
Medical
Communication
Biosci. Biotech. Res. Comm. 9(4): 756-761 (2016)
Risk factors associated with hepatitis B virus disease
in different states of North Eastern India and their
distribution
Namrata Kumari
1
, Priyanka Kashyap
1
, Snigdha Saikia
1,2
, Kangkana Kataki
1
,
Subhash Medhi
1
, Bhavadev Goswami
2
, Premashis Kar
3
, Th. Bhimo Singh
4
, K.G Lynrah
5
,
M. R. Kotowal
6
, Pradip Bhaumik
7
, Moji. Jini
8
and Manab Deka
1
1
Bioengineering and Technology Department, Gauhati University, Guwahati, Assam
2
Department of Gastroenterology , Gauhati Medical College, Guwahati, Assam
3
Department of Medicine, Maulana Azad Medical College, New Delhi
4
Department of Medicine, Regional Institute of Medical Sciences Regional Medical College,Imphal
5
Deptartment of Medicine, NEIGRIHMS, Shillong, Meghalaya
6
Medical Adviser to the Hon’ble Chief Minister of Sikkim, STNM Hospital, Gangtok, Sikkim
7
Dept of Medicine, Agartala Govt. Medical College, Agartala, Tripura.
8
Directorate of Medical Education , General Hospital, Naharlagun, Arunachal Pradesh.
ABSTRACT
To determine whether risk factors such as fever, anorexia, abdominal discomfort, haematemesis, weight loss, high coloured urine,
blood transfusion, alcoholic intake and multiple sexual partners are highly associated and derive a novel risk score for the devel-
opment of HCC. Different liver diseases were screened for the positivity of HBsAg were were followed up (mean Age and SD) for
the occurrence of HCC. The risk factors were recorded and found the statistical signi cant with the disease. The distribution of the
different categories of HBV disease in six different states of Northeastern India region were recorded .The number of Chronic cases
are found as the highest followed by Acute viral hepatitis, cirrhosis, HCC and FHF. The mean Age±SD of HCC was was recorded as
53.3 ± 9.57 which was greater than other study groups of HBV. The risk factors such as fever, high coloured urine, blood transfu-
sion and Multiple sexual partners were recorded as mostly signi cant(p<0.05). These risk factors are closely associated with the
progression of the liver diseases than other recorded in this study . The other risk factors were also recorded and the values were
not found as a highly associated but may be increase up to a level . The risk score, based on the present and absent of the factors
can estimate the chance of development of HCC in few years . It can be used to identify high-risk CHB patients for treatment and
screening of HCC.
756
ARTICLE INFORMATION:
*Corresponding Author: namrata388@gmail.com
Received 14
th
Sep, 2016
Accepted after revision 15
th
Dec, 2016
BBRC Print ISSN: 0974-6455
Online ISSN: 2321-4007
Thomson Reuters ISI ESC and Crossref Indexed Journal
NAAS Journal Score 2015: 3.48 Cosmos IF : 4.006
© A Society of Science and Nature Publication, 2016. All rights
reserved.
Online Contents Available at: http//www.bbrc.in/
Namrata Kumari et al.
INTRODUCTION
Hepatitis B is a public health problem and more than
350 millionpeople are said to be infected with the hepa-
titis B virus worldwids (Kim et. al., 2016) . Hepatitis B
virus infection is mainly associated with an acute liver
disease which includes liver failure and also chronic-
ity which can lead to cirrhosis and liver cancer (Liang
et. al., 2009). Hepatitis B virus (HBV) is a major blood-
borne and sexually transmitted infectious agent that is
a signi cant global public health issue Currently, eight
HBV genotypes (A-H) have been described and diverge
by at least more than eight per cent in their nucleotide
sequences (Kramvis et. al., 2005). The occult hepatitis B
virus infection is de ned as “the presence of HBV DNA
in the liver (with detectable or undetectable HBV DNA
in serum) in individuals testing HBsAg negative by cur-
rently available assays” (Raimondo 2008; Hollinger 2010
and Metaferia et. al., 2016).
Earlier, naturally occurring deletions in the pre-S2/S
promoter region were observed in several cases of occult
HBV infection (Chaudhuri 2004; Mu 2009), chronic HBV
infection (Fan et al., 2001), and patients with progressive
liver diseases (Chen et. al.,2006) . In a subsequent study, it
was demonstrated that these deletions can cause altered
surface protein expression, and an increased large-
HBsAg (L-HBsAg) to major/small-HBsAg (S-HBsAg)
ratio leading to reduced HBsAg secretion (Sengupta
et al., 2007).
HBV is spread predominantly by percutaneous or
mucosal exposure to infected blood and other body u-
ids with numerous forms of human transmission. The
sequelae of HBV infection include acute and chronic
infection, cirrhosis of the liver and primary liver can-
cer. The likelihood of progression to chronic infection is
inversely related to age at the time of infection. Around
90% of infants infected perinatally become chronic car-
riers, unless vaccinated at birth. The risk for chronic
HBV infection decreases to 30% of children infected
between ages 1 and 4 years and to less than 5% of per-
sons infected as adults (McQuillan 1999; Wasley 2010).
Healthcare personnel are at increased risk of occupa-
tional acquisition of hepatitis B virus (HBV) infection.
While effective vaccination for HBV is widely available,
the prevalence of HBV and vaccine acceptance in hospital
personnel have not been recently assessed.Some liver dis-
eases are potentially preventable and are associated with
lifestyle choices. Alcohol-related liver disease is due to
excessive consumption and is the most common prevent-
able cause of liver disease.Hepatitis B is a viral infection
most often spread through the exchange of bodily u-
ids (for example, unprotected sexual intercourse, sharing
unsterilized drug injecting equipment, using non-steri-
lized equipment for tattoos or body piercing).
The hereditary liver disease can be passed geneti-
cally from generation to generation. Examples include
Wilson’s disease (copper metabolism abnormalities) and
hemochromatosis (iron overload). Chemical exposure
may damage the liver by irritating the liver cells resulting
in in ammation (hepatitis), reducing bile ow through
the liver (cholestasis) and accumulation of triglycerides
(steatosis). Obesity/overweight increases the risk for liver
disease. Obesity often results in the accumulation of fat
cells in the liver. Acids that are secreted by these fat
cells (called fatty acids) can cause a reaction in the body
that destroys healthy liver cells and results in scarring
(sclerosis) and liver damage.From previous studies in
Ethiopia have demonstrated that the important factors
of HBV transmission include blood transfusion; tattoo-
ing; a history of surgery, unsafe injections, or abortions;
multiple sexual partners; and traditional practices such
as scari cation, circumcision, and also ear piercing
(Awole 2005; Walle 2008; Ramos 2011; Zenebe 2014;
Tegegne 2014) .Although the association between HIV
and HBV has become less prominent in Africans, evi-
dence has been found indicating that HIV makes HBV-
related liver disease develop more quickly (Metaferia
et. al., 2007) and HIV/HBV co-infection has serious
effects on both pregnant women and infants. A previous
study among pregnant women in Bahir Dar city showed
an HIV/HBV co-infection rate of 1.3% (Chen et. al., 2006)
. The risk of developing liver disease varies, depending
on the underlying cause and the particular condition.
General risk factors for liver disease include alcoholism,
exposure to industrial toxins, heredity (genetics), and
long-term use of certain medications.
Age and gender also are risk factors for liver disease.
These factors vary, depending on the particular type of
disease. For example, women between the ages of 35
and 60 have the highest risk for primary biliary cirrhosis
and men aged 30-40 are at higher risk for primary scle-
rosing cholangitis.
In our study we have included the following factors
having unprotected sex with more than one partner or
with an infected partner , Having a sexually transmit-
ted disease (STD) ,Using IV (injected) drugs ,Living with
an infected person , Having end-stage kidney disease
and receiving hemodialysis treatments,Being exposed to
human blood at work (e.g., health care workers) .
MATERIAL AND METHODS
Study area: The North-eastern region, where the where
the study was conducted, is a less developed region of
India in terms of economic, social, and health indices.
Insuf cient health services and lack of public awareness
of health-related issues have increased the prevalence of
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS THE RISK FACTORS ASSOCIATED WITH HEPATITIS B VIRUS DISEASE 757
Namrata Kumari et al.
diseases, particularly communicable diseases. In order to
achieve the objectives of the study, we enrolled patients
with various types of liver diseases seen at various par-
ticipating centre of Northeastern states which include
Regional Institute of Medical Sciences, Imphal, Manipur;
Agartala Govt. Medical College, Tripura; STNM Hospi-
tal, Gangtok, Sikkim; Naharlagun General Hospital,
Arunachal Pradesh,Gauhati Medical College, Guwahati,
Assam; NEIGRIHMS, Shillong, Meghalaya .Patients with
HBV infection who had achieved a virological response
were collected and recorded the data since Nov 2012 to
May 2015.
CLINICAL DATA
The patients of AVH were evaluated on the basis of history
and clinical examination. The liver function tests (LFT)
was done at the rst visit. The patients of Acute Viral
Hepatitis (AVH), Fulminant Hepatic Failure (FHF) were
evaluated on the basis of history, physical examination,
liver function test and serological test for HBsAg. Sam-
ples which were positive for HBsAg were also screened
for IgM anti-HBc and HBV-DNA. To rule out any co-
infection with other hepatotropic viruses IgM anti-HAV,
anti-HCV, IgM, anti-HEV infection was done. The patients
of chronic liver disease viz. chronic hepatitis, cirrhosis of
the liver and hepatocellular carcinoma was evaluated on
the basis of history, physical examination, Liver function
pro le, Prothrombin time, serological markers for HBsAg.
Samples which are positive for HBsAg were further tested
for IgG anti-HBc and HBeAg followed by HBV DNA.
Anti-HCV and HCV RNA was done in the cases which are
positive for HBV DNA to rule out cases of co-infection.
The serum of voluntary blood donor was collected from
blood banks of all the hospitals .They were screened for
HBsAg using commercially available ELISA kits (3rd gen-
eration) at each centre.Serum samples from each subject
were stored at -80®C until use. The patients with HCC
cases, the serum samples were collected at the time when
liver biopsy was performed.
Inclusion and Exclusion Criteria for the study:
All those patients who were clinically diagnosed as
Acute Viral Hepatitis (AVH), Fulminant Hepatic Failure
(FHF), chronic active hepatitis (CAH), Cirrhosis, Hepa-
tocellular Carcinoma (HCC) were included in the study.
Voluntary blood donors and Healthcare workers were
also included in this study. Professional blood donors,
high-risk group like IV drug abusers will be excluded
from the study.
EXTRACTION OF HBV DNA
HBV DNA was extracted using slightly modi ed Phenol-
Chloroform method as described by Teresa Santantonio
et al 1991. Brie y the method involves 100 μl of serum
sample incubated with 0.5% SDS, 10mM Tris-HCl (pH-
7.5), 10mm EDTA & 10mg / ml Proteinase K at 37°C
overnight. Then the serum DNA would be extracted
twice with Phenol / Chloroform and precipitated with
ethanol in the presence of 30 μg of tRNA. The pallet was
air dried and resuspended in 25 μl of distilled water.Part
of the surface gene (nucleotide position 425 to position
840) was ampli ed by nested polymerase chain reaction
(PCR) for the HBV DNA.
Study design
Before starting the study, approval from the local ethi-
cal committee was received, and those subjects over the
age of 15 who had consented to participate in the study
were included. Informed consent forms, as well as infor-
mation about the aims of the study, were provided for
each subject. Age, residence site (rural/urban), a level of
education, and marital status of the subjects, and any
family history of jaundice were recorded.
Statistical analysis
Categorical variables of HBV diseases were reported as
a number of cases and were grouped into states. The
statistical analysis was done by using the SPSS version
13.1 to con rm the association.For the descriptive anal-
yses, we calculated the values and were presented as
either a number (percent;%) or mean SD (standard devi-
ation). Statistical signi cance levels were determined by
two-tailed tests and considered the signi cant P value <
0.05 (p < 0.05). Statistical analysis data were plotted in
excel.
RESULTS AND DISCUSSION
DEMOGRAPHICS AND OUTCOMES
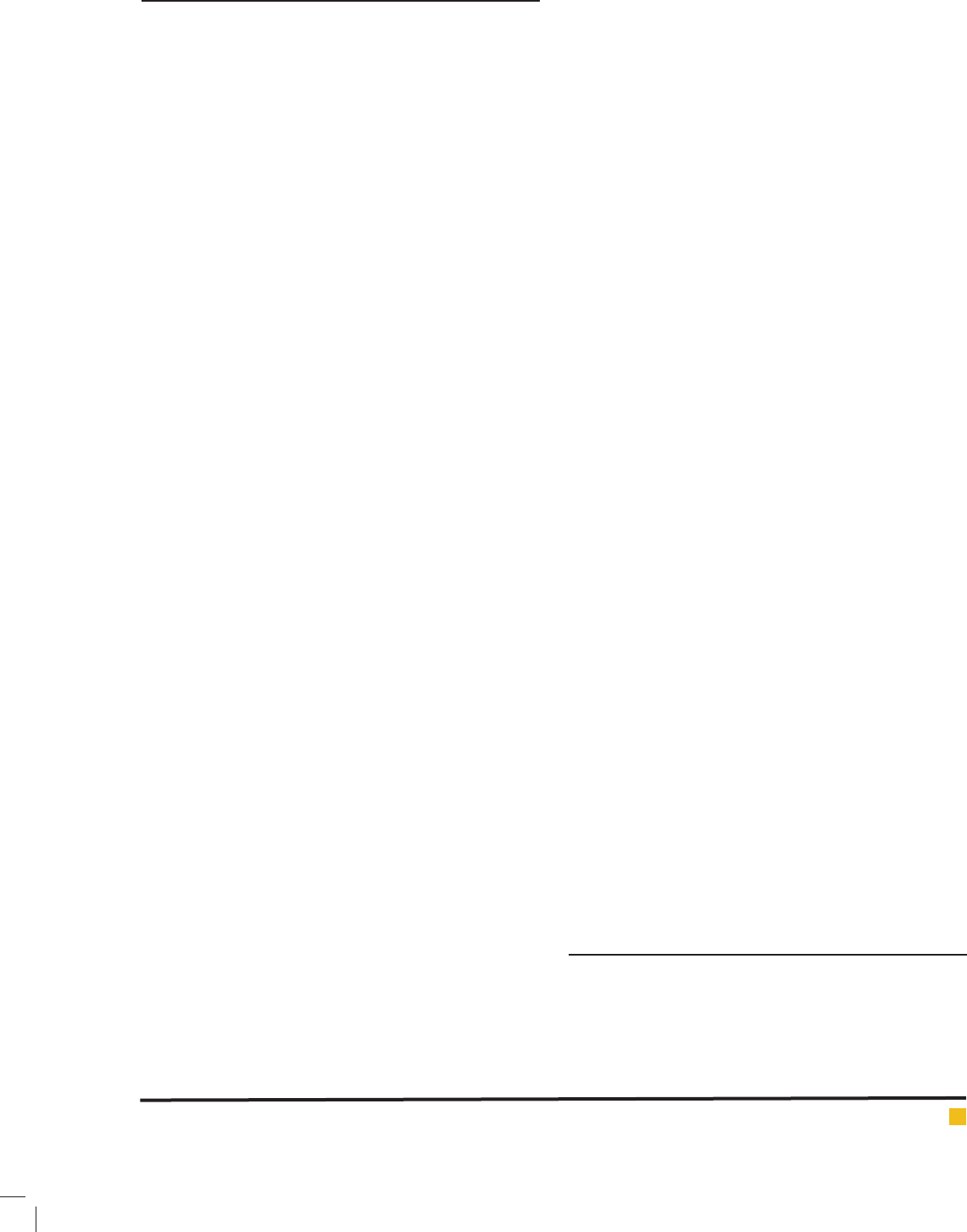
The distribution of the different categories of HBV dis-
ease in six different states of Northeastern India region
is shown in Table1. Different states have the distribu-
tion in different ranges and the numbers were showed
in the rst table. The number of Chronic cases is found
as the highest followed by Acute viral hepatitis, cirrho-
sis, HCC, and FHF. All the values were recorded and a
bar graph was plotted to express the distribution levels.
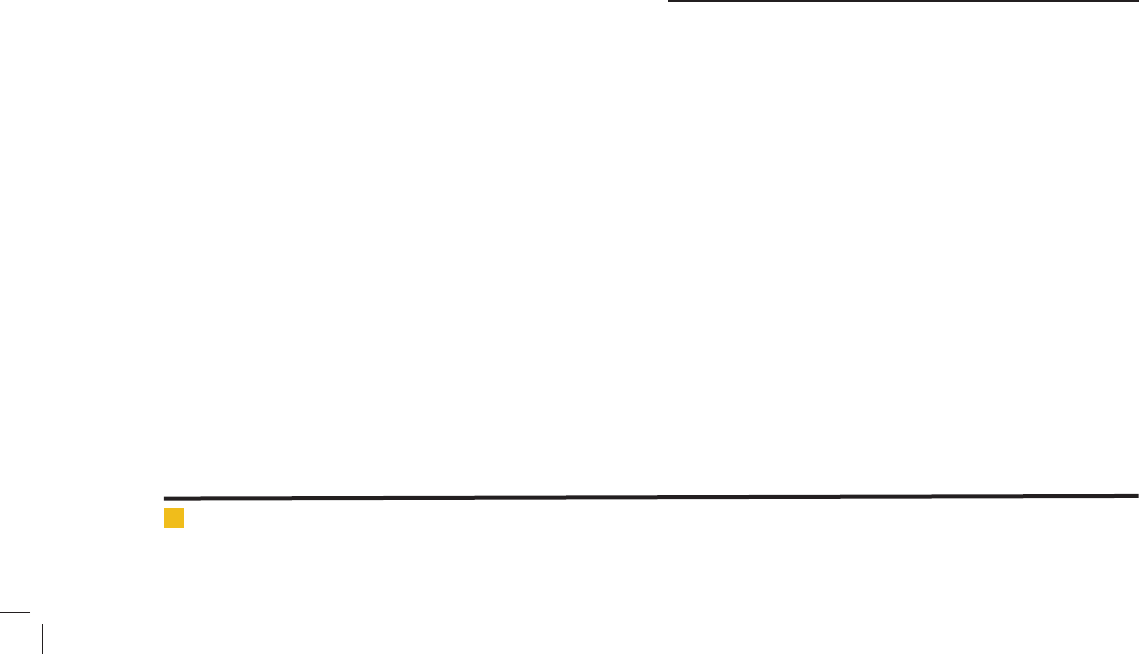
The mean and S.D values of age were also recorded and
it was distributed among all the groups of the disease
infected cases of Hepatitis B virus. The table 2 showed
all the mean and S.D values of the different stages of
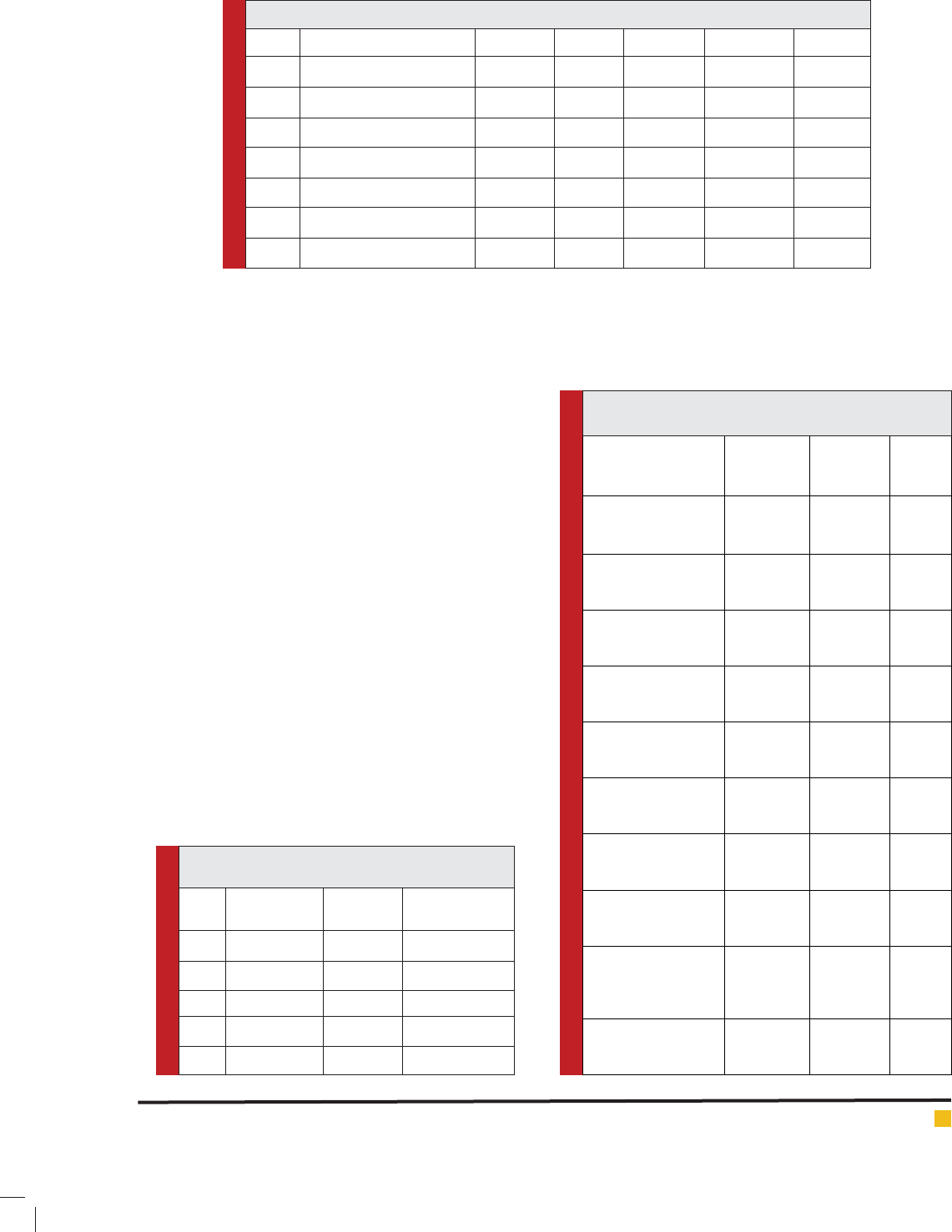
liver disease. The table 3 showed the risk factors of
HBV-related liver diseases were recorded and which
indicated the factors such as fever, anorexia, Abdomi-
nal discomfort,Haematemesis,weight loss, High coloured
urine, blood transfusion, alcoholic intake, multiple sex-
758 THE RISK FACTORS ASSOCIATED WITH HEPATITIS B VIRUS DISEASE BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
Namrata Kumari et al.
Table 1: Distribution of HBV infection among the different parts of North Eastern India.
S. NO STATES AVH FHF CAH CIRRHOSIS HCC
1 ASSAM (n=427,34.4%) 157 0 180 62 28
2 SIKKIM (n=260,20.9%) 151 2 48 54 5
3 MEGHALAYA (n=125,10%) 19 0 67 29 10
4 TRIPURA (n=186 ,14.98%) 32 2 105 33 14
5 ARUNACHAL (n=117 ,9.4%) 48 0 47 6 16
6 IMPHAL (n=126,10.1%)) 7 4 58 46 11
TOAL (n=1241) 414(33.3%) 8(0.64%) 505(40.7%) 230 (18.5%) 84 (6.76%)
Table2: The mean age of the study groups among
various categories of the HBV infection.
s. no Study group Number
(n=1241)
Mean Age±S.D
1 AVH 414 34.1 ± 4.33
2 CAH 505 40.1 ± 11.45
3 CIRRHOSIS 230 45.2 ±10.95
4 HCC 84 53.3 ± 9.57
5 FHF 8 35.3 ± 7.83
Table 3: The independent risk factors and their
signi cant role in the progression of the liver disease.
Risk Factors HBV DNA
PRESENT
(n=712)
HBV DNA
ABSENT
(n=571)
P value
Fever:
Present:
Absent :
206(29%)
506(71%)
204(36%)
367(64%)
0.01*
Anorexia:
Present
Absent
165(23%)
547(77%)
144(25%)
427(75%)
0.40
Abdominal Discomfort
Present
Absent
220(31%)
492(69%)
196(34.%)
375(66%)
0.4
Haematemesis:
Present
Absent
83(11%)
629(89%)
66(11%)
505(89%)
0.68
Weight Loss:
Present
Absent
216(30%)
488(70)
183(32%)
382(68%)
0.51
High coloured urine:
Present
Absent
76(11%)
636(89%)
90(16%)
481(84%)
0.003*
Blood Transfusion
Present
Absent
22(3%)
690(97%)
30(4%)
541(96%)
0.004*
Alcohol intake
Present
Absent
306(43%)
406(57%)
263(46%)
308(54%)
0.27
Multiple sexual
partners:
Present
Absent
37(5%)
665(95%)
25(4%)
546(96%)
0.049*
Ascites:
Present
Absent
130
581
95
476
0.44
ual partners, and ascites.In Northeast India HBV is a pre-
dominant underlying disease (52%).
In this report we showed that the CAH was distributed
the highest in number(n=505,40.7%)followedbyAVH(n=
414,33.3%),Cirrhosis(n=230,18.5%),HCC(n=84,6.76%)
and FHF(n=8,0.64%).So the number of FHF was the
least 0.64% among all. The highest number of infections
were recorded in Assam(n=427,34.3%) and the incident
rate of CAH was more and no FHF cases were recorded
during the study. In Sikkim 20.9% prevalence rate was
recorded and the incident rate of AVH(n=151)was the
highest followed by cirrhosis(n=54),CAH(n=48),HC
C(n=5)andFHF(n=2).10% of incident rates were recorded
in Meghalaya and the number of CAH(n=67) were more
than another group of the liver disease. In Tripura, the
HBV positive cases were recorded as 14.98%.Where CAH
was recorded as the highest (n=105) and only a few(n=2)
were recorded as FHF .9.4% of HBV were recorded in
Arunachal Pradesh with AVH(n=48)as the highest inci-
dent rates and no FHF cases were recorded. In Imphal,
only 10.1% cases of HBV were recorded and CAH was
the highest incident .
In the Table2, the mean Age±SD of HCC was was
recorded as 53.3 ± 9.57 which was greater than other
study groups of HBV. The infection with AVH was
recorded as 34.1 ± 4.33 .
The risk factors such as fever ,high coloured urine,
blood transfusion and Multiple sexual partners were
recorded as mostly signi cant(p<0.05).These risk fac-
tors are closely associated with the progression of the
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS THE RISK FACTORS ASSOCIATED WITH HEPATITIS B VIRUS DISEASE 759
Namrata Kumari et al.
FIGURE 1. The distribution of the HBV-related liver disease among all the states of NorthEastern India.
FIGURE 2. The distribution of different age groups as means±S.D in different cases of HBV.
FIGURE 3. The independent risk factors of HBV-related liver diseases in all the states by differentiating the
HBV DNA present or absent.
760 THE RISK FACTORS ASSOCIATED WITH HEPATITIS B VIRUS DISEASE BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
Namrata Kumari et al.
liver diseases than other recorded in this study. The other
risk factors were also recorded and the values were not
found as a highly associated but may be increased up
to a level.
In conclusion, it has been demonstrated that the
characteristic of Hepatitis B virus disease HBsAg surface
marker identi cation is the most important to nd the
prevalence rate of the liver disease. Along with the iden-
ti cation of marker, the risk factors are also necessary to
nd so that it may help the physicians to give the treat-
ment and also to reduce the high risk of this disease.So
the awareness should be made among the incident areas.
Finally, the signi cant distribution of major risk factors
raises the possibility of association of this HBV disease.
ACKNOWLEDGEMENT
A special acknowledgement goes to Indian Council
Medical Research,New Delhi for providing the funding
to carry out this study.
ABBREVIATIONS
• CHB, chronic hepatitis B
• HBsAg, hepatitis B surface antigen
• AVH,Acute viral Hepatitis
• HCC,Hepato cellular carcinoma
REFERENCES
Awole M, Gebre-Selassie S. Seroprevalence of HBsAg and its
risk factors among pregnant women in Jimma, Southwest
Ethiopia. Ethiop J Health Dev. 2005;19:45–50.
A. Wasley, D. Kruszon-Moran, W. Kuhnert, E.P. Simard, L.
Finelli, G. McQuillan, et al.The prevalence of Hepatitis B Virus
infection in the United States in the Era of Vaccination J Infect
Dis, 202 (2010),192–201.
Chaudhuri V, Tayal R, Nayak B, Acharya SK, Panda SK. 5.
Occult hepatitis B virus infection in chronic liver disease: full-
length genome and analysis of mutant surface promoter. Gas-
troenterology 2004; 127 : 1356-71.
Chen BF, Liu CJ, Jow GM, Chen PJ, Kao JH, Chen DS. High 8.
prevalence and mapping of pre-S deletion in hepatitis B virus
carriers with progressive liver diseases. Gastroenterology 2006;
130 : 1153-68.
Liang TJ. Hepatitis B: the virus and disease. 1. Hepatology
2009; 49 (Suppl 5): S13-21.
Kramvis A, Kew M, Francois G. Hepatitis B virus genotypes. 2.
Vaccine 2005; 23 : 2409-23.
Raimondo G, Allain JP, Brunetto MR, Buendia MA, Chen 3.
DS, Colombo M, et al. Statements from the Taormina expert
meeting on occult hepatitis B virus infection. J Hepatol 2008;
49 : 652-7.
Hollinger FB, Sood G. Occult hepatitis B virus infection: a 4.
covert operation. J Viral Hepat 2010; 17 : 1-15.
Mu SC, Lin YM, Jow GM, Chen BF. Occult hepatitis B 6. virus
infection in hepatitis B vaccinated children in Taiwan. J Hepa-
tol 2009; 50 : 264-72.
Fan YF, 7. Lu CC, Chen WC, Yao WJ, Wang HC, Chang TT, et
al. Prevalence and signi cance of hepatitis B virus (HBV) pre-S
mutants in serum and liver at different replicative stages of
chronic HBV infection. Hepatology 2001; 33 : 277-86.
Sengupta S, Rehman S, Durgapal H, Acharya SK, Panda SK.
9. Role of surface promoter mutations in hepatitis B surface
antigen production and secretion in occult hepatitis B virus
Infection. J Med Virol 2007; 79 : 220-8.
G.M. McQuillan, P.J. Coleman, D. Kruszon-Moran, L.A. Moyer,
S.B. Lambert, H.S. Margolis Prevalence of hepatitis B virus
infection in the United States: The National Health and Nutri-
tion Examination Surveys, 1976 through 1994 Am J Public
Health, 89 (1999), 14–18
Kim DH. Kang HS. Kim KH. Roles of hepatocyte nuclear factors
in hepatitis B virus infection.World J Gastroenterol. 2016 Aug
21;22(31):7017-29.
Metaferia Y. Dessie W. Ali I. Amsalu A. Seroprevalence and
associated risk factors of hepatitis B virus among pregnant
women in southern Ethiopia: a hospital-based cross-sectional
study. Epidemiol Health. 2016 Jun 19;38:27 .
Walle F, Asrat D, Alem A, Tadesse E, Desta K. Prevalence of
hepatitis B surface antigen among pregnant women attend-
ing antenatal care service at Debre-Tabor Hospital, Northwest
Ethiopia. Ethiop J Health Sci. 2008;17:13–20.
Ramos JM, Toro C, Reyes F,Amor A, Gutiérrez F.Seroprevalence
of HIV-1, HBV, HTLV-1 and Treponema pallidum among preg-
nant women in a rural hospital in Southern Ethiopia. J Clin
Virol. 2011;51:83–85.
Tegegne D,Desta K,Tegbaru B, Tilahun T. Seroprevalence and
transmission of hepatitis B virus among delivering women and
their new born in selected health facilities,Addis Ababa, Ethio-
pia: a cross sectional study.BMC Res Notes. 2014;7:239.
Zenebe Y, Mulu W, Yimer M, Abera B. Sero-prevalence and risk
factors of hepatitis B virus and human immunode ciency virus
infection among pregnant women in BahirDar city,Northwest
Ethiopia: a cross sectional study.BMC InfectDis. 2014;14:118.
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS THE RISK FACTORS ASSOCIATED WITH HEPATITIS B VIRUS DISEASE 761