
Health Science
Communication
Biosci. Biotech. Res. Comm. 10(3): 398-403 (2017)
Effect of educational intervention based on health
promotion model (HPM) on promoting behavior in safe
delivery among Afghani pregnant women refugees in
Sirjan, Iran
Reza Sadeghi
1
, Mostefa Shamsi
2
, Fatemeh Baghernezhad Hesary
3
and Victoria Momenabadi
4
*
1
PhD Candidate Scholar of Health Education and Health Promotion, Sirjan Faculty of Medical Sciences,
Kerman University of Medical Sciences (KMU), Kerman, Iran
2
MSc in Health Services Administration, Kerman University of Medical Sciences, Kerman, Iran
3
PhD Candidate Scholar of Health Education and Promotion, Social Determinates of Health Research, Birjand
University of Medical Sciences, Birjand, Iran
4
PhD Candidate Scholar of Health Education and Health Promotion, Department of Health Education and
Health Promotion, Faculty of Public Health, Shiraz University of Medical Sciences, Shiraz, Iran
ABSTRACT
Health promotion behaviors can promote physical and psychological health in individuals and population, especially in Afghan Preg-
nant Women. Therefore, this study performed to recognize the Effect of Educational intervention Based on Health Promotion Model
(HPM) on promoting behavior in Safe Delivery among Afghan Pregnant Women in Sirjan city, 2016. This was a quasi- experimental
study. 120 Pregnant Afghan Women attending health centers in Sirjan city were selected to participate in this study: (60 in intervention
group and 60 in control group). The intervention was conducted over two sessions in 60 minutes. Data were collected by a validated and
reliable questionnaire (39 questions) before intervention and three months after intervention. Data was analyzed by chi-square, Fisher’s
exact, paired t-test and independent t-test. The average scores of both groups indicated that health-promoting behavior, perceived self-
ef cacy, perceived barriers, perceived bene ts, perceived social support and interpersonal norms, had no meaningful differences before
the intervention. But after education, the average scores of all variables increased meaningfully in the intervention group (P<0.001). But,
there was no increase or signi cant difference in the control group. HPM was effective in educating Afghan Pregnant Women. Therefore,
it is suggested that HPM can be used to improve the safe delivery in Afghan women.
KEY WORDS: HEALTH PROMOTION MODEL, AFGHAN PREGNANT WOMEN, SAFE DELIVERY, SIRJAN
398
ARTICLE INFORMATION:
*Corresponding Author: vici.momeni@yahoo.com
Received 12
th
June, 2017
Accepted after revision 10
th
Sep, 2017
BBRC Print ISSN: 0974-6455
Online ISSN: 2321-4007 CODEN: USA BBRCBA
Thomson Reuters ISI ESC and Crossref Indexed Journal
NAAS Journal Score 2017: 4.31 Cosmos IF: 4.006
© A Society of Science and Nature Publication, 2017. All rights
reserved.
Online Contents Available at:
http//www.bbrc.in/
DOI: 10.21786/bbrc/10.3/10
Reza Sadeghi etal.
INTRODUCTION
Maternal and infant mortality due to complications of
pregnancy is a very important health indicator. What-
ever the percentage of deliveries in non-sanitary and
out-of-hospital increase, the mortality rate of infants
and pregnant women and neonatal tetanus infection will
increase too (Wax etal., 2010). Great deals of investment
have been spent to reduce maternal and infant mortality
rate and to reach the World Health Organization goal in
the country, and also maternity and childbirth facilities
have been built in various parts of Iran (Karyani etal.,
2015).
One of the most vulnerable groups in this regard is
refugees Afghan pregnant women. Decades of war and
internal con ict in Afghanistan has led to migrate a
large number of Afghans to neighboring countries,
including Iran. One of the problems of these immigrants
in Iran is the high rates of non-safe and non-sanitary
delivery despite the availability of maternity facilities
(Kala etal., 2002). Even in the Sirjan city in spite of
the existence of maternity and women’s specialists and
well-equipped midwifery, 67% of Afghan women deliver
babies at home in unsanitary conditions and by non-
specialists, while this rate of giving birth at home is only
1% in developed countries (Sadeghi etal., 2015b). But in
some developing countries, this ratio reaches to 50% or
even more (Gloyd etal., 2001).
In the different studies, several reasons have been
mentioned for giving birth at home, including high cost
of delivery in the hospital, Fear of the hospital, hus-
band’s opposition, wrong culture, mother’s emotional
support at home and fear of cesarean section (Salehi and
Pour, 2002).
The changing of this risky behavior in Afghan
pregnant women requires proper education. The value
of education depends on its Effectiveness and chang-
ing or creation of health behaviors, which is possible
with the proper use of theories and educational models
(Glanz etal., 2008). Theories identify the main factors
that had in uenced in question behaviors, specify the
relationships between these factors, and outline the cir-
cumstances, the manner and the time of the occurrence
of these relationships. Therefore, theories are useful in
identifying the elements that should be considered as the
main axis of interventions (Sadeghi etal., 2016). Health
Promotion Pender Model is one of the comprehensive
and predictive models which is used to study the health
promoting behaviors and provides a theoretical frame-
work for discovering affected factors in these behaviors
(Pender, 2011).
The determinants of health promotion behaviors con-
cepts in this model include: 1) individual experiences
and Characteristics, 2) emotions and behavioral speci c
cognition, and 3) behavioral outcomes. The concept of
individual experiences and Characteristics is a concept
that directly or indirectly in uences on the behaviors
through cognition and behavioral emotions, including
personal factors and previous related behaviors. While
the concept of cognition and behavioral speci c emo-
tions directly in uence on the behaviors and include
constructs such as perceived bene ts and barriers, per-
ceived self-ef cacy, behavioral emotions, interpersonal
in uences, and situational in uences (Pender, 2011).
Professor Pender has identi ed models that have
in uenced on explanation of behavior in over 50% of
the researches, including personal factors (perceived
health status), perceived bene ts, perceived barriers,
perceived self-ef cacy and interpersonal in uences
(Social support) (Pender, 2011).
Several studies have con rmed the effectiveness of
this model. In this regard, a study by Morowati Shari-
fabad et al aimed at optimizing the health promotion
model indicated that perceived self-ef cacy was the
most important determinant of health promotion behav-
iors and also perceived religious support was directly
and indirectly have been effective by in uencing on
perceived self-ef cacy, perceived bene ts, perceived
barriers, and perceived importance of health promotion
behaviors (Morowati etal., 2005). The results of Magli-
one et al. showed that individuals with higher levels
of social support, self-ef cacy and with commitment
of planning are more physically active (Maglione and
Hayman, 2009). Considering the importance of the safe
delivery and due to the high rate of delivery at Afghani
homes; it seems that a similar study has not done in this
regard. Therefore, the present study aimed to investigate
the effect of educational intervention using the health
promotion model in promoting behavior of Safe delivery
among refugees Afghan Pregnant Women in Sirjan city
in 2016.
MATERIALS AND METHODS
This quasi- experimental study was conducted in 2016.
The research environment was the health centers of Sir-
jan city and the study population was Afghani preg-
nant women. Subjects were selected by simple random
sampling. The sample size was calculated by using the
ratio difference formula by considering the con dence
level of 95%, a power of 80%, and about 3/3 differences
in score before and after the intervention with a stand-
ard deviation of 7 and 52 subjects in per group, but the
sample size was nally calculated as 60 subjects with
consideration of 10 percentage of possible number of
subjects dropping out in each group (Mohammadipour
etal., 2015).
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS EFFECT OF EDUCATIONAL INTERVENTION BASED ON HEALTH PROMOTION MODEL 399
Reza Sadeghi etal.
The subjects were selected based on the inclusion cri-
teria which were as follows: Afghans, being pregnant in
the third up to fth month and resident of Sirjan city;
the exclusion criteria were: without chronic disease such
as pregnancy diabetes and high blood pressure, non-
residence until the end of pregnancy and unwilling to
participate in the study. Data collection tool was a self-
administered questionnaire. The questionnaires were set
anonymously and encoded and were arranged in three
parts. The rst part contains the demographic character-
istics including 5 questions about age, education, occu-
pation, number of pregnancies, and residence. The sec-
ond part was related to the evaluation of the structures of
the Pender Health Promotion Model. This part contains
seven questions for perceived bene ts, seven questions
of perceived barriers, seven questions of perceived self-
ef cacy, six questions of perceived interpersonal norms,
and six questions of perceived social support structures.
The third part was related to the measurement of safe
delivery behavior. The questions were scored as follows.
questions about perceived bene ts, perceived barriers,
perceived self-ef cacy, interpersonal norms and per-
ceived social support were scored 1-3 by Likert’s trilogy
scale as agree (score 3) to disagree (score 1), The range
of scores for perceived bene ts, perceived barriers and
perceived self-ef cacy were from 7 to 21 and for inter-
personal norms and perceived social support was from
6 to 18. Also, the assessments of safe delivery behavior
were of yes/no type questions.
In this research the analyzing the validity of the con-
tent method was used for the analyzing the validity of
the questionnaires. The questionnaire was approved by
healthcare professionals to examine the issue’s compre-
hensiveness. The re-test method was also used in the
distance of 2 weeks to determine the reliability of the
study. The correlation coef cient has calculated between
the two-time responses as follows, for perceived bene ts,
0.79, perceived barriers, 0. 77, perceived self-ef cacy,
0.74, perceived interpersonal norms, 0.84 and perceived
social support, 0.81.
The method was as follows the researchers randomly
divided subjects into intervention and control groups
after the selection them based on inclusion criteria. At
rst, the pre-test questionnaire was completed by the
interviewer, then the education program was conducted
for the intervention group. Educational content included
the de nition of pregnancy, maternity care, and also the
bene ts of safe delivery.The educational program was
conducted for four groups of 15 subjects (60 subjects
in intervention group), which consisted of two, one-
hour training sessions in a one-month interval that were
held in a lecture and group discussion. Also, an indi-
vidual counseling was held for a pregnant woman and
their family. The educational classes were held in health
centers and health care homes. After three months of
conducting the classes, post-test questionnaires were
completed by the researcher for the patients in the inter-
vention and control groups.
The current research has been approved by the Eth-
ics Committee of the Kerman University of medical sci-
ences (ethics code: IR.KMU. REC. 1396.11). All the par-
ticipants were voluntarily and consciously participated
in the study and they were given the assurance that the
information has been collected only in order to be used
for research and will remain con dential and the written
testimonial had been gotten from all of the participants
in order to participate in the study. Meanwhile, although
the control group was not under educational interven-
tion, but after completing the post-test, educations were
provided to them with the same quantity and quality.
Data were analyzed by using Chi-square, Fisher’s
exact test, independent t-test and paired t-test through
SPSS version 16. The signi cance level was considered
less than 0.05.
RESULTS AND DISCUSSION
In this study, 120 participants were randomly divided
into two groups, intervention (n = 60) and control (n =
60) then the mean and standard deviation of the ages of
subjects in the study and control groups were analyzed
and they were respectively 24.83 ± 9.43 and 25.12 ± 9.26
years old. This difference based on independent t-test
did not show signi cant differences in both intervention
and control groups (P = 0.426). Also other demographic
characteristics of the population did not show any sig-
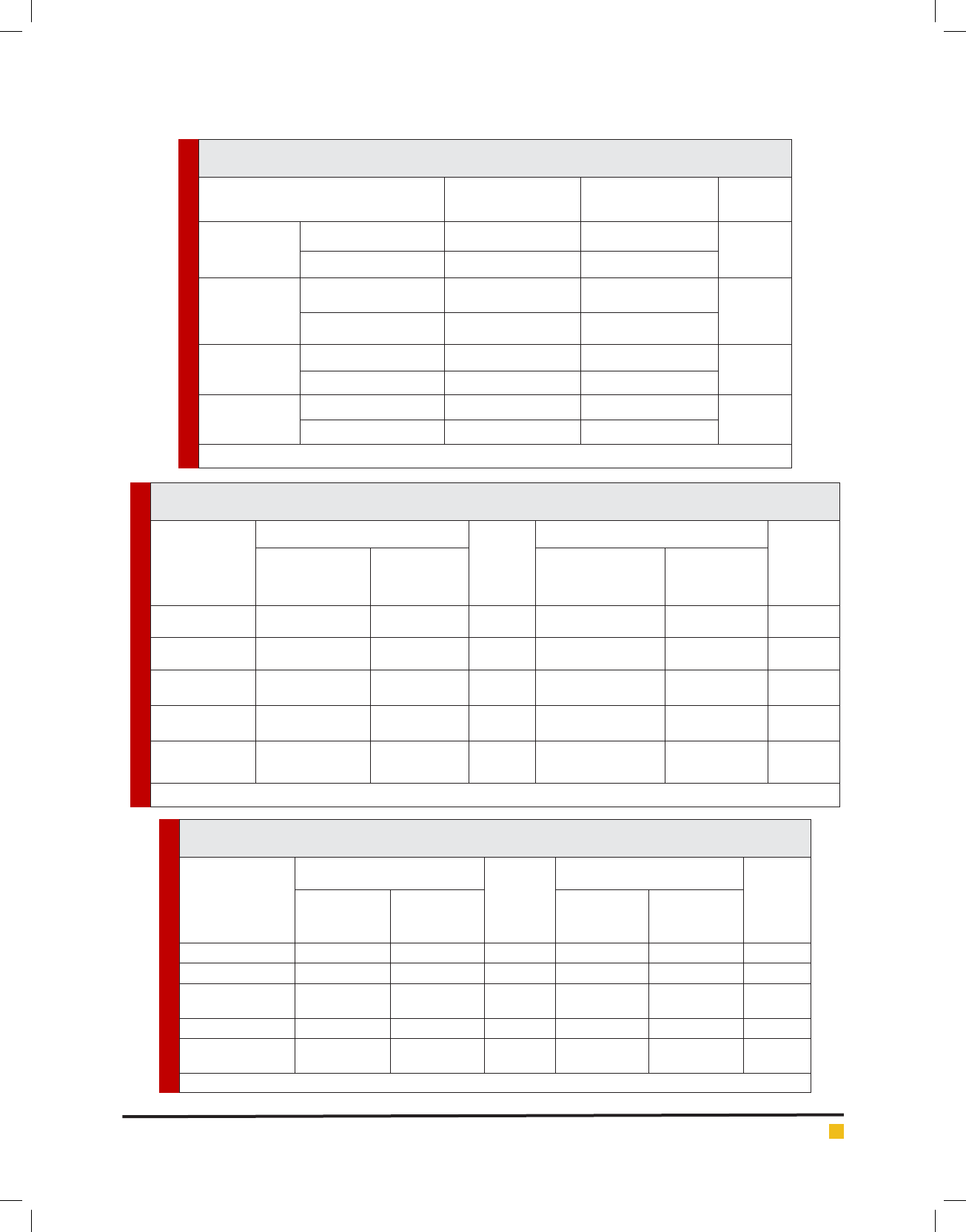
ni cant differences between the two groups (Table 1).
The results showed that there wasn’t any signi cant
difference between the mean scores of perceived ben-
e ts, perceived barriers, perceived self-ef cacy, inter-
personal norms and perceived social support before the
intervention in the intervention and control groups, but
after the intervention, the differences were signi cantly
clear and Scores were increased (Table 2).
The statistical results showed that in the study group,
there was a signi cant increase between the mean scores
of perceived bene ts, perceived barriers, perceived self-
ef cacy, interpersonal norms and perceived social sup-
port before and after the intervention, and also the
educational intervention was effective (Table 3) .
The results also showed that the safe delivery behav-
ior in the intervention group have increased from 23%
to 57% after the educational intervention.
Afghan women carry out childbirth at home and in
unhealthy conditions, due to traditional beliefs and mis-
conceptions of them and their followers, which unfor-
tunately can lead to the death of mother or infant and
may lead to complications such as neonatal tetanus.
400 EFFECT OF EDUCATIONAL INTERVENTION BASED ON HEALTH PROMOTION MODEL BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS EFFECT OF EDUCATIONAL INTERVENTION BASED ON HEALTH PROMOTION MODEL 401
Reza Sadeghi etal.
Table 1. Comparing some variables among the refugees Afghan Pregnant Women in Sirjan city in the
control and intervention groups
Variable
intervention Group
(n= 60) Number (%)
Control Group
(n= 60) Number (%)
*p-value
Occupation
Housewife 55 (50.4) 54 (49.6)
0.251
Employed 5 (45.4) 6 (54.6)
Pregnancy status
First pregnancy 12 (52.1) 11 (47.9)
0.925
More than one pregnancy 48 (49.4) 49 (50.6)
Education
Literate 10 (47.6) 11 (52.4)
0.712
illiterate 50 (50.5) 49 (49.5)
Residence
City
28 (49.1) 32 (50.8)
0.283
Village
29 (50.9) 31 (49.2)
*Chi-square test
Table 2. The mean scores of refugees Afghan Pregnant Women in Sirjan between the control and intervention groups
regarding Safe Delivery before and after the intervention
Before intervention (n=60)
p-value*
After intervention (n=60)
p-value*
Intervention
group Mean± SD
Control group
Mean± SD
Intervention group
Mean± SD
Control group
Mean± SD
perceived bene ts
12.14±2.21 11.94±1.87 0.212 18.42±0.64 12.02±1.56 <0.001
Perceived barriers
18.82±2.72 18.41±3.09 0.367 14.77±1.46 18.25±3.11 <0.001
perceived
self-ef cacy
12.94±3.23 12.64±4.37 0.055 17.18±1.39 12.29±3.85 <0.001
interpersonal
norms
10.19±2.61 10.71±2.83 0.412 14.21±1.67 11.14±2.78 <0.001
perceived social
support
7.24±2.43 7.58±2.67 0.216 14.12±3.73 7.68±2.83 <0.001
*Independent t-test
Table 3. The comparison of the variables. The mean scores of refugees Afghan Pregnant Women in Sirjan
between the control and intervention groups regarding Safe Delivery before and after the intervention
Intervention group (n=60)
p-value*
Control group (n=60)
p-value*
Before
Intervention
Mean± SD
After
intervention
Mean± SD
Before
Intervention
Mean± SD
After
intervention
Mean± SD
perceived bene ts 12.14±2.21 18.42±0.64 <0.001 11.94±1.87 12.02±1.56 0.021
Perceived barriers 18.82±2.72 14.77±1.46 <0.001 18.41±3.09 18.25±3.11 0.424
perceived self-
ef cacy
12.94±3.23 17.18±1.39 <0.001 12.64±4.37 12.29±3.85 0.356
interpersonal norms 10.19±2.61 14.21±1.67 <0.001 10.71±2.83 11.14±2.78 0.172
perceived social
support
7.24±2.43 14.12±3.73 <0.001 7.58±2.67 7.68±2.83 0.481
*Paired t-test
402 EFFECT OF EDUCATIONAL INTERVENTION BASED ON HEALTH PROMOTION MODEL BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
Reza Sadeghi etal.
Therefore, in order to control this important and fun-
damental dilemma, we evaluated the relevant train-
ing based on the health promotion model to promote
safe delivery behavior.The ndings showed signi cant
increase in the safe and hygienic delivery of Afghan
women from 23% to 57% in Sirjan city.
In the health promotion model, in the intervention
group, all of the constructs of the model showed signi -
cant differences after the intervention.
In the health promotion model, perceived bene ts are
as a direct stimulus action of behavior and the adop-
tion of an action to prevent the problem or action on a
health behavior are dependent on its perceived bene ts
(Pender, 2011). The most important perceived bene ts of
safe delivery of Afghan pregnant women respectively
included the baby’s health, their health, and the pre-
vention of unwanted childhood complications at home.
In the present study, the average of perceived ben-
e ts scores of patients in the intervention group has
increased signi cantly than in the control group after
the education, which was consistent with the results of
similar studies (Morovati, 2007, Leslie etal., 2000, Sad-
eghi etal., 2014). But the results of the study of Ghaffari
etal was inconsistent to the present study and did not
indicate an increase in the average score of perceived
bene ts (Ghafari, 2007).
In the present study, nancial problems, lack of
medical insurance and lack of access to facilities were
respectively the most important obstacles in the target
group. The signi cant reduction in the average score
of perceived barriers after educational intervention and
inter-sectional collaboration in the health care sys-
tem indicates that the education has a positive effect
on removing the perceived barriers in the intervention
group. The studies of Nowroozi et al. (Noroozi et al.,
2011) and Karimi etal. (Karimi and Eshrati, 2012), which
were conducted with this model, indicate that educa-
tional intervention are effective in reducing perceived
barriers.
Self-ef cacy is referred to a person’s con dence to his
ability in performing an action (Bandura, 2006). In the
present study, the average of self-ef cacy score of the
experimental group after the intervention was signi -
cantly increased, which were consistent with the studies
of Morowati etal. (Morowati etal., 2005) and Sadeghi
etal. (Sadeghi etal., 2015a), but they contradicted by the
ndings of Kinsler etal. (Kinsler etal., 2004).
Also, in the study, after the education, the aver-
age scores of the interpersonal norms of the interven-
tion group were signi cantly higher than in the con-
trol group, which was consistent with the results of the
studies of Chenari etal (Chenary etal., 2013) and Nos-
ratabadi etal (Nosratabadi etal., 2015). In the present
study, perceived social support was considered as the
most important determinant of the behavior of delivery
at home, which this issue was arisen from the in uences
of family and relatives on this unhealthy behavior. But
after educational sessions for the participants and their
relatives, the average score in the intervention group was
signi cantly higher than in the control group, which is
consistent with the results of conducted studies with this
model (Lusk etal., 1997, Norouzi etal., 2010). Accord-
ing to this research and the ndings, it is suggested that
a precise educational program should be carried out
based on the health promotion model for Afghan preg-
nant women, their spouses and their relatives, and plan-
ners should train them by using individual and group
educational methods, in order to solve their nancial
and health problems, and to prevent the risks of unsafe
deliveries at home.
One of the limitations of this study was the problem
of Afghan women’s language and their accent, which
was solved by Afghan inquirer and educator, as well
as Unwillingness of some of the women to participate
in the study, which it was solved by convincing them
through local clerks and Afghan elders. Another limita-
tion of the study was the nancial and insurance prob-
lems of Afghan women, which it was reduced by inter-
agency co-ordinations.
CONCLUSION
The results of this study indicates the impact of educa-
tional intervention based on the health promotion model
on increasing the safe delivery of pregnancy in Afghan
pregnant women in Sirjan city. education and interven-
tion based on the health promotion model is helpful and
effective to enhance awareness, to change the attitude
and to adopt preventive behaviors for unsafe delivery
at home.
ACKNOWLEDGMENTS
Researchers acknowledge the Faculty of Medical Sci-
ences Research Committee of Sirjan city and Research
Deputy of Kerman medical university, related staffs in
health centers of Sirjan as well as all Afghan pregnant
women who are participating in this study.
AUTHORS’ CONTRIBUTIONS
RS helped design the study, carried out data collection,
data analysis, and drafted the manuscript. VM carried
out the statistical analysis and interpretation. MS con-
ceived the study, supervised the data collection and
analyses, and helped draft the manuscript. BB edited
and commented on the nal draft. All authors read and
approved the nal manuscript.

BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS EFFECT OF EDUCATIONAL INTERVENTION BASED ON HEALTH PROMOTION MODEL 403
Reza Sadeghi etal.
CONFLICT OF INTEREST
The authors declare no con icts of interest.
REFERENCE S
bandura, A. 2006. Guide For Constructing Self-Ef cacy Scales.
Self-Ef cacy Beliefs Of Adolescents, 5.
Chenary, R Noroozi, A. & Tahmasebi, R 2013. Effective Fac-
tors Of Health Promotion Behaviors Based On Health Promo-
tion Model In Chemical Veterans Of Ilam Province In 2012-13.
Www. Sjimu. Medilam. Ac. Ir, 21, 257-267.
Ghafari, M. 2007. Comparing The Ef cacy Of Health Belief
Model And Its Integrated Model In Aids Education Among
Male High School Students In Tehran. A Thesis For Degree Of
Phd, Tehran: Tarbiat Modares University.
Glanz, K., Rimer, B. K. & Viswanath, K. 2008. Health Behavior
And Health Education: Theory, Research, And Practice, John
Wiley & Sons.
Gloyd, S., Floriano, F., Midwife, M. S., Chadreque, M. A.,
Nyangezi, J. M. & Platas, A. 2001. Impact Of Traditional Birth
Attendant Training In Mozambique: A Controlled Study. Jour-
nal Of Midwifery & Women’s Health, 46, 210-216.
Kala , Y., Hagh-Shenas, H. & Ostovar, A. 2002. Mental Health
Among Afghan Refugees Settled In Shiraz, Iran. Psychological
Reports, 90, 262-266.
Karimi, M. & Eshrati, B. 2012. The Effect Of Health Promotion
Model-Based Training On Promoting Students’ Physical Activ-
ity. Journal Of Kermanshah University Of Medical Sciences (J
Kermanshah Univ Med Sci), 16, 192-200.
Karyani, A. K., Azami, S. R., Rezaei, S., Shaahmadi, F. & Ghaz-
anfari, S. 2015. Geographical Distribution Of Gynecologists
And Midwives In Kermanshah Province (2008-2013). Journal
Of Kermanshah University Of Medical Sciences (J Kermanshah
Univ Med Sci), 19, 294-302.
Kinsler, J., Sneed, C. D., Morisky, D. E. & Ang, A. 2004. Evalu-
ation Of A School-Based Intervention For Hiv/Aids Prevention
Among Belizean Adolescents. Health Education Research, 19,
730-738.
Leslie, E., Fotheringham, M., Owen, N. & Veitch, J. 2000. A Uni-
versity Campus Physical Activity Promotion Program. Health
Promotion Journal Of Australia: Of cial Journal Of Australian
Association Of Health Promotion Professionals, 10, 51.
Lusk, S. L., Ronis, D. L. & Hogan, M. M. 1997. Test Of The
Health Promotion Model As A Causal Model Of Construction
Workers’ Use Of Hearing Protection.
Maglione, J. L. & Hayman, L. L. 2009. Correlates Of Physical
Activity In Low Income College Students. Research In Nursing
& Health, 32, 634-646.
Mohammadipour, F., Izadi, T. A., Sepahvand, F. & Naderifar,
M. 2015. The Impact Of An Educational Intervention Based On
Pender’s Health Promotion Model On The Lifestyle Of Patients
With Type Ii Diabetes.
Morovati, M. 2007. The Effectiveness Of Modi ed Health Pro-
motion Model In Change Of Health Promotion Behaviors In
The Yazd Elderly. Tehran: Tarbiat Modares University.
Morowati, S., Ghofranipour, F., Hidarnia, A. & Babaee-Ruchi,
G. 2005. Modi cation Of Health Promotion Model And Its
Application Together With Adult Education Theory In Chang-
ing Health Promoting Behaviors Of Older Adults In Yazd. J
Med Tarbiat Modares U-Ni, 21, 54-8.
Noroozi, A., Tahmasebi, R. & Ghofranipour, F. 2011. Effect Of
Health Promotion Model (Hpm) Based Education On Physical
Activity In Diabetic Women. Iranian Journal Of Endocrinology
And Metabolism, 13, 361-367.
Norouzi, A., Ghofranipour, F., Heydarnia, A. & Tahmasebi,
R. 2010. Determinants Of Physical Activity Based On Health
Promotion Model (Hpm) In Diabetic Women Of Karaj Diabetic
Institute. Ismj, 13, 41-51.
Nosratabadi, M., Halvaiepour, Z. & Sadeghi, R. 2015. Exploring
The Relationship Between Social Capitals, And Social Support
With Mother’s Health In Mothers Referring To Health Centers
Of Sirjan City: A Structural Model. Journal Of Urmia Nursing
And Midwifery Faculty, 13, 781-790.
Pender, N. J. 2011. Heath Promotion Model Manual.
Sadeghi, R., Khanjani, N., Hashemi, M. & Movagheripour,
M. 2014. Using Health Belief Model To Prevent Skin Cancer
Among Farmers. Iranian Journal Of Health Education And
Health Promotion, 2, 215-222.
Sadeghi, R., Mazloomy, S., Hashemi, M. & Rezaeian, M. 2016.
The Effects Of An Educational Intervention Based On The
Health Belief Model To Enhance Hiv-Preventive Behaviors
Among Male Barbers In Sirjan. Journal Of Rafsanjan Univer-
sity Of Medical Sciences, 15, 235-246.
Sadeghi, R., Rezaeian, M., Khanjani, N. & Iranpour, A. 2015a.
The Applied Of Health Belief Model In Knowledge, Attitude
And Practice In People Referred For Diabetes Screening Pro-
gram: An Educational Trial. Journal Of Rafsanjan University
Of Medical Sciences, 13, 1061-1072.
Sadeghi, R., Rezaeian, M. & Mohseni, M. 2015b. The Effect Of
An Educational Program Based On Basnef Model On Breast
Self-Examination Practice Of 20-45-Year-Old Women In Sir-
jan City: A Training Trial Study.
Salehi, M. & Pour, Z. G. 2002. Reasons For Zahedan’s Women
For Not Referring To Delivery Ward For Child Delivery. Journal
Of Reproduction & Infertility, 3.
Wax, J. R., Lucas, F. L., Lamont, M., Pinette, M. G., Cartin, A.
& Blackstone, J. 2010. Maternal And Newborn Outcomes In
Planned Home Birth Vs Planned Hospital Births: A Metaanaly-
sis. American Jo urnal Of Obstetrics And Gynecology, 203, 243.
E1-243. E8.