
Biomedical
Communication
Biosci. Biotech. Res. Comm. 9(4): 689-693 (2016)
Effectiveness of constrained time of visual data on
angular velocity during sit-to-stand movement
in three planes
Mozhgan Faraji Aylar*, Faramarz Firouzi and Mandana Rahnama Araghi
Faculty of Engineering, Electrical Engineering Department, Imam Reza International University,
Mashhad, Iran
Faculty of engineering, Department of Biomedical Engineering, Mashhad Branch, Islamic
Azad University, Iran
Faculty of Physical Education & Sport Sciences, Ferdowsi University of Mashhad, Iran
ABSTRACT
The purpose of this study investigation was to assess whether time of constrain of visual information in uences the
angular velocities of sit to stand (STS) task in children or not. Five girls with congenital blindness (CB) and ten girls
with no visual impairments were divided into two groups of ve, control or treatment. The participants in the treat-
ment group were asked to close their eyes (EC) for 20 minutes before the STS test; whereas the ones in the control
group kept their eyes open (EO). The performance of the participants in all three groups was measured using a motion
capture system and two force plates. The results showed that the constrained duration of visual information did not
affect the angular velocities of lower extremity joints in three planes (sagittal, frontal and transverse). These nding
suggest that vision is not the major in uence factor on the STS kinematics.
KEY WORDS: VISUAL INFORMATION, SIT TO STAND, ANGULAR VELOCITIES, ANATOMICAL PLANES
689
ARTICLE INFORMATION:
*Corresponding Author: m.faraji@imamreza.ac.ir
Received 26
th
Oct, 2016
Accepted after revision 2
nd
Dec, 2016
BBRC Print ISSN: 0974-6455
Online ISSN: 2321-4007
Thomson Reuters ISI ESC and Crossref Indexed Journal
NAAS Journal Score 2015: 3.48 Cosmos IF : 4.006
© A Society of Science and Nature Publication, 2016. All rights
reserved.
Online Contents Available at: http//www.bbrc.in/
INTRODUCTION
Sit-to-stand (STS) motion is a demanding activity of
everyday living that is on average performed four times
in an hour (Coghlin & McFadyen, 1994; Music, Kamnik,
& Munih, 2008), and is accepted as being a prerequisite
for gait (Kerr, White, Barr, & Mollan, 1997). Some stud-
ies demonstrated that the hip and knee joints required
highly forces during STS performance greater than gait
and stair ascent (Kerr et al 1994).
Dark adaptation for the visual system is the pro-
cess of adjusting to total darkness or to lower levels
690 EFFECTIVENESS OF CONSTRAINED TIME OF VISUAL DATA ON ANGULAR VELOCITY BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
Mozhgan, Faramarz and Mandana
of illumination (Held, 1988). The time of the rod inter-
cept reported is less than or equal to 20 min, usually
8.2 (±1.4) min (Jackson & Edwards, 2008)
and 12.5 min
(Holfort et al 2010), in young and elderly people, respec-
tively. Therefore, in this study, the time of the eyes being
closed was set to be 20 minutes to ensure occurrence of
rod intercept.
Congenitally blind children usually suffer from falls
that result in injury (Jackson, et al 1999) and contusion.
The STS movement is one of the safest tasks for blind
children to perform. The STS movement requires the
coordination of all body segments (Manckoundia et al.
2006) and balance (Treasurer et al 2007). The STS task is
a common activity in daily life (Galli et al 2008), so it is
completely familiar with central nervous system (CNS).
In addition, the study of visual adaptation is important
for a variety of practical reasons as well as for obtaining
an understanding of the effects of the visual information
in performance of the motor tasks. The speci c objective
of the present study was to characterize the kinematics
of STS performance in short- and long-durations dark
adaptation tasks. The fundamental aim of this study was
to develop knowledge about the visual memory during
the STS performance.
METHODS
PARTICIPANTS
The total participants in this study were 15 girls who
were randomly selected. Five of the girls suffered from
congenital blindness (CB) (mean (±standard deviation),
age: 94.6 (±5.58) mo, mass: 25.74 (±2.12) kg, height:
126.82 (±0.05) cm, leg length: 36.62 (±1.58) cm, anterior
superior iliac spines (ASIS) width: 17.76 (±1.23) cm) and
the remaining ten were healthy and did not have any
visual impairments. These ten healthy girls were divided
into two groups.
The subjects in one group (treatment group) closed
their eyes (EC) (age: 93.8 (±5.88) mo, mass: 24.16 (±1.36)
kg, height: 124.24 (±0.044) cm, leg length: 34.56 (±1.13)
cm, ASIS width: 15.84 (±0.64) cm) for 20 minutes
before the STS test was carried out ; whereas the other
group (control group) kept their eyes open (EO) (age:
95.8 (±5.53) mo, mass: 26.06 (±5.21) kg, height: 126.66
(±0.05) cm, leg length: 36.16 (±1.56) cm, ASIS width:
16.46 (±0.95) cm). During the practice and trial phases,
the subjects in the EC group had their eyes closed to pre-
vent any learning taking place through receiving visual
information. The healthy girls had no musculoskeletal or
neuromuscular problems and were considered normally
active. Moreover, blind children were physically active
in daily life and merely suffered from blindness. An
informed oral consent was obtained from each subject
and their parents after they were provided with detailed
information about the study. In addition, a local ethic
committee con rmed the human studies.
DATA COLLECTION
Retro-re ective markers were placed over bony land-
marks including: vertex, seventh cervical vertebra (C7),
spinous process of the twelfth thoracic vertebrae, right
and left of lateral border of the acromion process, right
and left of head of humer us, right and left of olecranon
process of the ulna, right and left of head of styloid pro-
cess of the ulna, right and left of ASIS, right and left of
posterior superior iliac spines (PSIS), right and left of
greater trochanter, right and left of lateral femoral epi-
condyles, right and left of lateral malleoli, right and left
of 5th distal metatarsal heads, right and left of calcaneal
tuberosity.
Before performing the test, the equipment and the
instruments were introduced verbally to the participants
in the EO group; whereas this was done through sense of
touch for the EC and CB groups. The Subjects were bare-
foot and were seated on a rm chair with no armrest, back
support or wheels. The height of the chairs was adjusted
in a way that corresponded with 100% of the subject’s leg
length, the distance from the lateral femoral condyle to
the ground. During the STS test, the participants had one
foot on each force plate for 3 to 4 s (Kerr, et al. 1994), the
arms were folded across the chest and wore tight shorts.
The subjects sat with their bodies and extremities
(thighs, legs and feet) symmetrically placed relative to
the chair and the width of the feet was determined from
the ASIS width. The subjects in EO group were told to
place their feet within the outer limits of the two force
plates, one foot on each plate. In addition, the subjects
were requested to use a self-selected movement strategy.
The widths of the ASIS for the EC and CB groups were
determined using a thick stick on the force plates. They
were instructed to raise their entire body from the chair at
a self-selected velocity, and keep standing until reaching
the upright position for 3 to 4 s ( Kerr et al., 1994). Each
subject was requested to perform ve STS trials with 30 s
rests between the trials and had three practices before the
actual test. Lower limb dominance was determined by the
foot used to kick a ball (Burnett et al. 2011).
Two adjusted force plates (9260AA6, Kistler, Switzer-
land) with a sampling frequency of 1000 Hz, were used
to record the ground reaction forces during the perfor-
mance of the STS task. An eight camera video-based
opto-electronic system (Qualisys AB, Sweden, sampling,
100 Hz) was used for 3D motion capture. The Force plates
and the motion data were ltered using a fourth order
Butterworth lter (cutoff frequency of 10 Hz) ( Huffman
et al 2015).
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS EFFECTIVENESS OF CONSTRAINED TIME OF VISUAL DATA ON ANGULAR VELOCITY 691
Mozhgan, Faramarz and Mandana
DATA PROCESSING
Upper extremity markers were used to de ne STS events.
Markers of olecranon process of the ulna and head of
styloid process of the ulna were used to control folded
arms across the chest because all participants were chil-
dren in the investigation. Markers of ASIS, PSIS and
greater trochanter were used to de ne hip joint center.
Segment of head-arm-trunk (HAT), thigh, leg and foot
were de ned by the head of humerus to the hip center,
the hip center to the lateral femoral epicondyle, the lat-
eral femoral epicondyle to the lateral malleoli, the lateral
malleoli to the 5th distal metatarsal heads, respectively.
Flexion, abduction, and internal rotation occurred at
the initiation of movement, when STS entered its nal
points, was beginning extension, adduction, and exter-
nal rotation at sagittal, frontal, and transverse planes,
respectively.
STATISTICAL ANALYSIS
Descriptive values (means, standard deviations) across
trials were rst obtained. Data distribution was tested
for homoscedasticity using the Levene’s test. A one-way
repeated measures analysis of variance (ANOVA) was
performed to test for the effects of vision on angular
velocities of the lower extremity joints (the hip, knee
and ankle). A two-way repeated measure ANOVA was
performed to test the effects of interaction of a visual-
motor adaptation memory and phases of STS motion on
(1) phase durations and (2) differences between phase
durations. If equal variance was found between groups,
Bonferroni’s post hoc test was used for pair-wise com-
parison of means. If unequal variance was determined
between groups, Tamhane’s was used for pair-wise com-
parison (Highsmith et al., 2011). These analyses were
performed separately for dominant and non-dominant
sides. Differences were considered signi cant at p <
0.05. Statistical analysis was performed using the SPSS
19.0
®
software.
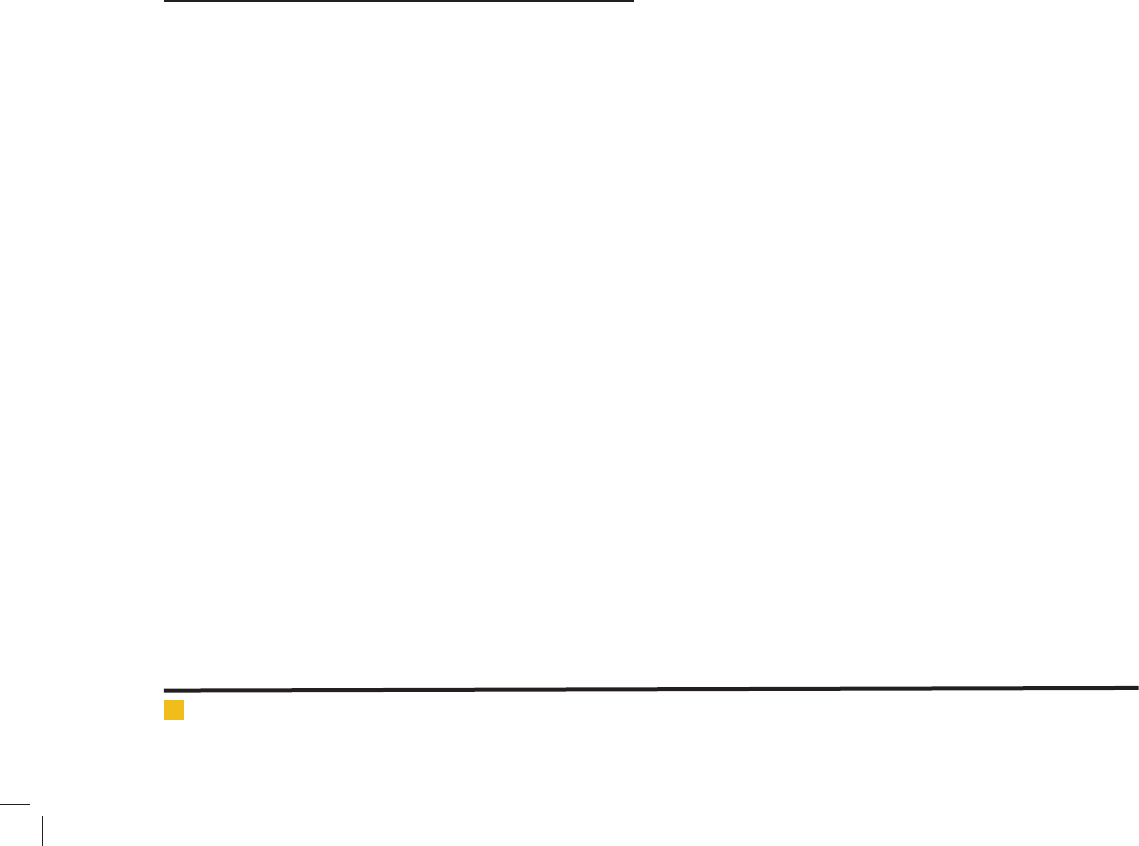
RESULTS
The CB group had the lowest value and the EC group got
the highest value among the groups during the prepara-
tion phase. Also, the EO group had the lowest value and
the EC group got the highest value among the groups
during the standing phase and total duration of the STS
performance (Table 1).
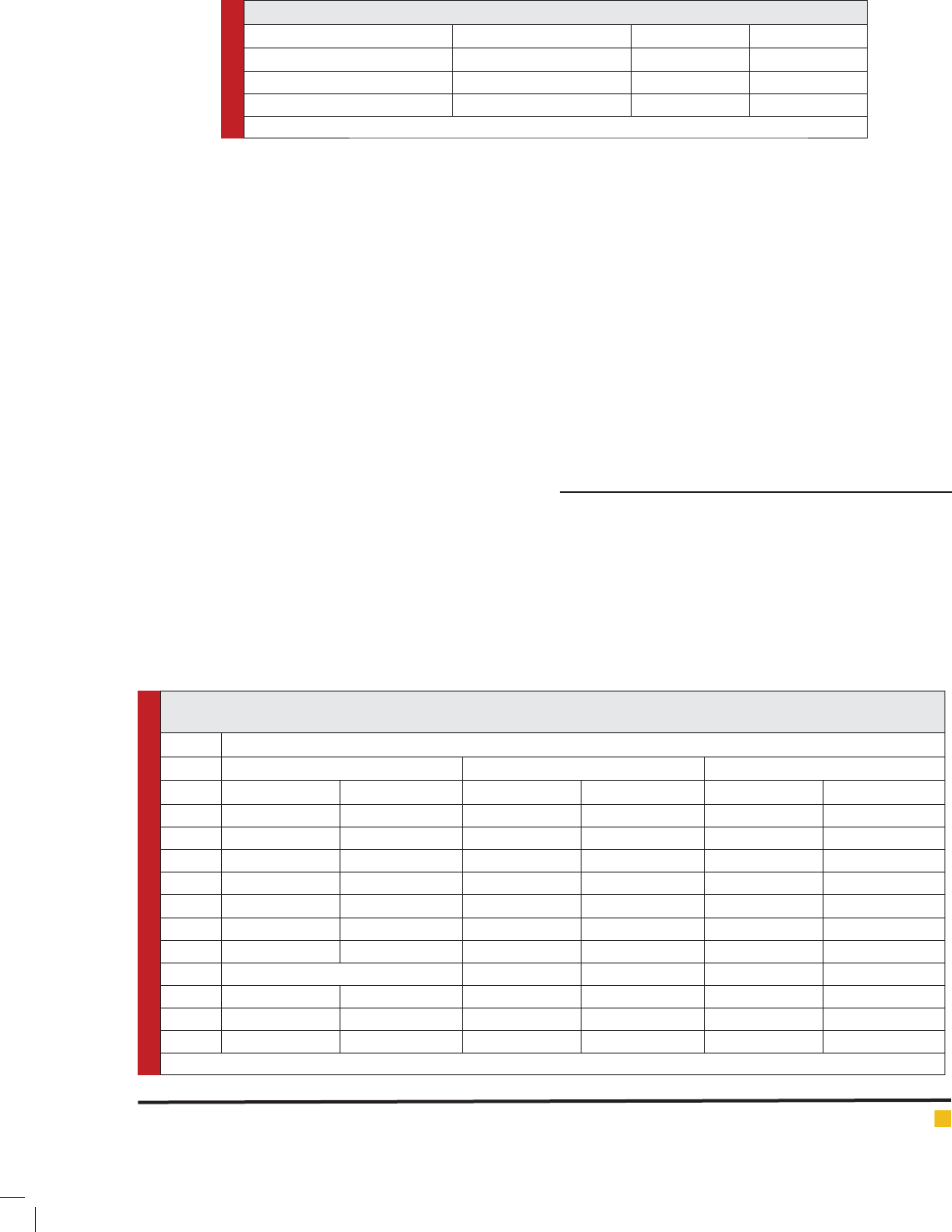
On both sides (D and ND) in the sagittal plane, the
EO group at the ankle joint had the lowest value and
Table 1: Phase durations of sit-to-stand (STS) motion
Congenital blindness Eyes closed Eyes open
Phase I (preparation phase) 0.48 ± 0.30 0.614 ± 0.36 0.492 ± 0.09
Phase II (rising phase) 0.888 ± 0.53 1.22 ± 0.55 0.568 ± 0.12
Total duration of STS motion 1.308 ± 0.51 1.834 ± 0.39 1.06 ± 0.13
Values are in second: mean ± SD.
Table 2: Means for ankle, knee, and hip angular velocity for congenital blindness, eyes closed, and eyes open groups at
dominant and non-dominant sides during sit-to-stand in sagittal, frontal, and transverse planes.
Sagittal plane
Eyes openEyes closedCongenital blindness
Non-DominantDominantNon-DominantDominantNon-DominantDominant
1.24 ± 7.382.58 ± 4.015.53 ± 3.517.35 ± 5.7710.72 ± 6.947.02 ± 3.71Ankle
58.56 ± 14.8158.43 ± 9.7141.08 ± 11.1943.63 ± 14.0560.39 ± 26.2259.49 ± 24.04Knee
56.06 ± 7.0057.48 ± 7.5134.60 ± 6.4336.50 ± 9.4652.26 ± 24.2754.35 ± 24.96Hip
Frontal plane
-4.19 ± 7.2810.84 ± 7.774.35 ± 5.407.76 ± 6.929.62 ± 13.988.77 ± 6.38Ankle
12.57 ± 12.3211.87 ± 12.0110.96 ± 6.5810.81 ± 6.895.91 ± 7.4820.23 ± 10.13Knee
12.58 ± 12.187.94 ± 6.805.32 ± 8.29-.72 ± 17.406.79 ± 3.8511.13 ± 7.27Hip
Transverse plane
-14.62 ± 45.717.15 ± 17.5817.35 ± 13.058.37 ± 13.1621.73 ± 34.2825.21 ± 17.92Ankle
-21. 01 ± 51.32-7.66 ± 8.3124.95 ± 32.8049.11 ± 44.4124.53 ± 38.778.74 ± 13.56Knee
-29. 10 ± 22.48-.25 ± 24.38-.32 ± 10.5614.36 ± 30.4816.17 ± 39.44-12.54 ± 11.90Hip
Values are in degree/second: mean ± SD.
692 EFFECTIVENESS OF CONSTRAINED TIME OF VISUAL DATA ON ANGULAR VELOCITY BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
Mozhgan, Faramarz and Mandana
at the hip joint reached the highest value among the
groups. In addition, the EC group at the knee and hip
joints obtained the lowest value among the groups. Fur-
thermore, the CB group got the highest angular velocity
among the groups in both sides of the lower extrem-
ity except at the D side of the ankle joint. In frontal
plane, the EC group at the hip joints reached the lowest
value among the groups. In vertical plan, the EO group
at the ankle and the knee joints obtained the lowest
value and the CB group had the highest value among
the groups (Table 2). However, no signi cant difference
was observed among the groups at three plans.
DISCUSSION
The fundamental aim of this study was to investi-
gate how short (EC group) and long (CB group) terms
restricted visual memory affect the angular velocities of
the lower extremity joints during the STS movements.
The results of this study were consistent with those of
some previously conducted studies (Hennington et al.,
2004; Santos et al. 2013; Yasin et al. 2008). In this study,
the longest time of STS performance was dedicated to
standing phase among the all participants (Table 1).
The EC group had the highest time of the STS move-
ment. This result exhibits that blind people hurry to rise
from chair (i.e. seat-off point), although they had a little
patience in the standing phase.
Hennington and others have reported at 0.583 (±0.117),
0.661 (±0.288), and 1.242 (±0.117) seconds for before
seat-off, after seat-off and total duration of STS motion,
respectively between 4.3 to 11.8 years old. In the present
study, the duration of preparation phase was 0.48(±.30),
0.614(±.36), and 0.492(±.09) seconds for the CB, EC and
EO groups, respectively (Hennington et al., 2004). In the
preparation phase, the present study was similar to the
result of Hennington’s study, but for the EC group a little
difference has been observed in the standing phase and
the total duration of the STS movement.
In Seven’s study, total duration of STS motion was
reported at 1.34 (±0.31) for 9.6 (±1.2) years old, our nd-
ing in the EC group was slightly different from the value
(Yasin et al 2008). In Santos’s study, the total duration of
the STS movement was reported at 1.34 (±0.15) and 1.48
(±0.19) seconds for the dominant and non-dominant
sides, respectively (Santos et al 2013). In the EO and CB
group the value were less than Santos’s data. In Santos’s
study age of participants’ age were different from this
study, and then maybe this difference is related to the
age. Because, it approved that young children (12 to 18
months old) with an increase in their age, there is an
inclination toward a rise in the number of successful tri-
als and a fall in the total duration of the STS movement
(Costa & Rocha, 2013).
In the control groups of Park’s study, total duration
of STS performance was 3.13 (±0.53) seconds; the value
is signi cantly different from the present study because
Park de ned initiation of the STS from start of sacral
marker trajectory and ending of movement when all of
markers were ceased (Park et al., 2003). However, the
present study was different in de ning the start and end
point of the movement.
In this study, there was no signi cant difference
between groups at three plans in the angular velocity of
the lower extremities (Table 2). These result exhibit that
the kinematics of blind people was similar to healthy
subjects and the time of constrain of visual data does
not affect the angular velocity in children during the
STS performance. Another studies proved that the STS
movement mostly perform in the sagittal plane relative
to the other plans(Chen et al. 2013; Yoshioka et al 2012).
However, in the present study has not been observed any
signi cant differences among the three groups in the
sagittal plan. Moreover, O’Meara and et al. reported any
signi cant differences related to the angular velocity
among the groups during the STS motion in the sagittal
plan (O’Meara & Smith, 2006).
This research imposes a limitation to the time of eyes
being closed among the participants in the EC group as
the participants in this study were in their early child-
hood and tolerating having their eyes closed for lengthy
periods of time was a little hard for them. Consequently,
there were no signi cant differences among the groups
in three anatomical plans related to the angular velocity
of the lower extremities; however, all of participants had
self-selected speed for the rising from chair. It exhib-
its CNS’s congenital blind children could manage chal-
lenges of the dominant and non-dominant sides during
the STS maneuver.
REFERENCES
Burnett, D. R., Campbell-Kyureghyan, N. H., Cerrito, P. B., &
Quesada, P. M. (2011). Symmetry of ground reaction forces and
muscle activity in asymptomatic subjects during walking, sit-
to-stand, and stand-to-sit tasks. Journal of Electromyography
and Kinesiology, 21, 610–615.
Chen, T., Chang, C.-C., & Chou, L.-S. (2013). Sagittal plane
center of mass movement strategy and joint kinetics during
sit-to-walk in elderly fallers. Clinical Biomechanics, 28(7),
807–812. doi: 10.1016/j.clinbiomech.2013.07.002
Coghlin, D. S. S., & McFadyen, B. J. (1994). Transfer strategies
used to rise from a chair in normal and low back pain sub-
jects. Clinical Biomechanics, 9(2), 85-92. doi: 10.1016/0268-
0033(94)90029-9
Costa, C. S. N. D., & Rocha, N. A. C. (2013). Sit-to-stand move-
ment in children: A longitudinal study based on kinematics
data. Human Movement Science, 32, 836–846.

BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS EFFECTIVENESS OF CONSTRAINED TIME OF VISUAL DATA ON ANGULAR VELOCITY 693
Mozhgan, Faramarz and Mandana
Galli, M., Cimolin, V., Crivellini, M., & Campanini, I. (2008).
Quantitative analysis of sit to stand movement: experimen-
tal set-up de nition and application to healthy and hemiple-
gic adults. Gait & Posture, 28(1), 80–85. doi: 10.1016/j.gait-
post.2007.10.003
Held, R. (1988). Vision and Visual Systems Sensory System I
(pp. 71-73). Boston: Readings from the Encyclopedia of Neu-
roscience.
Hennington, G., Johnson, J., Penrose, J., Barr, K., McMulkin,
M. L., & Linden, D. W. V. (2004). Effect of bench height on sit-
to-stand in children without disabilities and children with cer-
ebral palsy. Archives of Physical Medicine and Rehabilitation,
85(1), 70–76. doi: 10.1016/S0003-9993(03)00407-6
Highsmith, M. J., Kahle, J. T., Carey, S. L., Lura, D. J., Dubey, R.
V., Csavina, K. R., & Quillen, W. S. (2011). Kinetic asymmetry in
transfemoral amputees while performing sit to stand and stand
to sit movements. Gait & Posture, 34, 86–91.
Holfort, S. K., Jackson, G. R., & Larsen, M. (2010). Dark adap-
tation during transient hyperglycemia in type 2 diabetes.
Experimental Eye Research, 91(5), 710–714. doi: 10.1016/j.
exer.2010.08.017
Huffman, K. D., Sanford, B. A., Zucker-Levin, A. R., Williams,
J. L., & Mihalko, W. M. (2015). Increased hip abduction in high
body mass index subjects during sit-to-stand. Gait & Posture,
41, 640–645.
Jackson, G. R., & Edwards, J. G. (2008). A short-duration dark
adaptation protocol for assessment of age-related maculopa-
thy. Journal of Ocular Biology, Diseases, and Informatics, 1(1),
7–11. doi: 10.1007/s12177-008-9002-6
Jackson, G. R., Owsley, C., & Jr, G. M. (1999). Aging and dark
adaptation Vision Research (Vol. 39, pp. 3975–3982).
Kerr, K., White, J., Barr, D., & Mollan, R. (1994). Analysis of
the sit-stand-sit movement cycle: development of a measure-
ment system. Gait & Posture, 2(3), 173-181. doi: 10.1016/0966-
6362(94)90005-1
Kerr, K., White, J., Barr, D., & Mollan, R. (1997). Analy-
sis of the sit-stand-sit movement cycle in normal subjects.
Clinical Biomechanics, 12(4), 236–245. doi: 10.1016/S0268-
0033(96)00077-0
Kerr, K. M., White, J. A., Barr, D. A., & Mollan, R. A. B. (1994).
Standardization and de nitions of the sit-stand-sit movement
cycle. Gait & Posture, 2(3), 182-190.
Manckoundia, P., Mourey, F., P tzenmeyer, P., & Papaxanthis,
C. (2006). Comparison of motor strategies in sit-to-stand and
back-to-sit motions between healthy and Alzheimer’s disease
elderly subjects. Neuroscience, 137(2), 385–392.
Music, J., Kamnik, R., & Munih, M. (2008). Model based iner-
tial sensing of human body motion kinematics in sit-to-stand
movement. Simulation Modelling Practice and Theory, 16(8),
933–944. doi: 10.1016/j.simpat.2008.05.005
O’Meara, D. M., & Smith, R. M. (2006). The effects of unilateral
grab rail assistance on the sit-to-stand performance of older
aged adults. Human Movement Science, 25, 257-274. doi:
10.1016/j.humov.2005.11.003
Park, E. S., Park, C.-i., Lee, H. J., Kim, D. Y., Lee, D. S., &
Cho, S.-R. (2003). The characteristics of sit-to-stand transfer in
young children with spastic cerebral palsy based on kinematic
and kinetic data. Gait and Posture, 17, 43-49.
Santos, A. N. d., Pava˜o, S. L., Santiago, P. R. P., Salvini, T. d. F.,
& Rocha, N. A. C. F. (2013). Sit-to-stand movement in children
with hemiplegic cerebral palsy: relationship with knee exten-
sor torque and social participation. Research in Developmental
Disabilities, 34(6), 2023-2032.
Santos, A. N. d., Pavão, S. L., Santiago, P. R. P., Salvini, a. d. F.,
& Rocha, N. A. C. F. (2013). Sit-to-stand movement in children
with hemiplegic cerebral palsy: Relationship with knee exten-
sor torque and social participation. Research in Developmental
Disabilities, 34(6), 2023–2032. doi: 10.1016/j.ridd.2013.03.021
Seven, Y. B., Akalan, N. E., & Yucesoy, C. A. (2008). Effects of
back loading on the biomechanics of sit-to-stand motion in
healthy children. Human Movement Science, 27(1), 65-79. doi:
10.1016/j.humov.2007.11.001
Seven, Y. B., Akalan, N. E., & Yucesoy, C. A. (2008). Effects
of back loading on the biomechanics of sit-to-stand motion
in healthy children. Human Movement Science, 27(1),
65–79.
Treasurer, J. W., Cox, D. I., & Wall, T. (2007). Epidemiology
of blindness and cataracts in cage reared ongrown Atlan-
tic halibut Hippoglossus hippoglossus. Aquaculture, 271,
77-84.
Yoshioka, S., Nagano, A., Hay, D. C., & Fukashiro, S. (2012).
The minimum required muscle force for a sit-to-stand task.
Journal of Biomechanics, 45(4), 699–705. doi: 10.1016/j.jbio-
mech.2011.11.054