
Health Science
Communication
Biosci. Biotech. Res. Comm. 9(4): 750-755 (2016)
Perceived stress and its relationship with spiritual
health in patients with diabetes in the city of
Urmia, Iran
Moradali Zareipour¹, Mehdi Abdolkarimi², Rohollah Valizadeh³, Hasan Mahmoodi
4
,
Zahra Khazir
5
, and Mousa Ghelichi Ghojogh
6
1
PhD student of HealthEducation andHealthPromotion, Health Center of Urmia, Urmia University, Urmia, Iran
2
PhD student of HealthEducation andHealthPromotion, Faculty of health, Shahid
SadoughiUniversityofMedical Sciences, Yazd, Iran
3
MSc student of Epidemiology, Student research committee, Urmia University of Medical Science, Urmia, Iran
4
PhD student of HealthEducation andHealthPromotion, Faculty of health, TabrizUniversityofMedical
Sciences, Tabriz, Iran
5
PhD student of HealthEducation andHealthPromotion, Faculty of health, Shahid
SadoughiUniversityofMedical Sciences, Yazd, Iran
6
Graduate of Epidemiology, Urmia University of Medical Science, Urmia, Iran. And Member of Young
Researchers Club and the elite Islamic Azad University Branch Zahedan, Iran
ABSTRACT
Psychological factors not only affect quality of life but also on the often determine the result of dealing with a
chronic illness can play an important role. According to the paradox results in the eld of the relationship between
mental health and spiritual health and limited studies about perceived stress and its relationship with spiritual health
of patients with diabetes, the aim of this study was to investigate the relationship between perceived stress and
spiritual health of patients with diabetes in the city of Urmia. This cross-sectional study (descriptive - analytical)
conducted with 330 patients with type 2 diabetes in rural health centers by random cluster sampling. Perceived Stress
and spiritual health questionnaire was used to collect information. Data using descriptive statistics and independ-
ent t-test, ANOVA and Pearson correlation coef cient were analyzed in SPSS v.21 software. The results of this study
showed that the majority of the patients’ perceived stress (70.9%) were in low level and the perceived stress mean of
them were in the low level (7.6±24.22) too. In terms of the level of the spiritual health, all patients were in medium
750
ARTICLE INFORMATION:
*Corresponding Author: mghelichi2000@yahoo.com
Received 23
rd
Sep, 2016
Accepted after revision 21
th
Dec, 2016
BBRC Print ISSN: 0974-6455
Online ISSN: 2321-4007
Thomson Reuters ISI ESC and Crossref Indexed Journal
NAAS Journal Score 2015: 3.48 Cosmos IF : 4.006
© A Society of Science and Nature Publication, 2016. All rights
reserved.
Online Contents Available at: http//www.bbrc.in/

Moradali Zareipour et al.
to high and mean score of spiritual health were in moderate level (95.6± 14.2) .There was statistically signi cant and
reverse relationship between perceived stress and spiritual health and its dimensions using Pearson correlation test
(p = 0.001, r =-0.48). According to the results of this present study, it is suggested to develop programs and approaches
to improve the spiritual health of patients with diabetes in order to improve their quality of life.
KEY WORDS: DIABETES, PERCEIVED STRESS, SPIRITUAL HEALTH
INTRODUCTION
According to the World Health Organization (WHO)
in 1947 Health is a state of complete physical, men-
tal and social well-being and not merely the absence
of disease or in rmity. (Butler, 1994) Mankind have
various dimensions such as cognitive, emotional,
social and spiritual, which lack of attention to each of
these dimensions leads to omission of important part
of human (Farahaninia, Abbasi, Givari, & Haghani,
2006). These dimensions interact with each other and
affect each other (Nejat, Montazeri, Holakouie Naieni,
Mohammad, & Majdzadeh, 2006). In most health mod-
els, spiritual health has been entered as one of the basic
dimensions (“Spiritual well-being.,”). Spiritual health is
an important dimension that strengthens the individual
adjustment and mental functioning and promotes other
dimensions of health (Mehrabiyan, 2016).
At the time of the occurrence of crises, spirituality is
a powerful resource that is a serious obstacle in front
of the psychological pressure and depression as well as
by encouraging individual to health behaviors, improves
overall health (“Promoting mental health.,”). Spiritual
health includes both religious and existence dimen-
sion, religious health is satisfaction caused by contact
with a superior power and existence health is trying to
understand the meaning and purpose of life. Chronic
and debilitating illnesses encounter person with ques-
tions about meaning and purpose of life (Jafari et al.,
2010).
Nowadays 347 million around the world are suffer-
ing from diabetes that 90% are type 2 (CORSER, 2010).
The prevalence of this disease in 1995, is estimated 4
% and it is anticipated to be 5.4% in the 2025 (Poro-
jan, Poanta, & Dumitrascu, 2012). According to World
Health Organization statistics, prevalence of diabetes
type 2 is 2% in Iran (World Health Organization-NCD
Country Pro les, 2011). On the other hand half of cases
of diabetes is unknown in the world and more than 5
million people in the world and 38 thousand die in Iran
are dying due to the complications of diabetes. Statistics
also show that the prevalence of diabetes is on the rise
in the world (Zimmet et al. 2014).
Psychological factor was considered as one of the
most important factors among more research in recent
years about the etiology, prognosis and treatment of
diabetes. One of the most important psychological fac-
tors affecting the occurrence of physical diseases such as
diabetes is stress, (Davadzah 2009). Psychological factors
not only affect quality of life but also often determine
the result of dealing with a chronic illness, especially in
diabetes care which is dependent on psycho-social fac-
tors to manage and achieve the proper control of this
disease (Kent et al., 2010).
Results of the study of Surwit and colleagues showed
that stress has a negative impact on health, particularly
in diabetics and can directly impair the control of dis-
ease by effect on diet, exercise and other self-learning
behaviors, so that life style and stress management is
accompanied with reduction in glycated hemoglobin
(glycosylated hemoglobin) (Surwit et al., 2002).
The results of another showed reverse signi cant
relationship between spiritual health and anxiety and
depression in cancer patients in the nal stages of life
(McCoubrie & Davies, 2006).The ndings of the study
of McMahon also showed the existence of a signi cant
relationship between spiritual health and anxiety in
cancer patients (McMahon, 2004). But con icting stud-
ies have also been reported for example a study in Eng-
land on about 250 patients showed that patients who
had much more powerful and higher status in terms of
spiritual beliefs within 9 months of continuous follow-
up after discharge from the heart and women, had worse
prognosis and status than other patients (Beery et al.
2002).
Therefore, despite the paradox results in the eld
of the relationship between mental health or spiritual
health in the absence of a study on perceived stress and
its relation with the spiritual health in patients with dia-
betes, it seems to be important the identi cation of the
relationship between these two variables and should be
considered by care providers, policy makers, planners
and economists of our health system.In addition to the
comments raised about the spiritual health, it can be
related as a motivational factor on the adoption of effec-
tive health. The relationship between health behaviors
including control of stress with spiritual health can lead
to a more desirable quality of life in the elderly that
have a lot worth and more priority in clinical decisions
and health policies. This study aimed to examine the
perceived stress and its relationship with spiritual health
in patients with diabetes in the city of Urmia.
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS PERCEIVED STRESS IN DIABETIC PATIENTS 751

Moradali Zareipour et al.
MATERIAL AND METHODS
This study was a cross-sectional study (descriptive – ana-
lytic) that 330 patients with type 2 diabetic of 10 rural
health centers were selected by cluster random sampling
method. Then, they were invited to interview and com-
plete a questionnaire. Before conducting research were
given enough explanation about subjects of study and
attracted their interest to participate in the study. After
signing a written consent of the research, questionnaires
completed using self-reporting method and questioner’s
guide, in the case of illiterate people questionnaires were
completed by health workers and through interview.
Questions related to demographic and blood sugar
and body mass index were registered from the les
of the patient by health workers. Questionnaires were
completed in a step using self-reporting method. The
information collection tool in this study, apart from
demographic (age, sex, education level, economic sta-
tus, occupation, duration of diabetes, type of treatment
and smoking) and disease including two questionnaires
the perceived stress questionnaire and spiritual health
questionnaire.
Perceived stress was measured by questionnaire pro-
vided by Cohen et al in 1983. This tool is very suitable
to determine the level of recognition of your stress in
front of unpredictable and uncontrollable events of life
including 14 questions from 0 to 4 with Likert scale that
answers are classi ed as 0 (never), 1 (rarely), 2 (some-
times), 3 (more times) and 4 (all the time).
It should be noted in the case of positive questions
(4.5.6.7.9.10.13), scoring can be calculated reversely. In
total, the scope of scores is considered 0-56. Scores less
than 28 were included in the low perceived stress group
and equal or higher than 28 in the high perceived stress
group (17). As well as the spiritual health variable using
the scale of spiritual well-being provided by Ellison and
Paloutezain in 1983, was measured that includes 20 Lik-
ert 6 pointed questions from completely agree (score 6)
to completely disagree (score 1).
It is worth noting that scoring was reverse in the
phrase with the negative verb forms. This scale is
divided into two subscale, existence health and religious
health, which each one included 10 phrase and 10 to
60 score. The total score is the sum of these two groups
20 to 120 that is a form of low spiritual health (20-40),
medium (41-99) and high (100-120) (Wang, Snyder, &
Kaas, 2001).
In this study, the Cronbach’s Alpha for the perceived
stress questionnaire obtained 0.88 and for the spiritual
health obtained 0.80. Data analyzed using the SPSS v.
21. Biographical information and diseases using descrip-
tive statistics methods were evaluated. As well as analy-
sis of variance and the t-test and Pearson correlation
coef cient were used for the purpose of analysis (signi -
cance level p < 0.05).
RESULTS AND DISCUSSION
The results of this study showed that 69.1% and 30.9
were participated male and female, respectively and the
mean age, BMI, FBS and HbA1C of patients were 60.4
± 73.08, 28.4±5.7, 158.7±140 and 7.86±1.8, respec-
tively. The majority of patients in terms of the education
were illiterate (52.1%) and elementary (39.4 %), 66.1 %
housewives, 63.9 % with moderate economic status and
77.2% with overweight and obesity. Duration of diabe-
tes in the majority of patients (89.4%) was less than 10
years (table 1).
The majority of patients (70.9%) have reported their
perceived stress in low level and the mean perceived
stress in them was low (24.22 ±7.6) (table 2). As well
as the results of the study showed that there was a sig-
ni cant relationship (p = 0/003) between the perceived
stress of patients and the sex variable that the mean
perceived stress scores of females was higher than males.
The results showed that there was a signi cant relation-
ship (p = 0/005) between the perceived stress of patients
and the occupation variable so that the mean per-
ceived stress in housewife group was higher than other
groups.
On the other hand in the group of patients that the
duration of the disease was more than 10 years, the
mean score of perceived stress was higher than other
groups and there was a signi cant statistically differ-
ence between the mean scores of perceived stress and
duration of diabetes (p = 0.008). In the case of other
individual variables and disease, the results suggest that
there were no signi cant statistically relationship among
the mean scores of perceived stress and complications
arising from the disease (p = 0.841), smoking (p = 0.523),
level of education (p = 0.075) and marital status (p =
0.111) while there was a signi cant statistically relation-
ship between mean perceived stress and economic status
(p = 0/001) and type of treatment (p = 0.028).
In terms of the level of the spiritual health, all patients
were moderate to high and spiritual health score was in
moderate level (table 2). As well as there were a statisti-
cal signi cantly relationship among spiritual health and
variables in terms of sex (p = 0.045), duration of disease
(p = 0.008), type of treatment (p = 0.028), economic sta-
tus (p = 0.001) and occupation (p = 0.005) while this
relationship was not observed among spiritual health
and complications of disease (p = 0.122), smoking (p =
0.611), marital status (p = 0.111) and the level of educa-
tion (p = 0.075). According to Pearson correlation test,
there was a signi cant and reverse relationship between
752 PERCEIVED STRESS IN DIABETIC PATIENTS BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
Moradali Zareipour et al.
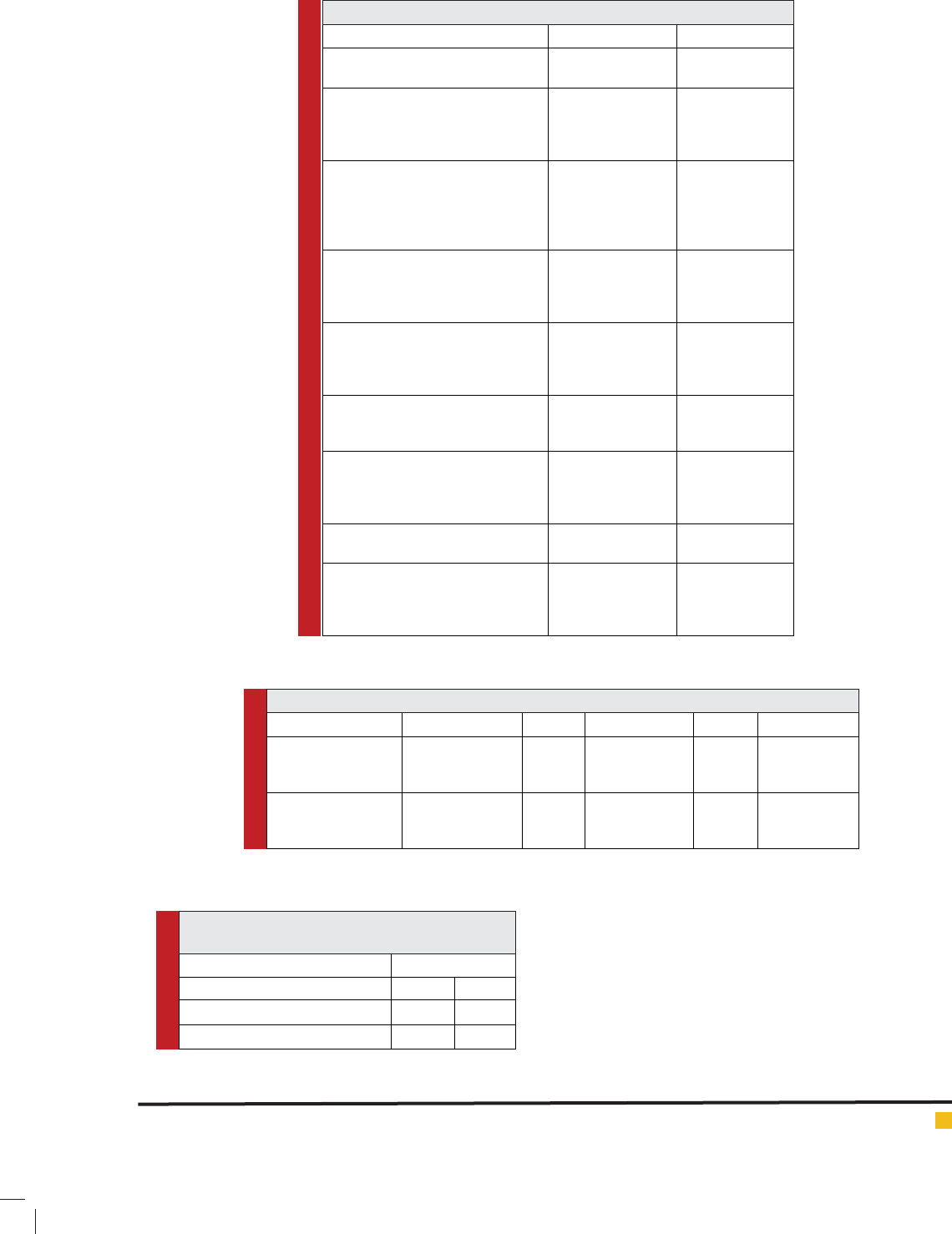
Table 1: Demographic and disease information of diabetic patients
Variable levels Frequency (%)
Sex Male
Female
(30.9)102
(69.1)228
Education level Illiterate
Elementary Diploma
Collegiate
1/52)172
(4/39)130
(6/7)25
( (9/0)3
Occupation rancher
self-employed
employee
housekeeper
others
(2/18)60
(10)33
(5/1)5
(1/66)218
(3/4)14
Marital status Single
Married
Divorced
Widow
(1/2)7
(9/83)277
(3/0)1
(6/13)45
Duration of diagnosed diabetes (year) Less than 2
5-2
9-6
More than 10
(17)56
(1/49)162
(3/23)77
(6/10)35
Economic status Low
Moderate
Good
(7/19)65
(9/63)211
(4/16)54
Treatment type Insulin
Pill
Food
Food and Pill
(2/11)37
(2/74)245
(3/7)24
(3/7)24
Smoking Yes
No
(9/10)36
(8/88)293
BMI Less than 18.5
24.9-18.5
29.9-25
More than 30
(5/1)5
(2/21)70
(8/44)148
(4/32)107
Table 2: Frequency distribution of Spiritual health and perceived stress in diabetic patients
Factor level Range SD± Mean % Frequency
Perceived stress <28
28≤
Total
55-6 7.6±24.22
70.9
29.1
100
234
96
330
Spiritual health Moderate (99-41)
High (120-100)
Total
119-57 14.2±95.6 46.1
53.9
100
152
178
300
Table 3: Correlation between spiritual health and
perceived stress in patients with diabetes
Spiritual health dimensions Blood sugar
Existence health p=0/31 r=-0/07
Religious health p=0/35 r=-0/06
Spiritual health(Total) p=0/27 r=-0/07
perceived stress and its dimensions (religious and exist-
ence health) (table 3).
The results of this study showed that 70.9 % of the
patients had low perceived stress that implies symptoms
of mental health in patients with diabetes and only 29.1
%reported high perceived stress that based on the study
of wang and colleagues can be associated with problems
and the complexity of the issues related to the physical
condition of the patients and familial problems (Wang
et al., 2001).
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS PERCEIVED STRESS IN DIABETIC PATIENTS 753
Moradali Zareipour et al.
Unlike the study of Bastani (1) and Malek (Malek,
Poorafkary, Dadashzadeh, & Safaeeyan, 2008), there
was no signi cant relationship between perceived stress
and age in this study. There was a signi cant relation-
ship between the status of occupation and perceived
stress, as in housewife group perceived stress was higher
than employed group that is consistent with the study
of Shoja and colleagues. Considering that people with
speci c occupation involved in a string of job activities
and are associated with participation in different social
environments and various people more than those who
have not job. Occupation can affect their mental health
(SHOJA, 2013).
In this study, despite the lack of a meaningful rela-
tionship between education level and perceived stress,
mean perceived stress scores on patients with college
education was less than patients who had not diploma.
It represent that education can reduce perceived stress
and anxiety of people in personal affairs and social role
and nally mental health by increasing the con dence,
as well as an increase in social communication. On the
other hand social and cultural limitations and as well as
the inability of individuals to use effective ways to deal
with stress factors in people with a lower education level,
can be main reason of the high stress that these results
are consistent with the results of other study (Bastani
et al. 2005; Habibi et al 2008; Harpham et al.2004) on
the other hand, in this study the mean perceived stress
scores in patients who have had speci c diet was sig-
ni cantly high compared with patients who have had
insulin and pills diet that it’s reason can be dif culty of
compliance of speci c diet and fear and stress resulting
from adherence to the diet.
Based on the results of this study, 53.9 % of patients
have reported their spiritual health in high levels, while
in the study of Bastani et al (2005) 43.9% of patients had
moderate spiritual health (Bastani et al., 2005). In this
study, similar to the results of Jadidi study (Jadidi, Fara-
haninia, Janmohammadi, & Haghani, 2011), there was
no a signi cant relationship between spiritual health
and age of the patients, while in other studies (Bastani
et al., 2005; Zarei et al. 2015) a signi cant and direct
relationship between spiritual health and age of the
patients were reported, so that whatever the age of the
patients is increased, the tendency towards spirituality
will be more. In our study, unlike the results of the study
of Bastani (Bastani et al., 2005), there was a signi cant
relationship between spiritual health and sex of patients.
There was a reverse relationship between perceived
stress and spiritual health dimensions in this study. In
other words, patients who had higher perceived stress,
had lower spiritual health and conversely patients who
had lower perceived stress, had higher spiritual health.
These results were consistent with the results of McCou-
brie & Davies, (2006). While Beery et al., (2002) showed
that patients who had higher and powerful status in
terms of spiritual beliefs, had worse prognosis than other
patients within 9 months of continuous follow-up after
discharge from the heart and women wards
CONCLUSION
Based on the ndings of this study, perceived stress were
low in the patients with diabetes mellitus with higher
scores of spiritual health. So it is necessary to be paid
attention to the psychological and spiritual dimensions
of health in patients with diabetes in order to improve
the quality of care. It can be used in accordance with
the results of this study the importance of paying atten-
tion to the spiritual beliefs in life to deal with prob-
lems arising from chronic diseases. Care is beyond cure
and attention to the various dimensions of the human
being in the care of chronic disease seems quite impor-
tant. The dominant religious culture in Iranian society is
also facilitator to achieve the comprehensive approach
to care. According to the results of the present study,
it is suggested to compile programs and approaches in
order to promote the spiritual health and quality of life
in patients with diabetes.
REFERENCES
Bastani, F., Hidarnia, A., Kazemnejad, A., Vafaei, M., & Kasha-
nian, M. (2005). A randomized controlled trial of the effects of
applied relaxation training on reducing anxiety and perceived
stress in pregnant women. Journal of Midwifery & Women’s
Health, 50(4), e36-e40.
Beery, T. A., Baas, L. S., Fowler, C., & Allen, G. (2002). Spiritu-
ality in persons with heart failure. Journal of Holistic Nursing,
20(1), 5-25.
Butler, J. T. (1994). Principles of health education and health
promotion: Morton Publishing Company.
Corser, W., Lein, C., Holmes-Rovner, M. & Gossain, V. . (2010).
Contemporary adult diabetes mellitus management percep-
tions. The Patient: Patient-Centered Outcomes Research(3),
101-111.
Davazdah Emamy, M., Roshan, R., Mehrabi, A. & Attari, A.
(2009). The effectiveness of cognitive-behavioral stress man-
agement training on glycemic control and depression in
patients with type 2 diabetes. . Iranian Journal of Endocrinol-
ogy and Metabolism(11), 385-392.
Farahaninia, M., Abbasi, M., Givari, A., & Haghani, H. (2006).
Nursing students’ spiritual well-being and their perspectives
towards spirituality and spiritual care perspectives. Iran Jour-
nal of Nursing, 18(44), 7-14.
Habibi, A., Neekpoor, S., Seyedolshohda, M., & Haghani, H.
(2008). Health promotion behaviours and Quality of life among
elderly people: A crosssectional survey 2006. Journal of Arda-
bil University of Medical Sciences, 8(1), 29-36.
754 PERCEIVED STRESS IN DIABETIC PATIENTS BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS

Moradali Zareipour et al.
Harpham, T., Grant, E., & Rodriguez, C. (2004). Mental health
and social capital in Cali, Colombia. Social science & medicine,
58(11), 2267-2277.
Jadidi, A., Farahaninia, M., Janmohammadi, S., & Haghani,
H. (2011). The relationship between spiritual well-being and
quality of life among elderly people residing in Kahrizak senior
house. Iran Journal of Nursing, 24(72), 48-56.
Jafari, E., Naja , M., Sohrabi, F., Dehshiri, G. R., Soleymani, E.,
& Heshmati, R. (2010). Life satisfaction, spirituality well-being
and hope in cancer patients. Procedia-Social and Behavioral
Sciences, 5, 1362-1366.
Kent, D., Haas, L., Randal, D., Lin, E., Thorpe, C. T., Boren, S.
Nelson, J. (2010). Healthy coping: issues and implications in
diabetes education and care. Population health management,
13(5), 227-233.
Malek, A., Poorafkary, N., Dadashzadeh, H., & Safaeeyan, A.
(2008). Ranking of stressful life events in general population
of Tabriz, Iran. Research Journal of Biological Sciences, 3(9),
993-998.
McCoubrie, R. C., & Davies, A. N. (2006). Is there a correlation
between spirituality and anxiety and depression in patients
with advanced cancer? Supportive Care in Cancer, 14(4), 379-
385.
McMahon, R. L. (2004). The Impact of Spirituality, Social Sup-
port, and Defensive/adaptive Coping on Death Anxiety at End
of Life.
Mehrabiyan, T. (2016). The Relationship of Prayer and Spiritual
Health with Self-Esteem of Patients Treated with Hemodialysis
in Ilam. Military Caring Sciences, 2(4), 214-220.
Nejat, S., Montazeri, A., Holakouie Naieni, K., Mohammad, K.,
& Majdzadeh, S. (2006). The World Health Organization quality
of Life (WHOQOL-BREF) questionnaire: Translation and vali-
dation study of the Iranian version. Journal of School of Public
Health and Institute of Public Health Research, 4(4), 1-12.
Porojan, M., Poanta, L., & Dumitrascu, D. (2012). Assessing
health related quality of life in diabetic patients. Rom J Intern
Med, 50(1), 27-31.
Promoting mental health. Available from:URL:www.who.int/
mental_health/evidence/MH_Promotion_Book.pdf.
Shoja, M., Rimaz, S., Asadi, L. M., Bagheri, Y. S. A. & Gohari,
M. R. . (2013). Mental Health of Older People and Social
Capital. Journal of the Iranian Institute for Health Sciences
Research(12), 345-353.
Spiritual well-being. Available from:URL:http://academic.
cuesta.edu/wholehealth/level2/lecpages/sp03.htm.
Surwit, R. S., Van Tilburg, M. A., Zucker, N., McCaskill, C. C.,
Parekh, P., Feinglos, M. Lane, J. D. (2002). Stress management
improves long-term glycemic control in type 2 diabetes. Dia-
betes care, 25(1), 30-34.
Wang, J.-J., Snyder, M., & Kaas, M. (2001). Stress, loneliness,
and depression in Taiwanese rural community-dwelling elders.
International Journal of Nursing Studies, 38(3), 339-347.
World Health Organization-NCD Country Pro les. (2011).
Available from:URL: http://www.who.int/nmh/countries/iran_
en.pdf.
Zarei, B., Vagharseyyedin, S. A., & Gorganie, E. (2015). Rela-
tionship Between Spiritual Well-Being and Self-Management
Among Iranian People With Multiple Sclerosis. Jundishapur
Journal of Chronic Disease Care, 4(4).
Zimmet, P. Z., Magliano, D. J., Herman, W. H., & Shaw, J. E.
(2014). Diabetes: a 21st century challenge. The Lancet Diabetes
& endocrinology, 2(1), 56-64.
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS PERCEIVED STRESS IN DIABETIC PATIENTS 755