
Health Science
Communication
Biosci. Biotech. Res. Comm. 9(4): 587-595 (2016)
Association between demographic characteristics
and health status of uninsured expatriate workers
in Saudi Arabia
Abdulwahab A. Alkhamis
1
and Shaima S. Ali Miraj
2
*
1
Supervisor Public Health Department and University Branches Department of Public Health,College of
Health Sciences, Saudi Electronic University, PO Box 93499 Riyadh,11673 Saudi Arabia
2
Assistant Professor, Department of Public Health, College of Health Sciences, Saudi Electronic University,
PO Box 93499 Riyadh, 11673 Saudi Arabia
ABSTRACT
Health insurance in Saudi Arabia is characterized by serious reforms, as the country has undergone major expan-
sion of its healthcare system. Despite enormous positive developments like introduction of compulsory health bene t
scheme for all, healthcare is still in its nascent stage in the Kingdom and little is known about user demographics
of the uninsured expatriate workers and its association with their health status. The present study has attempted to
highlight the impact of certain key demographic factors such as age, educational level, nationality and language
pro ciency on the health status of non-insured expatriates working in Saudi Arabia. A cross-sectional survey with
a multi-stage strati ed cluster sampling technique was used with veri ed questionnaires. Our ndings indicate that
important characteristics such as age, education, nationality and language, are associated with an individual’s health
status. The analysis of these demographic factors impacting health insurance of expatriates will help in determining
successful and bene cial working of health insurance and its accessibility with regard to ever increasing expatriate
participation in future.
KEY WORDS: DEMOGRAPHIC, CHARACTERISTICS, UNINSURED, EXPATRIATES, SAUDI ARABIA
587
ARTICLE INFORMATION:
*Corresponding Author: s.miraj@seu.edu.sa
Received 28
th
Nov, 2016
Accepted after revision 27
th
Dec, 2016
BBRC Print ISSN: 0974-6455
Online ISSN: 2321-4007
Thomson Reuters ISI ESC and Crossref Indexed Journal
NAAS Journal Score 2015: 3.48 Cosmos IF : 4.006
© A Society of Science and Nature Publication, 2016. All rights
reserved.
Online Contents Available at: http//www.bbrc.in/
588 DEMOGRAPHIC CHARACTERISTICS AND HEALTH STATUS OF UNINSURED EXPATRIATE WORKERS BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
Abdulwahab and Ali Miraj
INTRODUCTION
Not long ago, the World Bank supported the extension
of role of private health insurance in many developing
countries. As a result, some employers in these coun-
tries provide health insurance as a tool to attract profes-
sional workers. Saudi Arabia attracts a large number of
additional expatriates, both skilled and unskilled, in the
hope of seeking employment for nancial security. Lit-
erature suggests that expatriates have increased health
risks related to leaving their home countries, (Sekhri and
Savedoff 2005, Sommers et al 2012 and Baicker, 2013).
Of late, there has been a resurgence in the role of pri-
vate health insurance companies in providing better ser-
vices to their clients, as in most high and middle income
countries they are now required to provide supplemen-
tary or complementary coverage to primarily, social or
national health insurance systems, with the exception
of the United States, (Bassett and Kane 2007, Thomson
et al 2009, Levy and Janke 2016, Alkhamis et al 2014,
Alkhamis 2016 and Sa 2016).
In a time when global disease burden is immense,
health insurance provides valuable risk coverage against
expenditure caused by any unforeseen medical emer-
gencies. Having health insurance is important for sev-
eral reasons, though these may vary in both developed
and developing economies. It is the poor and most vul-
nerable who are at greatest risk owing to lack of protec-
tion against the impoverishing effects of illness. People
who are uninsured are more likely to have worse health
outcomes, delayed access to care and are more likely to
receive less medical care than the insured ones. Health
care providers do not care about the uninsured people
due to nancial implications (Bassett and Kane, 2007and
Thomson et al 2009).
The role of private health insurance in access to
healthcare varies among developing and developed
countries, and has been deliberated in different sur-
roundings (Thomson et al 2009; Schoen et al 2010. Dor-
herty 2011, Berkhout and Oostingh, 2008; Drechsler and
Jütting 2005; Islam 2007 and Smith, 2007).
Saudi Arabia shares characteristics of both high and
low-income countries as recently Alkhamis (2012) and
Alkhamis et al (2014) have reported. It has attempted
to seriously reform its private healthcare system and
reduce expatriate access to government resources
through the provision of Compulsory Employment
Based Health Insurance (CEBHI). CEBHI was announced
in 1999; however, it could not be implemented until
2006, when it was carried out in phases according to
company size, similar to the plan used for implementing
compulsory healthcare in Korea (Jeong and Niki, 2012).
Consequently, by November 2008, all companies had to
provide health insurance to their employees regardless
of their company’s size and could not renew their work-
ers residency permit unless they were insured (Cabinet
of Ministers, 1999). Despite widespread adoption of this
policy, employer provided healthcare is still in its nas-
cent stage in the Kingdom, knowledge of controlling
factors becomes vital to determine the successful expan-
sion of employer-provided healthcare and its funding,
(Alkhamis et al 2014, TCCHI 2009, Gallagher 2002,
Alkhamis 2016 and Sa 2016).
As there is no data-based information regarding the
demographic characteristics of uninsured expatriate
workers working in the Kingdom, the present study has
been attempted to identify the important demographic
associations of the uninsured expatriates, in context to
their health status by means of utilization of health ser-
vices by them. Lack of awareness is a major factor of the
low acceptance of health insurance. Thus, an increase in
awareness of the expatriates, with more information on
demographics, would be vital for proper dissemination
of health insurance and its associated bene ts in future.
Earlier studies elsewhere have highlighted the associa-
tion between low health literacy and age, race, language
and education, (Kunter and White 2003, Levy and Janke
2016, McCormack 2009, Paez et al 2014, Quinn et al
2000, Agency for Healthcare Research and Quality 2009,
Short 2004, The Economist 2014, Kenney et al 2010,
Health Insurance Coverage in the United States 2013).
It is pertinent to state that understanding of demo-
graphic characteristics constitutes one of the most
important pillars of any successful healthcare model.
The expatriate population in Saudi Arabia is unique
because not only does this population dominate the
private sector, but expatriates in Saudi Arabia are also
young, have limited education and face more health
problems despite having health insurance because of a
lack of awareness of its proper bene ts
United Nations,
World Population Prospects, 2008; Ministry of Labour
Riyadh, 2009 and Alkhamis et al 2014).
In this paper we present the results of a cross-sec-
tional survey conducted on a representative sample of
uninsured expatriate workers belonging to different
trades in Riyadh, the capital of Saudi Arabia. This inves-
tigation of their health insurance status along with its
associations with demographic factors was conducted
out of public interest and to gain important information
on the lacunae for low penetration of health insurance
in expatriates.
METHODOLOGY
To test the outcomes, veri ed questionnaires were given
to the uninsured expatriate population working in com-
panies representing nine different trades, namely agri-

BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS DEMOGRAPHIC CHARACTERISTICS AND HEALTH STATUS OF UNINSURED EXPATRIATE WORKERS 589
Abdulwahab and Ali Miraj
culture, mining, industry, construction, transportation,
nancial services, personal services, trade, and elec-
tricity.
All companies that provide healthcare-oriented
services such as hospitals, clinics, eye doctors, and
pharmacies were excluded. Economic sector/industry
classi cation was based on the third revision of the
International Standard Industrial Classi cation (ISIC) of
all economic activities, which has been used to stand-
ardise the collection and reporting of statistics (Ministry
of Labour Riyadh, 2009; Health Insurance Coverage in
the United States, 2013). To determine the sample size, a
multistage strati ed sampling method was used for the
employee population working in the above-mentioned
industrie
s. The study strati cation was based on busi-
ness type, company size and number of employees. The
companies’ size and economic sectors were randomly
selected from the Ministry of Labour database; these
names were concealed and coded. The code of the com-
panies was known only to the Manager of the Statistics
Department of the Ministry of Labour.
The participating companies identi ed from this
database were registered in Riyadh. Riyadh was selected
because it represented more than one third of the expa-
triate population working in Saudi Arabia (Ministry of
Labour Riyadh, 2009). It has a population of over 5.0
million, from which a total of 4,737 participants were
selected. The expatriate workers belonged to countries
from the Asian subcontinent including India, Paki-
stan, Bangladesh, Sri Lanka, and the Philippines; Arab
nations including Egypt, Yemen, and Africa; and West-
ern countries. They were selected randomly, representing
a homogenous group. The present study included only
male expatriates working in the private sector. Female
expatriates, the elderly and children were excluded from
the sample because men dominate the expatriate work-
force in the private sector (98.30% of all expatriates in
the private sector).
The questionnaire was adapted from the Medical
Expenditure Panel Survey (MEPS), and was translated
into six dominant expatriate languages, namely Urdu,
Hindi, Bengali, Malayalam, Arabic and English (Agency
for Healthcare Research and Quality, 2009). The total
sample size was 4,737, out of which 4,575 responded
to the questionnaire prepared, as per standard proto-
col of MEPS. Among the 4,575 respondents, 1,370 were
uninsured and 3,205 were insured. In the current study,
sample size of 1370 uninsured was used. The selected
questionnaire had comparable sections on parameters
representing demographic factors such as age, educa-
tion, nationality, marital status and language pro -
ciency measured for stating difference among the unin-
sured expatriate population across various segments
.
Similarly outcome measures for health service utiliza-
tion characteristics included Medicare, visit to clinic in
last one year, hospitalization in last one year or above,
reimbursement for payment made and percentage of
reimbursement to evaluate the differences among vari-
ous demographic characteristics of the uninsured sam-
ple population. In the present study, frequencies and
percentages were calculated for the responses collected
from these uninsured respondents. Statistical Package
for the Social Sciences (SPSS) software version 16.0 was
used to analyse the coded data.
RESULTS
The average age of the study population was 36 years.
It was found that an average 22.2 % of the expatriates
were less than 30 years old. The maximum number of
employees found was in age group of 31 to 40 years with
a frequency distribution of 46.3%. It was also observed
that in the age group of 50 years and older, the percent-
age of insured expatriates two times greater than that of
the uninsured (Table 1).
Comparing the categories on basis of educational
quali cation among uninsured individuals from the
sample population, it was found that 74% of the inter-
viewed people were either illiterate, had elementary
level education or had education up to higher secondary
level. In comparison people having technical diploma/
graduation or above were only 26%. The data based on
nationality demonstrated that majority of expatriates
were non-Arabs (69%) maximum being from Bangla-
desh, followed by India and Pakistan. Among the Arab
origin expatriate population, majority of them were
from Egypt, followed by Yemen (Table 1).
On analysing the criteria for language pro ciency, it
was observed that 93% of the sample uninsured popu-
lation was comfortable speaking in Arabic. Comparing
the same for English as a medium of communication,
just 33% were pro cient in it (Table 1). Comparing the
marital status among the uninsured people it was found
that 82% were married, with about 71.3% were living
without their family. The uninsured expatriates were
then compared on the basis of certain outcome meas-
ures based on the utilization of health services. The two
most important criteria among the demographical fac-
tors, age and educational quali cations were compared
to evaluate their in uence on ve important variables
representing health services utilization namely: medical
care, number of clinical visits in a year, number of hos-
pitalizations in a year, whether reimbursed for expenses
made for hospitalization and percentage of reimburse-
ment made for the same. Interesting observations were
noticed. On comparing the medical care, just 12.2% of
the subjects con rmed of seeking medical care. Among
them, 57.2% belonged to 31 to 45 years of age, followed
590 DEMOGRAPHIC CHARACTERISTICS AND HEALTH STATUS OF UNINSURED EXPATRIATE WORKERS BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
Abdulwahab and Ali Miraj
months, maximum number of visits were observed in 31
to 45 years age group, followed by younger people. Sim-
ilar trends were observed in clinical visits made between
6 to 12 months and > 1 year time period as well (Table2).
Another signi cant observation made was that
among the 1370 sample population, across all age
groups, 28.7% people af rmed on visiting clinic only
after more than one year or more. In comparison, 17.8%
visits were made between 6 to 12 months, followed by
14.3% visits made before 6 months. On evaluating the
outcome of hospitalization, it was found that 32.2%
responded to have sought it. Among them, maximum
people to have undertaken hospitalization were from 31
to 45 years (Table 2).
Similarly when evaluated for reimbursement made
for treatment, a majority of 57.6% people among the
insured sample population con rmed to have been reim-
bursed for payment made, with maximum percentage
(62.8%) being between 31 to 45 years of age. Similarly
on evaluating for percentage of payment, 57% of the
uninsured people received partial payment as compared
to full amount reimbursed for the payment made for
hospitalization/ treatment, (Table 2).
On comparing the outcome measures on the basis of
educational quali cations of the uninsured expatriates,
it was observed that 57.7% people who were hospital-
ized had up to higher secondary educational quali ca-
tions in comparison to 26.3% people hospitalized who
had higher quali cations. Comparing the same on the
basis of reimbursement made for treatment, full reim-
bursement was found in 51.3% having higher quali -
cations. Similarly even among partial reimbursement
made, 47.8% people having higher quali cation fared
better than their counterparts, (Table 3).
DISCUSSION
In the entire Middle East region, comprising of the
major six GCC countries, the evidence related to health
insurance is very scanty because of lack of research in
this area. Our study provides estimates of the impor-
tant demographic characteristics associated with the
health status of expatriates. We have tried to exam-
ine the involvement of age, quali cations, language
and nationality of the uninsured expatriates for seek-
ing health bene ts by utilization of services. Therefore,
the present work contributes signi cantly by providing
relevant information that can be used by health policy
makers. Among the uninsured sample population, the
middle-age group (30 – 50 years) was in majority rep-
resenting 73% of the sample size without having insur-
ance which interestingly was also the one having up
to secondary level (representing nearly 72%). These
lower levels of education level among these respondents
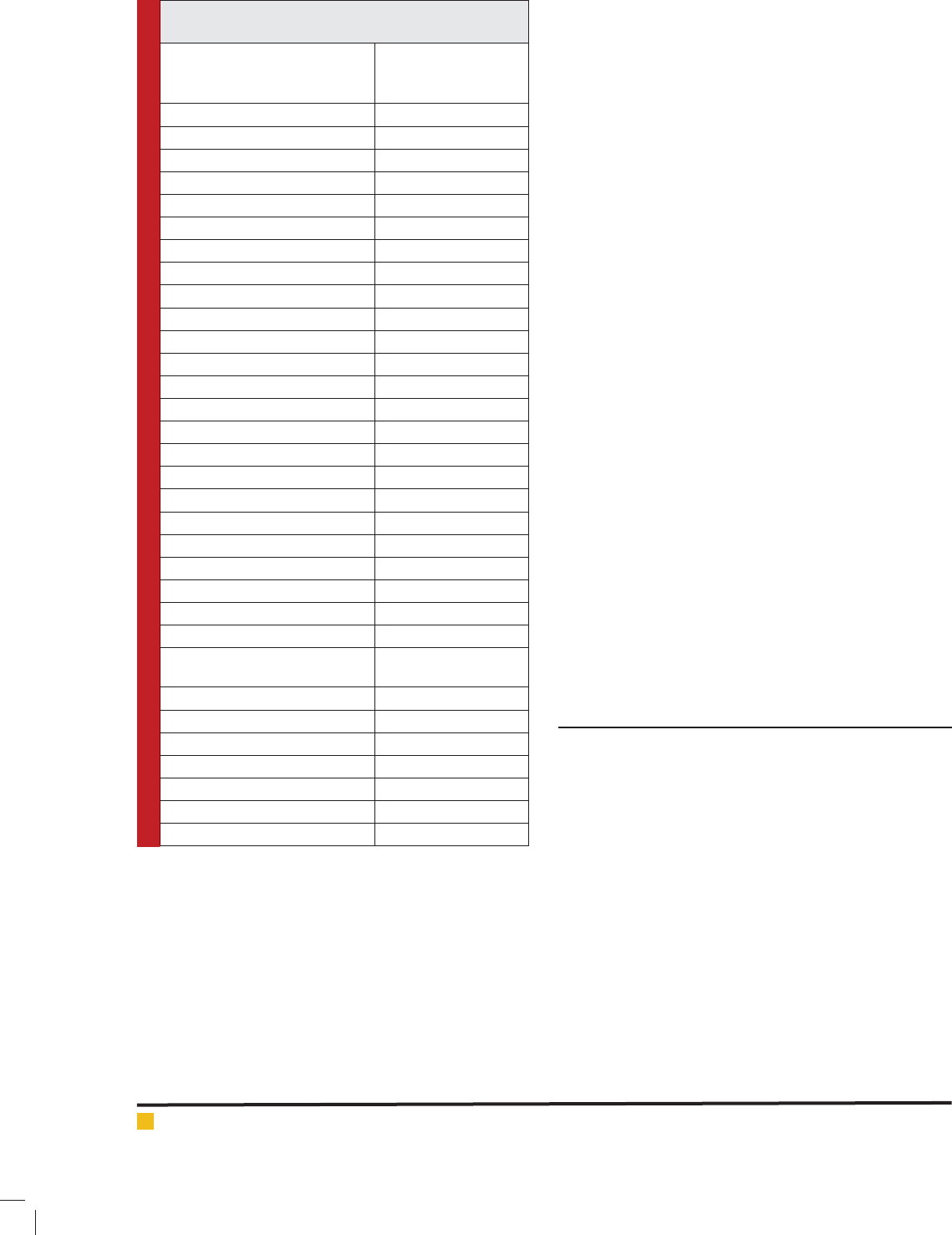
Table 1: Socio-demographic characteristics of uninsured
expatriate employees working in Riyadh, KSA.
Demographic Characteristics Uninsured
Expatriates
n = 1370
Age (in years) No. (In Percentage)
18-30 303(22.2%)
31 – 40 635(46.3%)
40– 50 367(26.8%)
51- 60 58(4.2%)
60+ 7(0.5%)
Education Level
Illiterate 14(1%)
Elementary 463(33.8%)
Up to Secondary /HS schooling 536 (39.1%)
Technical Diploma/Graduate 340 (24.8%)
Post Graduate and Above 17(1.2%)
Nationality (Non-Arab Nations)
India 351(25.6%)
Bangladesh 402(29.3%)
Pakistan 141(10.5%)
Philippines 20(1.4%)
Others 60(4.4%)
Total (In No.) 974
Arab Origin Nations
Egypt 216(15.7%)
Yemen 63(4.6%)
Other Arabs 117(8.5%)
Total (In No.) 396
Language Pro ciency
(Comfortable in conversing)
Arabic 1276 (93%)
English 451 (33%)
Marital Status
Unmarried/ Divorced/Widower 247 (18%)
Married with family in KSA 146 (10.7%)
Married without family in KSA 977 (71.3%)
TOTAL 1370
by 27.1 % people seen from the younger age group of
less than 30 years followed by 16% seen in people with
age group > 45 years (Table 2).
On evaluating frequency of visits to medical clinics in
a year, it was observed that 39% among the uninsured
sample size of 1370, never visited any clinic over one
year or more for treatment in comparison to 61% who
went to clinic to seek treatment. Comparing the same
on the basis of the age group, interesting observations
were seen. When evaluated for clinical visits less than 6
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS DEMOGRAPHIC CHARACTERISTICS AND HEALTH STATUS OF UNINSURED EXPATRIATE WORKERS 591
Abdulwahab and Ali Miraj
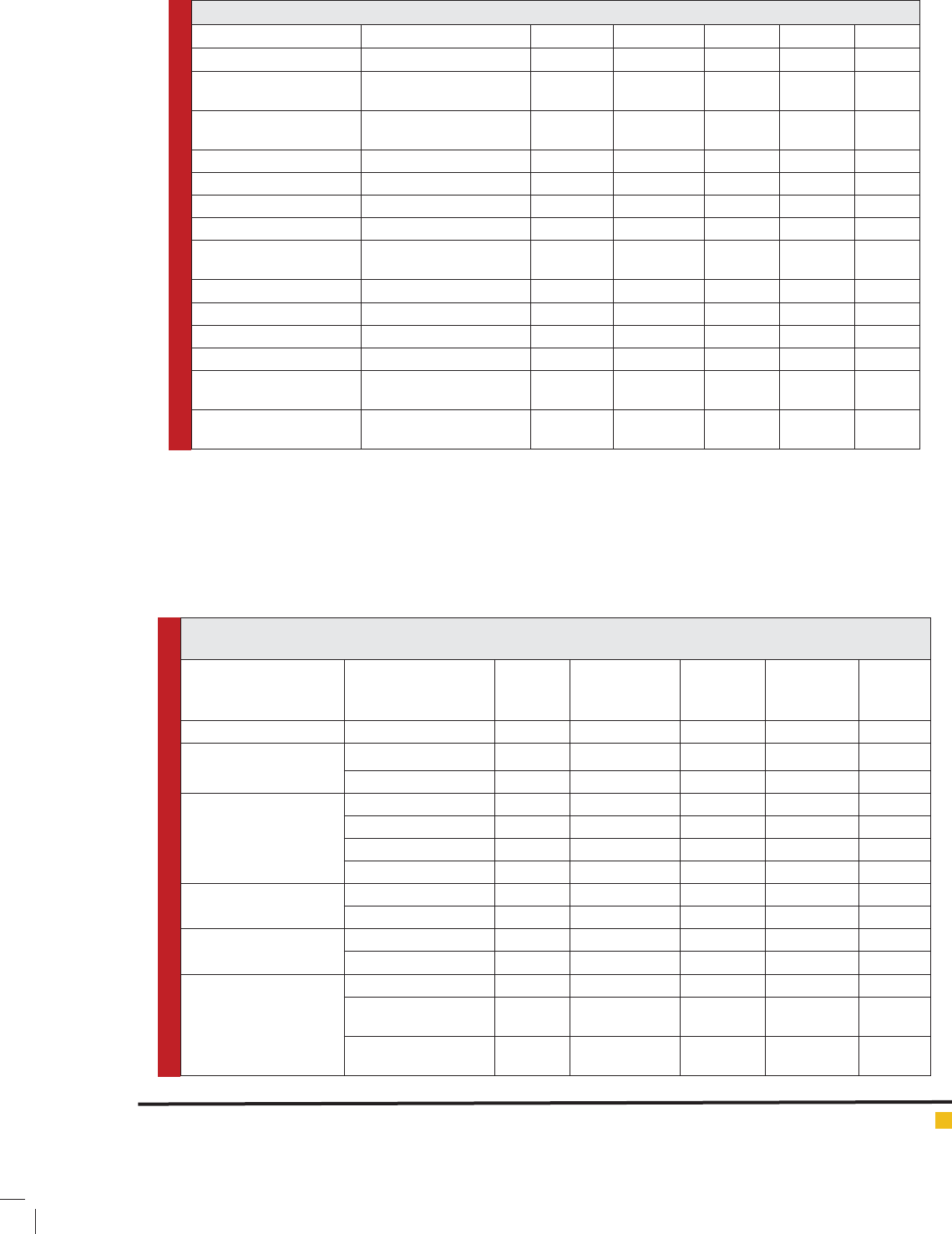
Table 2: Frequency distribution of uninsured expatriates according to age with certain outcome measures.
AGE GROUPS 18-30 31-45 45-60 >60 Total
OUTCOME MEASURES n=1370
Medical care seeked NO (87.8%) 320 (26.5%) 771 (64%) 109
(9.05%)
4 (0.33%) 1204
YES (12.2%) 45 (27.1%) 95 (57.2%) 25
(15.06%)
1 (0.60%) 166
CLINIC VISITS PER YEAR NEVER (39%) 198 (37%) 291 (54.3%) 45 (8.4%) 1 (0.1%) 535
<6 MONTHS(14.3%) 53 (26.9%) 128 (64.9%) 15 (7.6%) 1 (0.5%) 197
6-12 MONTHS (17.8%) 38 (13.93%) 176 (72.13%) 29 (11.8%) 1 (0.4%) 244
>1YEAR (28.9%) 76(19.2%) 271(68.7%) 45(11.4%) 2 (0.5%) 394
HOSPITALIZATION
PER YEAR
NO (67.8%) 274 (29.4%) 562(60.4%) 90 (9.7%) 3(0.3%) 929
YES (32.2%) 91(20.6%) 304 (68.9%) 44(9.9%) 2(0.4%) 441
REIMBURSEMENT NO (42.4%) 31(16.5%) 145(78.05%) 10(5.3%) 2(1%) 188
YES (57.6%) 60(23.7%) 159(62.8%) 34(13.4%) 0 (0%) 253
% OF REIMBURSEMENT FULL (43%) 23(21.1%) 74 (67.8%) 12(11%) 0 (0%) 109
PARTIAL (More than 50%)
(36.3%)
20(21.7%) 58(63%) 14(15.2%) 0 (0%) 92
PARTIAL (Less Than 50%)
(20.7%)
17(32.6%) 27(51.92%) 8 (15.3%) 0 (0%) 52
Table 3: Frequency distribution of uninsured expatriates according to their educational quali cations with outcome
measures.
Educational
Quali cation
Illiterate Elementary Upto HS Diploma/
Graduate &
Above
TOTAL
Outcome Measures n=1370
Medical care NO (87.8%) 10 (0.83%) 399 (33.1%) 476 (39.5%) 319 (26.4%) 1204
YES (12.2%) 4(2.4%) 64(38.5%) 60 (36.1%) 38(22.8%) 166
WENT to CLINIC in LAST
1 YEAR
NEVER (39%) 7(1.3%) 191(35.6%) 204 (38%) 134(25%) 536
<6 MONTHS(14.3%) 1(0.5%) 66(33.6%) 73(37.2%) 56(28.5%) 196
6-12 MONTHS (17.8%) 1(0.4%) 74(30.3%) 110(45.1%) 59(24.2%) 244
>1YEAR (28.9%) 5(1.26%) 132(33.5%) 149(37.8%) 108(27.4%) 394
HOSPITALIZED IN LAST
1 YEAR
NO (67.8%) 12(1.29%) 323(34.7%) 353 (37.9%) 241(25.9%) 929
YES (32.2%) 2(0.5%) 140(31.7%) 183(41.4%) 116(26.3%) 441
REIMBURSEMENT NO (42.4%) 2 (1.06%) 100 (53.19%) 58 (30.85%) 28 (14.8%) 188
YES (57.6%) 0 (0%) 87(34.3%) 94(37.1%) 72(28.4%) 253
% OF REIMBURSEMENT FULL (43%) 0 (0%) 8 (7.3%) 45(41.2%) 56 (51.3%) 109
PARTIAL (More than
50%) (36.3%)
0(0%) 22(23.9%) 26(28.2%) 44(47.8%) 92
PARTIAL (Less Than
50%) (20.7%)
0 (0%) 9 (17.3%) 32(61.5%) 11(21.1%) 52
possibly might have contributed to a reduced awareness
of healthcare options, which in turn led to their greater
percentage of population having no insurance coverage.
This probably draws attention towards two vital
issues representing, issue of health literacy and secondly
the mind-set. The issue of not seeking health insurance
which was among 22% which were less than 30 years
could be highlighted from the fact that probably, since
they been young, feel health insurance is not for them.
However, the same could not be said for the middle aged
respondents, since these people probably, avoided opt-
ing for medical care thinking that there are no issues

Abdulwahab and Ali Miraj
592 DEMOGRAPHIC CHARACTERISTICS AND HEALTH STATUS OF UNINSURED EXPATRIATE WORKERS BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
with their health, though it may be vice versa. At the
same time, stark differences in health coverage were
observed in the various age groups. In earlier studies it
has been reported that overall health care expenses and
insurance coverage, both increased with age, (Quinn et
al 2000, Short 2004 and The Economist 2014).
However, in our investigation, it was just the reverse.
Among the uninsured, even as age progressed the utili-
zation of health services did not increase. This could be
possibly due to the fact that the large number of expatri-
ates who work in the kingdom had to have sound health
to continue to work. Despite the increasing age, they
might feel no major health issues because of nancial
reasons or deliberately do not want to report. In our
analysis, it was also found that the younger age group
opted less healthcare in comparison to the middle aged.
This view is consistent with the recent research of
Levy and Janke (2016) and that of McCormack, (2009).
It has been observed that usually, young people would
think and feel to have no health issues as compared to
middle or older age groups. In our study, it was observed
that irrespective of been young, they opted for more
healthcare as compared to the older population. This
may be due to the fact that older age group being in
minority, had low health literacy; and thus probably
would have lacked adequate awareness (McCormack,
2009; Paez et al 2014, United Nations World Population
Prospects 2008).
The existing literature clearly reveals that the insur-
ance status of subjects varies by age. In an earlier study,
it was found that young adults represented the largest
percentage of Americans not covered by a health insur-
ance plan (Kunter and White 2003 and Paez et al 2014).
It was also shown by a 2004 Joint Economic Committee
study, that young adults between the ages of 18 and
24 are about 30% less likely to be insured than the rest
of the population, and the chances of being insured
increase as a person ages (McCormack, 2009)
.
According to Carper and Beauregard’s MEP survey
conducted in the United States in 2009, age plays a major
factor in whether a worker has health insurance. Young
adults aged between 19 and 23 years old were more at
risk of being uninsured than any other age group. Addi-
tionally, these investigators stated that workers under
the age of 35 were signi cantly more likely than older
workers to be uninsured all year.
Another very strong
aspect which was revealed from our study was that irre-
spective of the age, the education level of a person could
play important in uence on health insurance. The data
of the present study, with regard to educational quali -
cations, showed that70%-80% of the expatriate popula-
tion, irrespective of insurance category had completed
up to higher secondary schooling. The percentage of
illiterate participants was extremely low (<2%).
Carper and Beauregard’s report (Carper and Beaure-
gard 2009), also states that educational attainment has a
substantial impact on worker’s health insurance status.
Lower levels of education were found to be associated
with being uninsured all year in workers 19–64 years of
age or decreased utilization of health services. Workers
who had less than a high school education were about
twice as likely as those who attended at least some col-
lege to be uninsured all year. Earlier studies have found
factors affecting service utilisation ranged from cul-
tural and socio-demographic factors, physical accessi-
bility and disease patterns to perception of quality of
services and con dence in care (The Economist, 2014).
In our study the impact of educational quali cation of
uninsured expatriates was evaluated for healthcare uti-
lisation.On evaluating the data for the
reimbursement
made for treatment/hospitalization, it was found that
the percentages of reimbursement made in highly quali-
ed uninsured expatriates was signi cantly higher from
those uninsured employees having low quali cation.
Studies have revealed that the insured were more
likely to pay doctor visits when sick and use health
care in community health centres but had less visits per
episode compared with the uninsured who tended to
seek care less frequently (Short 2004 and McCormack
2009). Our study with comprehensive data using a large
number of subjects, is one of its rst in the Middle East
region to emphasize upon the point that better educa-
tion could signi cantly in uence health insurance reim-
bursements.
The nationality of the expatriates was yet another
distinguishing factor for assessing the impact of demo-
graphic factors on the issue of accessing healthcare. It
was found that out of the total 4,575 expatriate workers
interviewed, a majority of 69% belonged to the South-
east Asian community, comprising Bangladesh (25.3%),
followed by India (24%), and Pakistan (10.9%).
We speculate that when the economy deteriorates,
expatriate in ltration increases. To remain in the earn-
ing country, expatriates are forced to shell out health
premiums regardless of need. It may be mentioned that
the high-quality facilities available, to expatriates in the
Kingdom, are in contrast to the major health disparities
in quality of healthcare, which have been reported to
exist between migrant workers and the local population
elsewhere, (Altijani and Ali, 2010).
In the present study, it was also observed that out of
the 1,370 uninsured respondents a staggering 71% of
non-Arab nationals were found to be uninsured com-
pared with the 33% of Arab-based nationals (i.e., Egypt,
Yemen) seen under insured category. These data show
that there is still need for further development and dis-
tribution of affordable health insurance plans so that
healthcare options are bene cial for both the insured
Abdulwahab and Ali Miraj
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS DEMOGRAPHIC CHARACTERISTICS AND HEALTH STATUS OF UNINSURED EXPATRIATE WORKERS 593
and the insurer. In the present study, analysis of the lan-
guage pro ciency variable revealed that irrespective of
nationality or insurance status, 89.6%–93% of the sub-
jects had pro ciency in the Arabic language, whereas
among the insured the majority of respondents (61%)
were pro cient in English. Existing literature shows that
effective communication with patients and healthcare
workers is a key part of safe and high-quality healthcare.
Cultural misunderstanding between patients and pre-
dominantly expatriate healthcare providers is another
factor contributing to patient dissatisfaction and poor
quality of care, (Altijani and Ali, 2010 and Kronfoll
2012).
In the present study, it was also observed that because
both native and expatriate subjects had good knowledge
of both the major working languages of the Kingdom,
Arabic and English, there was no reported experience of
a language barrier. Thus, in our study language was not
an issue in selecting healthcare as majority of the expa-
triates had good command of Arabic, the main language
of communication, which is in contrast to the results of
most similar studies, especially in countries that have
a large number of expatriate healthcare workers. These
expatriates faced language problems due to not being
comfortable in the local language.
A recent review concluded that healthcare provid-
ers such as nurses and their patients experience serious
language and communication barriers (Schyye, 2007).
The results of the above-quoted study show a communi-
cation issue between patients and healthcare providers;
however, as there have not yet been studies of the lan-
guage issues between the health insured and the insur-
ers, our study is one of the few reports, where the in u-
ence of language on obtaining health insurance among
expatriates can been seen. The present data demonstrate
that because of the language pro ciency of the subjects,
there were no communication issues when obtaining
health insurance.
On evaluating the demographic factors that could pre-
dominantly in uence decision making among the unin-
sured expatriates for not procuring health insurance, it
was found that a majority (47.3 %) did not have working
permits (iqama) and felt that the only purpose of health
insurance was to renew these permits. This awed per-
ception, in which there is little value in obtaining health
insurance, alarmingly defeats its purpose, especially in
an expatriate-dominant country.The above ndings pos-
sibly also re ect the de cient understanding of health
insurance and its bene ts among the interviewed unin-
sured respondents. Thus, when choosing health insur-
ance, expatriates most value employment aspects, such
as renewal of iqama, cost and money-saving, followed
by coverage bene ts, with regard to health awareness,
knowledge and its bene ts.
These data are in conjunction with those of (Altijani
and Ali 2010 and Kronfoll, 2012), who have reported that
the expatriate population in Arab countries faces sig-
ni cant dif culty in accessing health services. Although
access has increased, the quality of the services provided
remains low, mostly owing to expatriates’ view of health
insurance as an unnecessary expenditure. Thus, within
our study sample, age, education and nationality are a
signi cant in uence on whether a person is enrolled
in a health insurance plan. This implies that the young
adults we studied did not generally opt health insurance
because they believed they did not need it possibly due
to their young age and perception of not requiring the
insurance for saving money.In addition, there are other
in uencing factors, such as new health insurance sec-
tors that are still under development, which will provide
expatriates with more choices in the future (Gallagher,
2002; Alkhamis, 2016 and Sa , 2016).
LIMITATIONS OF THE STUDY
This study had some limitations. It represented only male
expatriates and excluded females, the elderly and chil-
dren. The reason for excluding female expatriates was
that their number was limited and represented only 1.7%
of the expatriate population (98.3% are male) (Ministry
of Labour, 2009). Therefore, if female expatriates were to
be included as one of the study variables, it would have
been very dif cult to obtain a suf cient number of par-
ticipants. As the expatriates are not allowed to keep their
parents, the exclusion of the elderly was justi ed. More-
over, since this study is a cross sectional study, which
may have increased bias with respect to time ordering
of events.
CONCLUSION
Providing appropriate healthcare services for a growing
young population, inclusive of locals and expatriates,
is one of the emerging priorities of Saudi Arabia. Exist-
ing disparities between different groups of expatriates
can be addressed using this demographic pro le and its
association with health insurance status. Our ndings
indicate that expatriates’ health insurance status is con-
siderably impacted by several important demographic
characteristics such as perceived need, perceived value
related to age, sex, education level, socioeconomic sta-
tus, nationality and language. However, as there is great
scope for further development and creation of affordable
health insurance plans bene cial for both the insured
and the insurer, we recommend further, detailed studies,
which might have bearing on the health of expatriates in
light of upcoming health insurance sectors.

Abdulwahab and Ali Miraj
594 DEMOGRAPHIC CHARACTERISTICS AND HEALTH STATUS OF UNINSURED EXPATRIATE WORKERS BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS
This work was supported by the King Abdullah Inter-
national Medical Research Centre under grant number
RC09/084, upon the recommendation of the Research
Committee following the review of the Institutional
Research Board on the ethical aspects of the proposal.
CONFLICT OF INTEREST
The authors do not have any con ict of interest.
REFERENCES
Agency for Healthcare Research and Quality, Medical Expend-
iture Panel Survey -Healthcare Questionnaire. 2009 (http://
www.meps.ahrq.gov/mepsweb/survey comp/survey.jsp)
Alkhamis A. (2012) Health care system in Saudi Arabia: An
overview. Eastern Mediterranean Health Journal 18(10): 1078-
1079.
Alkhamis A.A., A. Hassan and P. Cosgrove (2014) Financing
healthcare in Gulf Cooperation Council countries: a focus on
Saudi Arabia International Journal of Health Planning and
Management 29, e64-e 82
Alkhamis AA (2016) Framing Health policy in the context of
Saudi Arabia Journal of Infection and Public Health 9, 3-6
Almutairi KM. (2015) Culture and language differences as a
barrier to provision. Saudi Medical Journal 322: 444 – 445
Alsaedi Y. (2011) Fake health insurance in order to legalize
your residency permit, in AL Madinah Newspaper 2011; Alma-
dinah Al Madinah
Altijani HH; Ali FM. (2010) Examining Equal Access to Health-
care among Nationals and Expatriates: Evidence from Qatar’s
World Health Survey SSRN 1-30.
Baicker K. (2013) The Oregon experiment-effects of Medic-
aid on clinical outcomes. New England Journal of Medicine
368(18), 1713-1722.
Bassett M.C. and V.M. Kane (2007) Review of the Literature
on Voluntary Private Health Insurance, in Private Voluntary
Health Insurance in Development Friend or Foe?, A.S. Preker
and M.C. Bassett, Editors Washington D.C. 335.
Berkhout E. and H. Oostingh (2008) Health insurance in low-
income countries: Where is the evidence that it works? Joint
NGO Brie ng Paper 112: 28.
Cabinet of Ministers, Cooperative Health Insurance Law, in 71
Dated 9th of August 1999, Council of Ministers, Editor. 1999,
Um Al Gorah, Makha Al Mukaramh.
Carper K. and Beauregard K. (2009) Characteristics of Unin-
sured Workers: Estimates for the U.S. Civilian Non institu-
tionalized Population 19–64 Years of Age, 2006 Medical
Expenditure Panel Survey Statistical Brief No. 257 (Aug 2009)
1-8.
Dorherty J. (2011) Expansion of the private for pro t health
sector in East and Southern Africa, in EQUINET, with UCT HEU
and TARSC Policy 26.
Drechsler D. and J.P. Jütting (2005) Private Health Insurance
in Low and Middle-Income Countries: Scope, Limitations, and
Policy Responses OECD Development Centre 67.
Gallagher EB (2002) Modernization and health reform in Saudi
Arabia, Chapter 4. In: Twaddle AC, ed. Health care reform
around the world. London, Auburn House181–197.
Health Insurance Coverage in the United States (2013) http://
www.census.gov/in
Islam, M. (2007) Health Systems Assessment Approach: A
How-To Manual. U.S. Agency for International Development
in collaboration with Health Systems 20/20 Management Sci-
ences for Health: Arlington, VA.
Jeong, H.S. and R. Niki (2012) Divergence in the development
of public health insurance in Japan and the Republic of Korea:
A multiple-payer versus a single-payer system. International
Social Security Review 65(2): 51-73.
Kenney G, Pelletier J and Blumberg L. (2010) How Will the
Patient Protection and Affordable Care Act of 2010 Affect
Young Adults? The Urban Institute Press
Khouja T. (2013) Reform of nancing healthcare services in the
GCC: Focus on establishing health insurance system in KSA
University of Pittsburgh 1- 41.
Kriss J. Sara R Collins, B. Mahato, E. Gould and Cathy Schoen
(2008) Rite of passage? Why young adults become uninsured
and how new policies can help, Commonwealth Fund Pub 1139
Vol. 38 1-26
Kronfoll N M.(2012) Access and barriers to health care deliv-
ery in Arab Countries: a review Eastern Mediterranean Health
Journal Vol 18 No.12, 1239-1246
Kutner M. and S.White (2006) The Health Literacy of America’s
Adults: Results from the 2003 National Assessment of Adult
Literacy. NCES National Center for Education Statistics 483.
Levy H. and A. Janke (2016) Health Literacy and Access to
Care. Journal of Health Communication 21(sup1): 43-50.
McCormack L. (2009) Health Insurance Literacy of Older
Adults. Journal of Consumer Affairs 43(2): 223-248.
Ministry of Labour.The Annual Statistical Book for One Year
2009, in The Annual Report, M.O. Labour, 2009;Editor Ministry
of Labour: Riyadh.
Ministry of Labour Saudi Labour Market Indicators, Riyadh
Region, Ministry of Labour, Editor. Ministry of Labour Riyadh.
2009; 124.
P
aez, KA.
CJ Mallery,H.J. Noel C Pugliese (2014)
Development
of the Health Insurance Literacy Measure (HILM): Conceptu-
alizing and Measuring Consumer Ability to Choose and Use
Private Health Insurance. Journal of Health Communication
19(Sup 2): 225-239.
Quinn K, Schoen C, Buatti L.(2000) On Their Own: Young
Adults Living Without Health Insurance safety in health care
2000
Sa O. (2016) The challenges for Saudi Arabia healthcare
system Indian Journal of Applied Research Vol 6, No.5 231-
233

Abdulwahab and Ali Miraj
BIOSCIENCE BIOTECHNOLOGY RESEARCH COMMUNICATIONS DEMOGRAPHIC CHARACTERISTICS AND HEALTH STATUS OF UNINSURED EXPATRIATE WORKERS 595
Schoen, C.R Osborn,D. Squires,M. M. Doty (2010) How health
insurance design affects access to care and costs, by income,
in eleven countries. Health Affairs Project Hope 29(12) 2323-
2334.
Schyve PM. (2007) Language differences as a barrier to qual-
ity and safety in health care. Journal of General Medicine 22,
2:360-361
Sekhri N. and W. Savedoff (2005) Private Health Insurance:
Implications for Developing Countries. Bulletin of the World
Health Organization 83: 8
Short P. (2004) Counting and characterizing the uninsured. In:
Mc Glaughlin C, Ed. Health policy and the uninsured. Wash-
ington DC The Urban Institute Press
Smith, P.C.(2007) Provision of a Public Bene t Package along-
side Private Voluntary Health Insurance in private Voluntary
Health Insurance in Development Friend or Foe?, Editors: A.S.
Preker, R.M. Schef er and M.C. Bassett Washington DC 147-
167
Sommers B.D., K. Baicker and A.M. Epstein (2012) Mortality
and access to care among adults after state Medicaid expan-
sions. New England Journal of Medicine, 367(11) 1025-1034.
Stewart M. (2001) Towards a global de nition of patient cen-
tred care British Medical Journal 322,445-446.
The Council of Cooperative Health Insurance, Regulations for
Cooperative Health Insurance System, Insurance, Editor (2009)
The Council of Cooperative Health Insurance Riyadh.
The Economist, Intelligence Report Health Care in Saudi Ara-
bia (2014)
(http://www.eiuperprspectives.economist.com/
healthcare/ Saudi Arabia)
Thomson S.T., Foubister J. and E. Mossialos (2009) Financ-
ing health care in the European Union: Challenges and policy
responses in European Observatory on Health Systems and
Policies World Health Organization: Copenhagen. p. 200
United Nations (2008) World Population Prospects. The 2008
Revision in World Population Prospects: Population Division,
Editor. Department of Economic and Social Affairs New York 87.