunders Elsevier.
Dehghani H, Dehghani K, Fallahzadeh H. (2005). The edu-
cational problems of clinical eld training based on nursing
teachers and last year nursing student’s viewpoints. Iranian
Journal of Medical Education; 5(1):24-33. [Persian]
Deyoung S. (2009). Teaching strategies for nurse educators. 2th
Ed. New Jersey: Prentice Hall. P.222-223.
Silen-Lipponen, M; Tossavainen, K; Turunen, H; Smith, A.
(2004). Learning about teamwork in operating room clinical
placement. British Journal of Nursing; 13.5 (24); 244-253.
Farneya, F; Abbaszadeh. A; Borhanif, F. (2013). inhibiting fac-
tors associated patient care in the operating room: a qualita-
tive content analysis. Journal of Health Sciences Research; 2
(1): 90-7.
Ghorbanian N, Abdollahzadeh Mahlani F, Kazemi Haki B.
(2014). Effective Factors on Clinical Education Quality; Anes-
thesiology and Operating Room Students View. Bimonthly
Educe Strategy Med Sic; 6 (4):235-239. [In Persian]
Graneheim UH, Lundman B. (2004). Qualitative content analy-
sis in nursing research: concepts, procedures and measures to
achieve trustworthiness. Nurse Educ Today; 24(2): 105-12.
Hadizadeh F, Firoozi M, Shamaeyanrazavi N. (2005). Gonabad’s
nursing students’ views about clinical Education assessment.
Iranian Journal of Medical Education; 5(1):70-8. [Persian}
Heshmati, Nabavi1, F. Vanaki, Z., Mohammadi, E. (2012). A
Critical Review on Communication Paradigms Beteween Aca-
demic and Clinical Service Institutions in Nursing. Iranian
Journal of Medical Education: 11(6); 554-568
Heshmati-Nabavi F, Vanaki Z. (2010). Professional approach:
the key feature of effective clinical educator in Iran.
Islamic Republic of Iran Ministry of Health and Treatment and
Medical Education Supreme Council for Planning of Medi-
cal Sciences, Educational programs of Baccalaureate Degree
operating room, Pro le, program, curriculum and evaluation
method. Adopted by 35 Th session of the Higher Council for
Planning of Medical Sciences: 20 /12/2007.
Kenton, K. (2006). How to Teach and Evaluate Learners in the
Operating Room. Obstetric Gynecology Cling N Am; 33; 325–
332.
Khazaei, J, Zarouj, H.Abbasi A. (2014). Quali cation of Clini-
cal Education of operation room in Bachelor degree from the
perspective of students and educators in this eld at the Uni-
versity of Medical Sciences, in Semnan Journal of Education
and Ethics in Nursing; Volume 3, Number 3, 39-46 [In Persian]
Khazaei, J, Zarouj, H.Abbasi A. (2014). Quali cation of Clini-
cal Education of operation room in Bachelor degree from the
perspective of students and educators in this eld at the Uni-
versity of Medical Sciences, in Semnan Journal of Education
and Ethics in Nursing; Volume 3, Number 3, 39-46 [In Persian]
Laura, C; Skoczylas, E B; Littleton, Steven, L; Kanter and Gary
Sutkin. (2012). Teaching Techniques in the Operating Room:
The Importance of Perceptual Motor Teaching. Academic Med-
icine; 87(3).
Lingard, L; Reznick, R; Espin, S; More. (2002). Team Communi-
cations in the Operating Room: Talk Patterns, Sites of Tension,
and Implications for Novices. Academic Medicine; 77(3):232-
237.
Manninen E (1998) Changes in nursing students’ perceptions
of nursing as they progress through their education. J Adv
Nurs 27: 390-8
Mayring p. (2000). Qualitative Content Analysis. Forum: Qual-
itative Social research; 1(2): 25-30
Moussaoui, S. (2005). Professional problems from the perspec-
tive of employees working in operating rooms. Hamedan Uni-
versity of Medical Sciences Journal; 12(47)
O’Driscoll M, Allan H, Smith P. (2010). Still looking for leader-
ship–Who is responsible for student nurses’ learning in prac-
tice? Nurse Education Today; 30(3):212-7
Omidvar S, Bakouee F, Salmalian H. (2010). Clinical education
problems: the viewpoints of midwifery students in Babol Uni-
versity of Medical Sciences. Iranian Journal of Medical Educa-
tion; 5(2):15-. [Persian]
Operating room and anesthesia, Introduction of operation
room. Available from: URL; http:// www.mums.ac.ir/ornanesn/
fa/historyOR. Accessed: 27/5/2017
Riley R, Manias E (2002) Foucault could have been an operat-
ing room nurse. J Adv Nurs 39: 316-24 -15
Sadeghi A (2011). “A case study: the association between
organizational culture with management knowledge in
Hasheminezhad hospital – Tehran. Of cial Journal of the
organs of administration of the hospitals in Iran, Issue 2, sum-
mer. No.37:1-8
Tanner J, Timmons S (2000) backstage in the theatre. J Adv
Nurs 32: 975-80
Tazakori, Z. Mehri, S.Mobaraki, N.Dadash L. Ahmadi Y. Shokri,
F.Hamrang, L. (2016). Factors Affecting on Quality of Clini-
cal Education from Perspectives of Operating Room Students.
Journal of Health and Care; 17 (2): 128 -136. [In Persian]
Zeighami R Faseleh M Jahanmiri Sh Ghodsbin F. (2004). Nurs-
ing student’s viewpoint about problems of clinical teaching.
The Journal of Ghazvin University of Medical Science; 8(30):
51-5. [Persian]